Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
20 Cards in this Set
- Front
- Back
|
PNF has 6 objectives:
|
to increase strength
to increase flexibility to increase ROM (applied passively, assisted, actively, or with resistance) to increase coordination to increase balance to decrease pain *used in therapeutic exercise |
|
|
GOALS:
|
restore of enhance the postural response and or normal pattern of motion in a functional manner
direct - focusing on target muscle indirect - more related to the synergists or antagonist muscle group |
|
|
PNF is based on 3 principles:
|
- successive induction - contraction of one muscle followed by its antagonist. e.g. contract stronger extensors to warm up before using weaker flexor group.
- reciprocal inhibition - contraction of one muscle while its antagonist is relaxed, allowing a joint to move. e.g. actively contract biceps to inhibit triceps. - process of irradiation - is when maximal contraction of a muscle recruits the help of additional muscles. e.g. for a stroke pt return happens proximal to distal, so facilitate movement at shoulder to get some overflow into the hand. |
|
|
Basic Levels of Progression:
|
1. Mobility – in a gravity-reduced position we learn the movements
2. Stability – learn how to statically hold a position against gravity 3. Controlled mobility – hold a position and moving against gravity 4. Skill – refined movement |
|
|
Agonists & Antagonists
|
Agonists - directions that is being performed by that muscle
Antagonists - direction that is being performed in relation to the opposing muscle |
|
|
Main Components of PNF:
|
- flexion or extension
- toward or away midline - rotation *based on 3 dimensions - not cardinal planes |
|
|
PNF Diagonal 1 - Upper Extremity (D1)
|

D1 Flexion - flexion/adduction/external rotation with wrist & finger flexion/RD (start in extension position)
D1 Extension - extension/abduction/internal rotation with wrist & finger extension/UD (start in flexion position) |
|
|
PNF Diagonal 2 - Upper Extremity (D2)
|
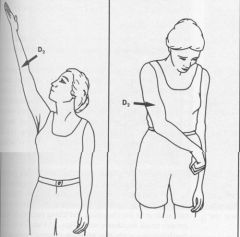
D2 Flexion - flexion/abduction/external rotation with wrist & finger extension/RD (start in extension position)
D2 Extension - extension/adduction/internal rotation with wrist & finger flexion/UD (start in flexion position) |
|
|
D1 Analogy
D2 Analogy |
D1 F - reaching across to grab seatbelt
D 1 E - pushing something down & away from you D2 F - “Y” of YMCA song D2 E - buckling seatbelt when riding shotgun |
|
|
Line of Movement
|
rotation is the initiating movement, then the other 2 components are initiated.
|
|
|
Isotonic/Isometric/Eccentric Defintions
|
Isotonic - tension remains unchanged and muscle length changes
Isometric - muscle length remains unchanged Eccentric - muscle length elongates |
|
|
Stretch
|
stimulus - muscle responds with greater contraction force when put in a stretched position due to increased surface area
response - quick stretch elicits a response when placed beyond point of tension |
|
|
Manual Resistance
|
should demand sufficient resistance
allow full ROM to be completed shouldn’t break patients movement shouldn’t elicit Valsalva Maneuver |
|
|
Joint Facilitation
|
traction - separating the joints (promotes mobility)
approximation - applying a weight bearing force on joints via compression (promotes stability) |
|
|
Agonist Contraction
|
HR or CR done, then pt moves limb into new range actively. Called HR-AC or CR-AC.
|
|
|
Rhythmic Initiation
|
sequence passive - active-assisted - active - resisted (make sure they are doing correct movements hands off. Used for patients having difficulty initiating movement (e.g. Parkinson’s patients). Allows the patient to understand the proper movement that is expected of them.
|
|
|
Hold-Relax
|
directed towards “tight” antagonist, isometric. (E.g. pt holds antagonist isometric, then PT passively moves pt further in range). “hold, hold, push into me”
|
|
|
Contract-Relax
|
directed towards “tight” antagonist, isotonic. (E.g. pt performs isotonic contraction of antagonist against resistance from the PT, then PT passively moves them further into the range). “push, push, push”
|
|
|
Testing Stability
|
- Alternating Isometrics (AI) – PT gives resistance alternating F/E, add/abd, ER/IR to get pt to do isometrics of m across the jt
- Rhythmic Stabilization (RS) – next step after AI, promotes co-contraction of m around a jt. PT provides stimulus similar to AI but less predictable. pt has to be ready for anything. |
|
|
Testing Strength
|
- Repeated Contractions (RC) if want to work on shoulder flexion, start in D2E, pt actively brings it into D2F (can be against resistance), relaxes, passively brought back down to D2E by PT, repeat. (apply resistance in one direction repeatedly)
- Agonist Reversal (AR) – aka slow reversal (SR), start c antagonist pattern first, then perform agonist pattern. Successive induction concept. (e.g. resist F, then resist E. Start c antagonist first to warm up the agonist/apply resistance in both directions) |