![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
53 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
MUSCLES JOINTS AND MOVEMENTS |
bones can move in relation to one another at joints. Ligaments join bone to bone, made up of elastic connective tissue. They hold bones together and restrict the amount of movements possible at a joint. tendons non elastic fibrous tissue joining muscle to bone. |
|
|
|
PARTS OF A JOINT |
tendon- muscle to bone ligament- bone to bone fibrous capsule- encloses the joints muscle synovial membrane- secretes s fluid synovial fluid- lubricant Cartilage- absorbs shock, absorbs synovial fluid Pad of cartilage- additional support Bone |
|
|
|
How joints work |
Skeletal muscles are those attached to bones and are normally arranged in antagnostic pairs. This means a pair of muscles that pull in oppostie directions. FLEXOR - contracts to bend a joint (biceps) EXTENSOR - contracts to extend or straighten a joint (triceps) |
|
|
|
SKETELTAL MUSCLE |
Skeletal muscle made up of billions of muscle cells known as bundles of muscle fibre. muscle cell few cm long and contains many nuclei. muscle cells contain myofibrils, that are made up of a fibrous tissue called actin (thin filament) and sarcolema. The SARCOPLASMIC RETICULUM specialised endoplasmic reticulum, stores and releases Calcium ions. specialised synapse between muscle and neurons are called NEUROMUSCULAR JUNCTION. |
|
|
|
MISTAKE! |
myofibrils contains fibrous protiens such as Actin (thin filaments) and Myosin (thick filaments). SARCOLEMMA IS THE CELL SURFACE MEMBRANE OF THE MUSCLE CELL. |
|
|
|
The sliding FILAMENT THEORY |
The functional unit of a muscle fibre is called a sarcomere. When a muscle contracts the thin actin filaments move in between the thick myosin filaments, this shortens the length of the sarcomere. Therefore shortening the length of the muscle. |
|
|
|
SARCOMERE MUSCLE CONTRACTION |
|
|
|
|
SLIDING THEORY PART 2 |
Myosin filaments have flexible heads and so change orientation, bind to an actin filament and Hydrolyse ATP using ATPase. Actin filament contains two protiens called troponin and tropomysin that control the binding of the actin to the myosin head. |
|
|
|
Nerve impulse part (SLIDING FILAMENT THEORY) |
When a nerve impluse arives at a neuromuscular junction, calcium ions are released from the sarcoplasmic reticulum and the following things take place to lead to a muscle contraction. |
|
|
|
PART 1 how muscles contract |
Ca ion attaches to the troponin causing it to move together with the threads of tropomyosin. MYOSIN BINDING SITES BLOCKED BY TROPOMYOSIN. MYOSIN HEAD CANNOT BIND. |
|
|
|
PART 2 |
Myosin binding sites on the actin are now exposed so myosin forms cross bridges with the actin filament. Myosin heads release the ADP and Pi and change shape as a result = the power stroke. |
|
|
|
PART 3 |
ATP binds to the myosin causing it to detach from thw actin. ATP hydrolysis by ATPase Myosin head returns to upright position. |
|
|
|
HOW ACTIN MOVES IN MYOSIN (SARCOMERE SHORTENING) |
1) Ca ions released from sarcomere binds to the troponin and this changes the shape of the troponin. 2) tropomyosin moves away from the myosin binding sites on actin. Allowing the myosin head to bind to the actin. 3) Myosin head must be activated for a cross bridge cycle to begin 1- ATP binds to the myosin head (ATP hydrolyses and releases energy) gives myosin head the energy to move into cocked position. |
|
|
|
PART 2 |
activated myosin head binds to actin forming cross bridge. Inorganic phosphate released bond between m and a stronger. POWER stroke- ADP released sliding myosin filament towards the centre of the sarcomere. *another ATP binds to myosin head the bond between ATP and the myosin head weakens myosin head detaches * ATP hydrolysis -activates myosin head again. * as long as binding sites on actin remain exposed cross bridge cycle repeats. * ends when Ca ions are actively transported back into the sarcoplasmic reticulum |
|
|
|
CHARACTERISTICS OF SLOW TWITCH |
1) specialised for slower and sustained contraction - can cope with long prriods of exercise. 2) Lots of mitochondria- ATP supplied by aerobic respiration ( e transport chain) 3) lots of myoglobin store lot of oxygen and a lot of capillaries for o2 suply 4) low glycogen levels and creatine phosphate 5) Fagtigue resistant |
|
|
|
FAST TWITCH CHARACTERISTIC |
1) specialised to produce rapid, intense contractions in short bursts 2) Less mitochondria- ATP provided by anerobic respiration (glycolysis) 3) little myoglobin and few capillaries (lighter colour) 4) more glycogen and creatine phosphate |
|
|
|
Energy and role of ATP in respiration |
all living organsims must respire there are 2 types. AEROBIC (with o2) - SYMBOL EQUATION. (+ 30 ATP) glucose + oxygen --> CO2 AND H2O ANEROBIC glucose --> 2C6H3O6 + 2ATP |
|
|
|
STRUCTURE AND FUNCTION OF ATP |
ATP = cells energy currency - ADP needs energy to add on another phosphate group and makes ATP. (CONDENSATION). energy is released when ATP is hydrolysed. this energy is used in energy requiring processes in the cell. ATP + H20 (equilibrium sign) ADP + Pi + energy released. |
|
|
|
FATE OF H ATOMS - ELECTRON TRANSPORT CHAIN |
H atoms released during glycolysis, the link reaction and the krebs cycle are taken up by co enzymes. For most ots NAD the hydrogen acceptor. kreb cycle = one step FAD when a coenzyme accepts H the coenzyme is reduced. coenzyme shuttles the hydrogen atoms to the electron transport chain on the mitochondrial onner membrane . H seperates to H+ and e-. With the e moving through carrier protiens in the mitochondrial inner membrane. |
|
|
|
Electron carrier Chain |
1) Reduced coenzyme carries the H+ and e- to electron transport chain in inner m membrane 2) electrons passed on throufh carrier protein redox as gain and lose e-. 3) H+ moving out from the inner m membrane to the intermembrane space. 4) H+ diffuses back into mitochondrial matirix due to down electrochemical gradient 5) the diffusion in 4 allows ATPase to catalyse ATP synthesis 6) H+ and e- join to form h atoms react with oxygen to form water. no oxygen no electron transport chain working and ATP synthesis stops |
|
|
|
AEROBIC RESPIRATION |
stage 1) glycolysis stage 2) LINK REACTION 1) pyruvate is decarboxylated and dehydrogenates 2) NAD is reduced it collects hydrogen changing pyruvate to acetate 3) acetate is combined with coenzyme A (transfers acetate to molecules) to form acetyl coenzyme A 4) NO ATP PRODUCED |
|
|
|
LINK REACTION HAPPENS TWICE FOR ONE GLUCOSE MOLECULE |
FOR EVERY GLUCOSE MOLECULE. two pyruvate molecules are made for every glucose molecule that enters glycolysis. so that means link reaction and kreb cycle happen twice for each molecule. two molecules of acetyl coenzyme A go into kreb cycle Two Co2 are released as a waste of respiration Two molecules of reduced NAD are formed and go on to the last stage oxidative phosphorylation. |
|
|
|
THE KREB CYCLE (PRODUCES REDUCED COENZYMES AND ATP) |
redox reactions that take place in the matrix, the cycle takes place twice. 1) Acetyl CoA from the link reaction reacts with oxaloacetate (4C) to form citrate. 2) Coenzyme A goes back to the link reaction to be used again 3) the 6C citrate converted to a 5C molecule by decarboxylation (CO2) and also Dehydrogenation (2H) 4) H used to form NADH from NAD |
|
|
|
KREB PART 2 |
The 5C molecule converted to a 4C molecule by decarboxylation. dehydrogenation also occurs forming one molecule of FADH and 2 NADH ATP produced by the direct transfer of a phosphate group from an intermediate to ADP. (SUBSTRATE LEVEL PHOSPHORYLATION) 4C is now oxaloacetate |
|
|
|
Respirometers and Anarobic respiration |
1) doesn't involve oxygen so no link reaction, kreb cycle or oxidative phosphorylation. 2) type of anaerobic respiration = lactate fermentation (some bacteria/animals) 4) Glucose converted to pyrovate via glycolysis --> Reduced NAD from gltcolysis transfers H to pyrovate to form lactate and NAD 5) NAD reused in glycolyisis 6) The production of lactate generates NAD. this means glycolyisis continues with no o2 around so small amount of ATP can be used. |
|
|
|
2 ways LACTIC ACID REMOVED |
After a period of anerobic respiration lactic acid builds up. Breakdown: 1) Cells can convert it back to pyruvate (used in aerobic respiration in the kreb cycle) 2) Liver cells can convert it back to gluvose can be used for respiration or stored. |
|
|
|
ELECTRICAL ACTIVITY IN HEART |
Cardiac muscle - myogenic doesn't need any neurone signals 1) SAN in right atrium wall - sends out regular waves of electrical impulses across the left and right atria 2) the non conducting collagen tissue prevents this wave from spreading into the ventricles 3) instead SAN sends the wave impulse to the AVN. 4) The AVN send out the electrical impulse to the bundle of His (but delay waiting for the atria to finish contracting) 5) The bundle of His group of muscle fibres is responsible for conducting the waves of electrical impulse to finer muscle fibres in the right and left vetrical walls called Purkyne fibres 6) they carru impulse into muscular walls of ventricles causing them to contract simultaneously, from the apex upwards |
|
|
|
ELECTROCARDIOGRAPH - Records electrical activity of heart using electrodes |
checks heart functions records electrical activity of the heart the heart depolarises when it contracts and repolarises when it relaxes 1) P wave - when the atria contracts (depolarises) 2) QRS wave - when the ventricles contract (3 parts) depolarises 3) T wave - when the ventricles relax repolarise |
|
|
|
DOCTORS USE ECGs TO DIAGNOSE HEART CONDITIONS: |
compare it to a normal trace. Problems with heart rhythem = cardiovascular disease. How to work out rate: 8 beats in 4 seconds - how many times does 4 go in 60 = 15 then 8*15 = 120bpm Tachycardia increased heart rate- 120bpm can be a sign of heart failiure heart can't pump blood efficiently and therefore heart beat increases in rate so it can supply cells with oxygen |
|
|
|
DOCTORS USE ECGs TO DIAGNOSE HEART CONDITIONS: |
compare it to a normal trace. Problems with heart rhythem = cardiovascular disease. How to work out rate: 8 beats in 4 seconds - how many times does 4 go in 60 = 15 then 8*15 = 120bpm Tachycardia increased heart rate- 120bpm can be a sign of heart failiure heart can't pump blood efficiently and therefore heart beat increases in rate so it can supply cells with oxygen |
|
|
|
part 2 |
PROB WITH AVN Some p waves are not followed by QRS waves, pulses not travelling from SAN to AVN |
|
|
|
Fibrillation |
irregular both atria and ventricles not contracting properly Atria fibrillation- chest pain, fainting and an increased risk of stroke. ventricular fibrillation- cause heart attack or death |
|
|
|
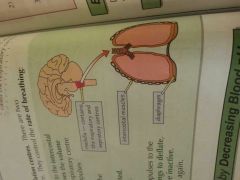
VARIATIONS IN HEART BEAT AND BREATHING RATE |
depends on activity, excersize increases heart rate. does this by: 1) increasing breathing rate and depth- takes in more oxygen and releases carbon dioxide 2) increasing heart rate- delivering oxygen and glucose to cells faster and removing CO2 faster by the muscle cells respiring and therefore being able to contract |
|
|
|
MEDULLA |
the medulla Is a parr in the brain that has ventilation centres to control breathing 2 types Inspiratory and Expiratory. |
|
|
|
MEDULLA |
the medulla Is a parr in the brain that has ventilation centres to control breathing 2 types Inspiratory and Expiratory. |
|
|
|
Inspiratory centre in the medulla sends nerve impulses to the intercostal and diaphragm muscles, makes the contract = lower pressure and the pressure difference between the air and the lungs leads to an increase in air in the lungs. the inspiratory centre also sends nerve impulses to the expiratory centre. These impulses inhibit the action of the expiratory centre. |
|
|
|
|
3) As the lungs inflate the stretch receptors are activated send impulses to the mudella and this inhibits the activity of the expirotory centre |
The inspiriatory centre no longer inhibited then sends impulses to the diaphram and intercostal muscles to relax. Causes lungs to deflate expellomhy air. As the lungs deflate, the stretch receptors become inactive. The expiratory centre is no longer inhibited and the cycle happens again. |
|
|
|
Exercise Triggers an increase in breathing rate by decreasing blood PH |
1) During exercise, level of CO2 in the blood increases. This decreses the Ph of the blood. 2) there are chemoreceptors (receptors that sense chemicals) in the medulla aortic bodies and carotid bodies that are sensitive to a change in PH 3) if the chemoreceptors detect a decrease in blood PH, they send nerve impulses to the medulla, which sends more never impulses to the diaphragm and intercostal muscles. increasing the rate and depth of breathing. 4) Causes gaseous exchange to speed up Co2 level drop and extra O2 SUPPLIED TO CELLS |
|
|
|
Ventilation rate increases with exercise |
1) Ventilation rate is the volume of air breathed in or out in a set timw 2) increases during exercise because breathing rate and depth increases |
|
|
|
The Medulla Controls heart rate too |
Heart rate is controlled by the cardiovascular control centre in the medulla of the brain: DECREASE IN BLOOD pH 1) A decrease in blood pH detected by chemoreceptors and this sends nerve impulses to the medulla 2) The medulla sends nerve impulses to the SAN to increase heart rate. |
|
|
|
Increase blood pressure leads to a decrease in heart rate |
1) Pressure receptors in the atria walls and the carotid sinuses detect changes on blood pressure 2) if too high pressure receptors send nerve impulses to the cardiovascular centre which sends nerve impulses to the SAN to slow down heart rate 3) if too low same happens but the SAN slows down heart rate |
|
|
|
Cardiac output |
Cardiac output is the total volume of blood pumped by a ventricle every minute. CARDIAC OUTPUT (CM3/Min) = heart rate X stroke volume output increases because the heart rate increases (stroke volume also increases because the heart pumps harder as well). So cardiac output increases because the heart rate increases (stroke volume also increases because the heart pumps harder as well). stroke volume- volume of blood pumped by one ventricle each Time it contracts stroke volume- volume of blood pumped by one ventricle each Time it contracts |
|
|
|
Volumes of air |
TIDAL - volume of air in a breath (0.4dm3) Breathing rate - how many breaths are usually taken in within a minute Ventilation rate - the volume of air breathed in or out usually in a minute V = T × B |
|
|
|
Spirometers can be used to Measure Tidal Volume and Breathing rate |
1) a spirometer has an oxygen filled chamber with a moveable loid 2) A person breathes through a tube connected to the oxygen chamber 3) As the person breathes in the lid of the chamber moves down When they breathe out it moves up 4) recorded on the rotating drum, creating a spirometer face 5) Soda lime in the tube absorbs the CO2 total volume decreases over time. |
|
|
|
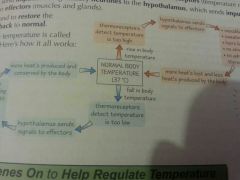
Homeostatic Systems - detect change and respond by negative feedback |
involves receptors, communication systems and effectors. 2) receptors detect when something is too high or too low. send this to the nervous system or the hormonal system to effectors 3) effectors counteract the change bringing the level back to normal mechanism that does this is called negative feedback 4) only works with in certain limits though- if the change is too big then the effectors may not be able to counteract it.
|
|
|
|
Mammals have many Feedback Mechanisms to change body temperature |
Sweating Hair lie flat- mammals have a layer trapped (air is a poor conductor of heat) when it's hot errector pilli muscles relax so the hairs lie flat. less air trapped . skin is less insulated and heat can be lost more easily. Vasodilation |
|
|
|
Increase body temperature |
shivering- muscles respiration Hormones- adrenaline and thyroxine, which increases metabolism so more heat is produced less sweat from sweat glands HAIR STANDS UP - erector pilli muscle makes hair stand up |
|
|
|
HYPOTHALAMUS CONTROLS BODY TEMPERATURE IN MAMMALS |
1) body temp comtrolled at a constant level, by hypthalamus 2) thermoreceptors let hypothalamus kmow if temp too high or low 3) Thermoreceptors send impulses along sensory neurons to the hypothalamus, which sends impulses along along motor neurons to effectors. 4) thermoregulation |
|
|
|
Hormones switch genes on to help regulate Temperature |
1) cells have protien called transcription factors that control the transcription of genes 2) Transcription factors bind to DNA sites near the start of genes and increase or decrease the rate of transcription. increase - activators decrease - repressors 3) Hormones can bind to some t-factors to change body temp Here's how: ♥ At normal body temp the thyroid hormone receptor (a transcription factor) binds to start of DNA ♥ This decrease the transcription of a gene coding for a protien that increases metabolic rate ♥ At cold temp thyroxine is released which binds to the thyroid hormone receptors = activator ♥ The transcription rate increases producing more protien that imcreases metabolic rate = increase in body temp |
|
|
|
Surgery Can help people woth injuries to play sports |
1) Keyhole surgery - way of doing surgery without a cut or an large incision made 2) Surgeons make a much smaller incision in the patient and insert tine vid cam and specialised mrdical instruments through body incision. 3) common sports injury is to damage cruciate ligaments found in the middle of your knee connecting thigh bone to lower leg 4) Damaged can be removed and replaced with a graft of ligament through small incison in the knee |
|
|
|
Advantage of key hole surgery ovee regular |
1) less blood loss and scaring 2) less pain after sugery and fast recovery as less damage made 3) easier for patient to return to routine and hospital stay shorter and hospital stay shorter |
|
|
|
Protheses |
mechanical replacement: - operate by picking up signals from the nervous systems - replaces cartilage and bone
|
|
|
|
Preformance enhancing drugs |
Anabolic Steroids - increases speed stamina increases rate of muscle growth increase aggression Stimulants- speeds up reaction, reduce fatigue and increase aggression Narcotic analgesics- reduce pain, so injuries don't affect their performance |
|