![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
28 Cards in this Set
- Front
- Back
|
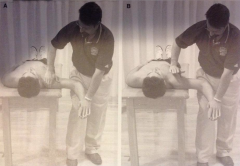
Cervical Compression Test (P. 547) |

Patient Position: Seated
Examiner Position: Standing behind the patient
Procedure: Please interlocked hands ontop of the head and press downward (axial loading of spine). Begin with lighter pressure and then gradually increase
Positive Test: Experiences pain or reproduction of symptoms in the upper cervical spine or upper extremities or both
Implication: Compression of the facet joints and narrowing of the intervertebral foramen resulting in pain |
|
|
Spurling Test (P. 548) |

Patient Position: Seated, neck laterally flexed
Examiner Position: Standing behind the patient
Procedure: Place interlocked hands on top of the head and press downward (axial loading relative to the trunk). Begin with lighter pressure and then gradually increase.
Positive Test: Pain or reproduction of symptoms radiating down patient's arm
Implications: Nerve root impingement by narrowing of the neural foramina |
|
|
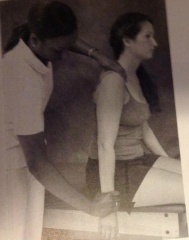
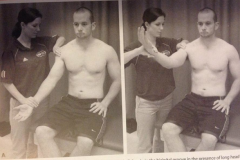
Brachical Plexus Traction Test (P. 557) |
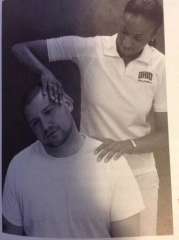
Patient Position: Seated
Examiner Position: Standing beside or behind the patient
Procedure: Place the stabilizing hand over the top of the effected shoulder. The other hand is placed on the temporal area of the head. Laterally flex the cervical spine away from the shoulder being stabilized/depressed
Positive Test: Reproduction of pain and/or peresthesia symptoms thorughout the involved upper extremity
Implications: Brachial plexus neurpraxia
Radiating pain of opposite side of lateral bending (tension of brachial plexus)
Radiating plain on side toward lateral bending (compression of cervical root of the two vertebrae) |
|
|
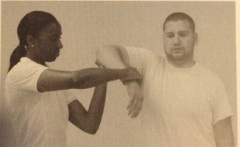
Adison's Test (P. 559) |

Patient Position: Seated, shoulder abducted to 30-60 degree, elbow extended with thumb pointing upward, and humerus externally rotated
Examiner Position: Standing behind the patient, one hand on the radial pulse
Procedure: Maintain the patient position while palpating the radial pulse and externally rotate and extend the patient's arm while he/she looks down the arm. Instruct the patient to inhale deeply and hold breath
Positive Test: Radial pulse disappears of markedly diminishes when compared to the opposite side
Implications: Subclavian artery occluded between the anterior and medial scalene muscle and pectoralis minor |
|
|
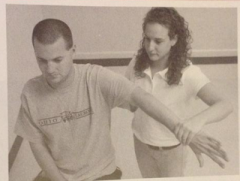
Allen Test (P. 560) |
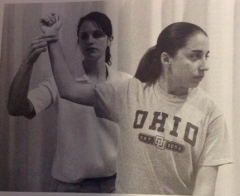
Patient Position: Seated. Head facing forward
Examiner Positon: Standing behind the patient, palpating the radial pulse on the side to be tested
Procedure: Flex elbow to 90 degrees wit shoulder abducted to 90 degrees. Passively extend (horizontal abduction) and externally rotate the shoulder and instruct the patient to turn head away from shoulder. Maintain radial pulse palpation throughout procedure. Patient rotates head toward opposite shoulder
Positive Test: Radial pulse disappears or reproduction of neurologic symptoms
Implications: Pectoralis minor muscle is compressing the neurovascular bundle |
|
|
Roo (EAST) Test (P. 562) |
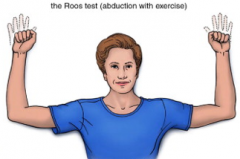
Patient Position; Seated or standing: shoulders abducted to 90 degrees and elbows flexed to 90 degrees with humerus externally rotated
Examiner Position: Standing in front of patient
Procedure: Patient is instructed to rapidly open and lcose his/her hands for 3 minutes
Positive Test: Inability to maintain the testing position and replication of sensory and/or motor symptoms in the extremity
Implications: Thoracic outlet syndrome of neurologic and/or origin |
|
|
Sparing Test (AKA Piano Key Test) |
Patient Position: Sitting or standing, arm relaxed by side
Examiner Position: Standing to side of patient
Procedure: Apply downward force over the end of the clavicle near the AC joint
Positive Test: Gross laxity (Some type of AC tear )
Video: https://www.youtube.com/watch?v=96gTvNQGMzU |
|
|
Apprehension Test (P 672) |
Patient Position: Supine preferred. Sitting or standing ok for on-the-field evaluation. Shoulder abducted to 90deg and elbow flexed to 90 deg.
Examiner Position: Standing to side of patient
Procedure: Support the arm at the elbow. The other hand applies pressure on distal forearm, slowly externally rotating the shoulder while it is abducted
Positive Test: The patient displays apprehension that the shoulder may dislocate and resists further movement. Pain is centered in the anterior capsule of the GH joint.
Implications: Anterior capsule, inferior GH ligement, or glenoid labrum have been compromised, allowing the humeral head to dislocate or subluxate anteriorly on glenoid fossa.
Apprehension coupled with pain is associated with instablity secondary and rotator cuff pathology
Pain in deep posterior shoulder may be associated with internal impingement |
|
|
Relocation Test (P. 674) |
Patient Positon: Supine preferred. Sitting or standing ok for on-the-field evaluation. Shoulder abducted to 90 degrees and elbow flexed to 90 degrees
Examiner Position: Standing to side of patient inferior to humerus of involved side
Procedure: Utilizing the same position and application of force as the apprehension test, place the stabilizing hand over the front of the shoulder and apply a posteriorly directed force
Positive Test: Decreased pain or increase ROM or both with apprehension test
Implication: Anterior pain may be result of increased laxity in the anteiror ligaments and capsular structures or a tear of the labrum. Posterior pain may be from internal of the posterior capsule or labrum
Supports increased laxity in anterior capsule owing to capsular damage or labrum tears. Manual pressure increases stability of anterior portion of GH capsule, allowing more external rotation to occur. |
|
|
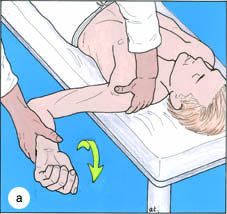
Sulcus Sign (P.678) |
Patient Position: Sitting, arm hanging down by side
Examiner Position: Standing lateral to involved side
Procedure: Place one hand over the top of the shoulder, stabilizing the scapula. Grasp the patient's arm distal to the elbow and apply traction (downward force) to the arm
Positive Test: Gapping between the acromion and head of humerus
When there is an indentation (sulcus) beneath the acromion process
Implication: Laxity in superior GH ligament
Grade 1 = 1 cm or less
Grade 2=1-2 cm Grace 3= greater than 2 cm |
|
|
Empty Can Test (P. 689) |
Patient Position: Sitting or standing, shoulder abduced to 90 degrees in the scapular plane (slightly forward of true abduction) with internal rotation (thumb down), elbow extended
Examiner Position: Standing, facing pateint
Procedure: Places one hand on the distal forearm, instruct the patient to resist your pressure as your push downward (resisted abduction)
Positive Test: Pain and weakness
Implications: Supraspinatus tendon = (1) Impinged between humeral head and/or acrominal arch (2) inflammed (3) Contains lesion |
|
|
Hawkins Impingement Test (P. 686) |
Patient Position: Sitting or standing
Examiner Position: Standing lateral or slightly forward of the involved shoulder
Procedure: Position the shoulder in 90 degrees flexion (in the Scapular plane) and elbow in 90 degrees flexion. Support underneath the elbow and grasp the distal forearm on the dorsal surface. Internally rotate the shoulder until pain or limit of range of motion is achieved
Positive Test: Pain with motion especially near the end of ROM
Implications: Rotator cuff (especially supraspinatus) or long head of biceps brachii impinges on the structures between the greater tuberoisty and inferior surface of the acromion process |
|
|
Yergason's Test (p. 690) |
Patient Position: Sitting or standing, elbow flexed to 90 degrees, and forearm midway between pronation and supination (thumb toward ceiling), humerus alongside trunk
Examiner Position: Lateral to patient. First palpate the bicipital groove to orient the patient to the location of the pain related to the evaluation. Then support behind elbow over olecranon process with one hand. Place one hand over top of distal forearm
Procedure: Instruct the patient to resist the downward force created by your hand over the distal forearm by simultaneously flexing and pronating the elbow and internally rotating the shoulder. (Examiner extends and supinates the elbow and externally rotates shoulder)
Positive Test: Pain, snapping of bicipetal groove
Pain at the superior glenohumeral joint
Implications:
(Primary) = Snapping or popping in the bicipital groove indicates a tear or laxity in the transverse humeral ligament. This pathology prevents the ligament from securing the long head of the tendon in its groove
(Secondary) = Pain with no associated popping in the bicepital groove may indicate biceps tendionopathy |
|
|
Speeds Test (P. 692) |
Patient Position: Sitting or standing, elbow extended, palm towards the ceiling, with shoulder slightly flexed
Examiner Position: Lateral to patient. Palpate the bicipetal groove with one hand. Then place other hand over top of distal forearm.
Procedure: Instruct the patient to move arm upward against your resistance, moving through the full range of motion.
Positive Test: Pain along the long head of the biceps brachii tendon, especially in the bicipital groove or at the superior shoulder
Implications: Inflammation of long head of biceps tendon as it passes through the bicipital groove. Possible tear of the transverse humeral ligament with concurrent instability of the long head of the biceps tendon as it passes through the bicipital groove. Pain at the superior shoulder (SLAP lesion) |
|
|
Valgus Stress test of the Elbow |
Patient Position: Standing or seated with elbow in complete extension, full supination
Examinaiton Position: Standing in front and slightly to the side of the patient with stabilizing hand on lateral aspect of elbow
Procedure: Place moving hand on distal forearm medially. Gently apply medially directed force with the stabilizing hand and laterally directed force with the distal hand
Positive Test: Observe for gapping on medial aspect of elbow. Note feeling of laxity. Note presence of and location of pain reported by patient.
Implications: Laxity on medial elbow compartment: joint capsule, medial (ulnar) ligament |
|
|
Varus Stress Test of the Elbow |
Patient Position: Standing or seated with elbow in complete extension, full supination
Examiner Position: Standing in front and slightly to the side of the patient with stabilizing hand on medial aspect of elbow
Procedure: Place moving hand on distal forearm laterally. Gentaly apply laterally directed force with the stabilizing hand and medially directed force with the distal hand.
Positive Test: Observe for gapping on lateral apsect of elbow. Note feeling of laxity. Note presence of and location of pain reported by patient.
Implications: Laxity on lateral elbow compartment: joint capsule, radial collateral ligament |
|
|
Tinel's Test (Sign) |

Patient Positions: Standing or seated with elbow in slight flexion
Examiner Position: Standing in front of the patient with stabilizing hand on distal forearm (supporting flexed position)
Procedure: Place index finger over middle finger, then gently tap distal aspect of arm, just superior to the ulnar tunnel, over the ulnar nerve
Positive Test: Numbness/tingling sensation along distribution of the ulnar nerve (medial forearm down 4th-5th fingers)
Implications: Ulnar nerve inflammation/sensativity |
|
|
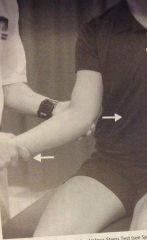
Tennis Elbow Test |
Patient Position: Standing or seated with elbow in 90 degree flexion, forearm pronated
Examiner Position: Standing to side of the patient with stabilizing hand palpating the wrist extensor common tendon
Procedure: Instruct patient to make a fist, then instruct them to resist wrist extension (not allowing elbow flexion angle to change)
Positive Test: Sudden or severe pain over the wrist extensors near the lateral epicondyle.
Implications: lateral condyle epicondylagia |
|
|
Golfer's Elbow Test |

Patient Position: Standing or seated with elbow in 90 degree flexion, forearm supinated
Examiner Position: Standing to side of the patient with stabilizing hand palpating the wrist flexor common tendon
Procedure: Instruct patient to make a fist, then instruct them to resist wrist flexion (not allowing elbow flexion angle to change)
Positive Test: Sudden or severe pain over the wrist flexors near the medial epicondyle
Implications: Medial condyle epicondylagia |
|
|
Pinch Grip Test: |
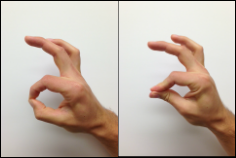
Patient Position: Seated or standing
Examiner Position: Observing patient
Procedure: Instruct patient to pinch tips of index finger and thumb together (Ok sign)
Positive Test: Normal test: tip or tip pinch, Abnormal: pulp to pulp pinch
Implications: Pathology of anterior interosseus nerve (possibly entrapment in pronator teres muscle) |
|
|
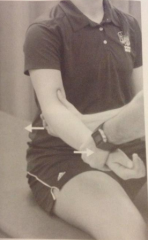
Isolation: Flexor Digitorum Profundus (Jersey Finger) |

Patient Position: Seated or standing, elbow flexed 90 degrees, forearm supinated
Examiner Position: Standing beside the patient on involved side, facing same direction as patient
Procedure: Stabilize the fingers alongside the involved finger with both hands, while stabilizing middle phalange of involved finger. Instruct patient to flex finger tip.
Positive Test: Inability to flex at DIP joint.
Implications: Indicates FDP tendon avulsion or rupture |
|
|
Isolation: Flexor Digitorum Superificalis |
Patient Position: Seated or standing, elbow flexed 90 degree, forearm supinated
Examiner Position: Standing in front of patient
Procedure: Stabilize the fingers alongside the involved finger with both hands, while stabilizing proximal phalange of involved finger. Instruct patient to flex finger.
Positive Test: Instability to flex at PIP joint
Implications: Indicates FDS tendon rupture |
|
|
Finkelstein's Test |
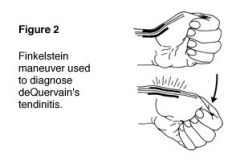
Patient Position: Seated or standing, elbow flexed to 90 or shoulder flexed to 40-60 degree
Examiner Position: Standing in front of patient
Procedure: Instruct patient to close fist around the thumb and then ulnarly deviate wrist. Clinician can stabilize forear and apply gentle overpressure if necessary
Positive Test: Pain over extensor and abductor tendons of thumb
Implications: Tendinopathy of extensor pollicus brevis and longus and abductor pollicus longus tendons: deQuervain's syndrome/disease |
|
|
Allen's Test for Ulnar and Radial Artery Integrity |
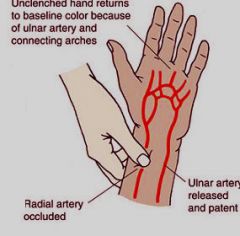
Patient Position: Seated or standing, elbow flexed to 90 degrees, forearm supinated
Examiner Position: Standing in front of patient
Procedure: Instruct patient to open and close hand several times and ifnish with a closed fist. Clinician simultaneously provides pressure over the ulnar and radial arteries at the wrist crease. Instruct patient to open hand while clinician maintains pressure. Release pressure on one artery. Observe for return of circulation (flush) to hand. Repeat entire procedure for other artery
Positive Test: Palm circulation does not return immediately (very slow!)
Implications: Reduced patency (reduced openness) of artery |
|
|
Phalen's Test |

Patient's Position: SEated or standing, elbows flexed to 90 degree, forearms pronated, dorsal surface of hands facing each other
Examiner Position: N/a
Procedure: Instruct patient to press dorsal surface of hands together, maximizing wrist flexion. Hold position for 1 minute
Positive Test: Patient reports pain or numbness along distribution of median nerve (usually into thumb and palmar surface of first three fingers)
Implications: Carpal tunnel syndrome |
|
|
Valgus Stress Test of the Thumb |
Patient Position: Seated or standing, elbow flexed to 90 degrees, forearm neutral (between pronation and supination)
Examiner Position: Stand to side of patient on involved side, stabilizing the metacarpal and proximal phalange of the MCP joint of the thumb with each ahdn by placing thumbs along the ventral surface of the thumb
Procedure: Apply valgus force at the MCP joint of the thumb, attempting to open up the medial joint line, to stress the UCL ligament
Positive Test: Increase gapping or laxity over the ulnar joint line of MCP joint of thumb
Implications: Injury to ulnar collateral ligament of thumb |
|
|
Valgus/Varus Stress Test - Interphalangeal joints |
Patient Position: Seated or standing, elbow flexed to 90 degree, forearm pronated
Examiner Position: Stand to side of patient on involved side, stabilizing the phalanges proximal and distal to the joint of interest
Procedure: Apply valgus force at the desired IP joint. Repeat by applying varus force at desired IP joint
Positive Test: Increased gapping or laxity over the medial or lateral joint line of IP joint of the finger.
Implications: Rupture or avulsion fracture involving the collateral ligaments
Video: http://youtu.be/qHJ-C1MdI3Y |
|
|
Axial Loading of Fingers |
Patient Position: Seated or standing, elbow flexed to 90 degree, forearm pronated
Examiner Position: Standing in front of patient, stabilizing over wrist and dorsum of the hand
Procedure: Grasp the finger at the levle of the most distal non-involved phalange. Apply a compression force along the long axis of the finger (axial loading)
Positive Test: Pain at level of IP joint or along phalange
Implications: Phalangeal fracture |