![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
152 Cards in this Set
- Front
- Back
|
The dating scan is best perform at what week? What is measured? |
Between 11+3 and 13+6 weeks gestation by measuring CRL. From 14 and 20 weeks the dating use the head circumference. |
|
|
Women at high risk of developing pre eclampsia |
1. Hypertensive disease during previous pregnancy 2. CKD 3. Autoimmune disease i.e. SLE or antiphospholipid syndrome 4. DM type 1 or 2 5. Chronic hypertension |
|
|
Women at high risk of preterm birth |
1. Previous preterm birth
2. Late miscarriage
3. Multifetal pregnancy
4. Cervical weakness i.e. previous cervical surgery 5. Infection i.e. chorioamnionitis 6. Polyhydramnios 7. APH i.e. placental abruption 8. Stress |
|
|
Risk factors for development of GDM |
1. Previous GDM 2. Previous macrosomia (>4.5kg) 3. High BMI (>30kg/m2) 4. First degree relative with diabetes |
|
|
Acute complications of RDS in baby |
1. Hypoxia 2. Asphyxia 3. Intraventricula hemorrhage 4. Necrotizing enterocollitis |
|
|
Foregut endoderm gives rise to: |
Oesophagus Stomach Proximal half of duodenum Liver Pancreas |
|
|
Midgut endoderm gives rise to: |
Distal half of duodenum Jejunum Ileum Caecum Appendix Ascending colon Transverse colon |
|
|
Hindgut endoderm gives rise to |
Descending colon Sigmoid colon Rectum |
|
|
What is the association of high maternal BMI and fetal outcome? |
1. BMI >40 kg/m2 has threefold risk of neural tube defect compared to BMI <30kg/m2. 2. Fetal macrosomia and its complication 3. Fetal growth restriction (FGR) and its complication 4. Miscarriage, 1 in 4 pregnancy if BMI >30 5. Still birth, doubling stillbirth risk (0.5 to 1%) |
|
|
Prior to birth, ductus arteriosus remains patent due to action of? |
Prostaglandin E2 and prostacyclin, which act as local vasodilators |
|
|
By what weeks the type I and II epithelial cell of the lungs begin to differentiate? |
By 26 weeks |
|
|
What produces pulmonary surfactant and when? |
Type II cells starting from about 30 weeks |
|
|
Normally how is the closure of foramen ovale occurs? |
+ During gestation the lung is filled with fluid. But they are absorbed at birth + With clearance of the fluid and the onset of breathing, the resistance of pulmonary vascular bed falls. + Increase in pulmonary blood flow + Raised pressure in LEFT atrium + The high pressure facilitate the closure of foramen ovale |
|
|
What is the content of pulmonary surfactant? What is it for? |
+ Surfactant mostly contains phospholipids (phosphatidylcholine) + Surfactant lowers surface tension, which prevent small alveoli collapse during expiration. |
|
|
What is omphalocele? |
+ Failure of the midgut to re-enter the abdominal cavity following physiological hernia normally by the 12 week |
|
|
What is the most common alimentary tract fistula in fetus? |
+ Tracheo-oesophageal fistula (TOF) + Commonly associated with other congenital anomalies VACTERL |
|
|
What is the role of choriodecidual complex in the initiation of labor |
Production of prostaglandin E2 and F2a |
|
|
Throughout pregnancy, who are producing the amniotic fluid? |
+ Initially amnion + By 10th week, mainly a transudate from fetal serum via skin and umbilical cord. + From 16 week, from fetal kidneys and lungs fluid |
|
|
Roughly, what is the volume of amniotic fluid throughout pregnancy? |
10 weeks = 30ml 20 weeks = 300ml 30 weeks = 600ml 38 weeks = 1000ml But from term, rapid fall 40 weeks = 800ml 42 weeks = 350ml |
|
|
Function of amniotic fluid |
1. PROTECT the fetus from mechanical injury 2. Permit FETAL MOVEMENT while preventing limb contracture 3. Prevent ADHESION between fetus and amnion 4. Permit fetal LUNG DEVELOPMENT in which there are two-way movement of fluid into fetal bronchioles. (absence of amniotic fluid in second trimester associated with pulmonary hypoplasia) |
|
|
At what week can we first see fetal heartbeat in ultrasound |
By about 6 weeks |
|
|
Early pregnancy trans-vaginal ultrasound is useful to diagnose what disorders? What is the expected u/s findings? |
1. Incomplete or missed miscarriage = fetus is present but no fetal heartbeat. 2. Blighted ovum = empty gestation sac 3. Ectopic pregnancy = Positive pregnancy test but no gestation sac within the uterus, and may have adnexal mass w/wo a fetal pole or presence of fluid in the pouch of Douglas |
|
|
How to differentiate monochorionic and dichorionic twin from ultrasound scan? |
1. Dichorionic twin has thicker inter-twin membrane (monochorionic = seperating membrane consist of 2 amnion) (dichorionic = seperating membrance consisit of 2 amnion and 2 chorion) 2. 'twin peak' or 'lambda' sign in dichorionic twin best seen at 9 - 10 weeks |
|
|
What is the ultrasound measurement used to assess amniotic fluid volume
|
1. Maximum vertical pool = < 2cm oligo, > 8cm poly 2. Amniotic fluid index (AFI) = Uterus is divided into 4 'ultrasound' quadrant. AFI is the summation of vertical measurement of deepest pool of fluid in each quadrants. |
|
|
what is the value of AFI in oligo- and polyhydramnios? |
AFI alters throughout gestation. In third trimester: < 5cm is oligohydramnios <10cm is reduced volume >25cm is polyhydramnios, |
|
|
Normal fetal heart rate at term |
110 - 150 bpm (160 bpm is the upper limit prior to term) |
|
|
Causes of fetal tachycardia |
1. Maternal or fetal infection 2. Acute fetal hypoxia 3. Fetal anemia 4. Drugs i.e. adrenoreceptor agonist (ritodrine = offmarket tocolytic) |
|
|
When is the baseline variability in CTG is considered abnormal |
When it is less than 10 bpm |
|
|
What are the possible causes for reduced baseline variability in CTG |
1. fetal sleep states and activity 2. fetal hypoxia 3. fetal infection 4. Drugs suppressing fetal CNS i.e. opioids & hypnotics |
|
|
Define fetal heart rate accelerations and what is considered normal in CTG |
Increase in baseline fetal HR of atleast 15bpm for at least 15 seconds. The presence of 2 or more accelerations on 20-30min antepartum CTG is a positive sign of fetal health |
|
|
What is fetal heart rate deceleration and what does it signifies? |
= transient reduction of baseline fetal HR of 15bpm or more, lasting for atleast 15sec May be indicative of: Fetal hypoxia or umbilical cord compression |
|
|
What are the parameters for Biophysical Profile (BPP)? |
1. Fetal Breathing Movement (FBM) 2. Fetal gross body movement 3. Fetal tone 4. CTG 5. AFI |
|
|
What is the scoring for BPP? |
each of the 5 parameters, suboptimal = 0, normal = 2 + Scores of 0, 2, and 4 is considered abnormal + Scores of 8, or 10 is considered normal Score of 6 require repeat test to exclude fetal sleep as cause |
|
|
How to identify fetal acidemia by using doppler ultrasound |
1. Increasing pulsatility index in ductus venosus or IVC 2. Absent diastolic blood flow in the aorta |
|
|
How to identify fetal anemia by using doppler ultrasound |
Increase in peak systolic velocity in the middle cerebral artery |
|
|
How to identify high resistance to flow in uterine artery by using doppler ultrasound? |
Diastolic 'notch' in the waveform |
|
|
What are obstetric conditions associated with high resistance pattern in the uterine artery doppler studies?
|
1. Pre-eclampsia 2. FGR 3. Placental abruption |
|
|
What is cerebroplacental ratio |
Ratio of the pulsatility indices between fetal middle cerebral artery and the umbilical artery |
|
|
Aim of obstetric ultrasound in early pregnancy scan (11 - 14 weeks) |
1. Confirm fetal VIABILITY 2. estimation of GESTATIONAL AGE 3. Diagnose MULTIPLE PREGNANCY, and determine its CHORIONICITY 4. Identify markers of CHROMOSOME ABNORMALITY i.e. Down Syndrome 5. Identify fetus with GROSS STRUCTURAL ABNORMALITY |
|
|
Aim of obstetric ultrasound at 20 week scan (18 - 22 weeks)
|
1. Detailed fetal ANATOMICAL SURVEY for structural/chromosomal anomalies. 2. Locate PLACENTA and identify low-lying placenta for further close monitoring 3. Estimate AMNIOTIC FLUID VOLUME 4. DOPPLER STUDY of maternal uterine artery to screen for adverse pregnancy outcome i.e. SGA 5. Measure CERVICAL LENGTH |
|
|
Aim of obstetric ultrasound in the third trimester
|
1. Assess fetal GROWTH 2. Assess fetal WELLBEING |
|
|
How to identify high resistance in the umbilical artery in Doppler study? What can the high resistance lead to? |
Absent or reversed end-diastolic flow in umbilical artery. Strongly associated with fetal hypoxia and intrauterine death |
|
|
What is the CTG findings of fetal hypoxia |
1. Fetal tachycardia 2. Reduced variability 3. Absence of acceleration 4. Presence of deceleration |
|
|
Advantage and disadvantage of chorionic villus sampling (CVS) over amniocentesis |
ADVANTAGE + Can be PERFORM EARLIER in pregnancy (although should not be performed before 10 weeks) + Provide LARGER SAMPLE for screening some genetic disorder requiring PCR DISADVANTAGE - Additional RISK OF MISCARRIAGE is higher compared to amniocentesis if performed after 15 weeks |
|
|
Indication to perform cordocentesis |
1. When FETAL BLOOD is needed for test i.e. severe fetal anemia / thrombocytopenia 2. When rapid full culture for KARYOTYPE is needed |
|
|
First trimester screening tool for Down's Syndrome |
1. Blood test for measuring HCG and PAPP-A (raised HCG + low PAPP-A) 2. Ultrasound scan for NT and CRL (Thick NT in relation to CRL) |
|
|
Second trimester screening for Down's Syndrome (14 - 20 weeks) |
Quadruple test: Raised HCG Low AFP Low unconjugated oestriol Raised inhibin A |
|
|
What are other markers beside NT, PAPP-A and Quadruple test can be used to further improve accuracy of screening for Down's Syndrome. |
1. Measuring NASAL BONE 2. Measuring FRONTOMAXILLARY NASAL ANGLE 3. Presence of TRICUSPID REGURGITATION at the ductus venosus waveform |
|
|
Hyperemesis gravidarum increases the obstetric risk of? |
1. Preterm birth 2. Low birth weight baby |
|
|
Non obstetric complication of hyperemesis gravidarum |
1. Malnutrition 2. Vitamin deficiency (Wernicke's encephalopathy in B1 deficiency) 3. Oesophageal trauma / Mallory-Weiss tear |
|
|
Treatment for hyperemesis gravidarum |
1. Fluid replacement therapy 2. Vitamin supplement (thiamine) 3. Antiemetics i.e. phenothiazines |
|
|
Pregnancy is a hypercoagulable state. What is the alterations in the thrombotic and fibrinolytic system? |
Increase in clotting factors VIII, IX, X and fibrinogen level Reduction in protein S and antithrombin (AT) III |
|
|
Why is the risk of VTE is higher in pregnant women? |
1. Hypercoagulable state 2. Venous stasis due to pressure on the IVC by gravid uterus 3. Immobility |
|
|
What are the risk factors for thromboembolism in pregnancy? |
Pre-existing: 1. > 35 y/o maternal age 2. Thrombophilia 3. Severe varicose vein 4. Smoking 5. Obesity 6. Previous VTE Specific to pregnancy: 7. Multiple pregnancy 8. Grand multiparity (more than 5 pregnancies) 9. Pre-eclampsia |
|
|
Treatment for VTE in pregnancy |
parenteral LMWH as it does not cross placenta unlike warfarin which might cause limb/facial defect and intracerebral hemorrhage |
|
|
Possible cause for oligohydramnios |
Too little production (1 - 5): 1. Renal agenesis = u/s no renal tissue, no bladder 2. Multicystic kidney = u/s large kidney with multiple cysts, no visible bladder 3. Urinary tract anomalies/obstruction = u/s kidney may present but urinary tract dilatation. 4. FGR / placental insufficiency = reduced SFH & FM, abnormal CTG, u/s SGA / abnormal Doppler 5. Maternal drug i.e. NSAIDs 6. Post-date pregnancy 7. Leakage i.e. PPROM |
|
|
Possible causes for polyhydramnios |
Maternal cause: 1. Diabetes Placental cause: 2. Chorioangioma 3. AV fistula Fetal cause: 4. Multiple gestation 5. Idiopathic 6. Oesophageal atresia / TOF 7. Duodenal atresia 8. Neuromuscular fetal disorder (prevent swallowing) 9. Anencephaly |
|
|
What are the types of breech presentation |
1. Extended / Frank breech 2. Flexed / complete breech 3. Footling |
|
|
Obstetric risk of breech presentation |
1. Cord prolapse 2. Foot prolapse |
|
|
Predisposing factors for breech presentation |
Maternal 1. Fibroids 2. Congenital uterine abnormalities i.e. bicornuate uterus 3. Previous surgery Fetal / placental 4. Multiple gestation 5. Prematurity 6. Placenta previa 7. Structural abnormality i.e. anencephaly or hydrocephalus 8. Oligohydramnios 9. Polyhydramnios |
|
|
Management option of breech presentation |
1. External Cephalic Version (ECV) 2. Vaginal breech delivery 3. Electice Caesarean section |
|
|
When can we do ECV for breech pregnancy? |
At or after 37 completed weeks of gestation |
|
|
Outline how the ECV is performed |
1. At 37 weeks the earliest 2. Should be performed with tocolytics i.e. nifedepine 3. Ensure patient emptied her bladder 4. Patient lie supine with left lateral tilt 5. With u/s guidance, elevate the breech from pelvis 6. Attempt to manipulate the fetus in direction of forward roll 7. Bring the head down to the pelvis |
|
|
Contraindication of ECV |
1. Fetal structural abnormality i.e. hydrocephalus 2. Placenta previa 3. Oligohydramnios 4. Polyhydramnios 5. Hx of APH 6. Previous surgical scar of the uterus i.e. carsarean / myomectomy 7. Multiple gestation 8. Hypertensive disorder / pre eclampsia 9. Plan to deliver by caesarean anyway |
|
|
The risks of ECV |
1. Placental abruption 2. PROM 3. Cord accident 4. Transplacental hemorrhage 5. Fetal bradycardia |
|
|
Feto-maternal pre-requisites for vaginal breech delivery |
1. Either frank or flexed breech. Fetal feet should not be below fetal buttocks 2. No evidence of feto-pelvic disproportion 3. EFW < 3.5 kg 4. No evidence of fetal head hyperextension |
|
|
How the baby head is delivered in vaginal breech delivery |
Mauriceau-Smellie-Veit manoeuvre If unsuccesful, can use forceps |
|
|
What is post term pregnancy |
A pregnancy that has extended to or beyond 42 weeks |
|
|
Risks of post term pregnancy |
1. Stillbirth 2. Perinatal death 3. Prolonged labour 4. Caesarean section |
|
|
Immediatel induction or labour post-dates should take place if: |
1. Reduced amniotic fluid on scan 2. FGR 3. Reduced fetal movement 4. CTG not perfect 5. Mother has significant medical condition i.e. hypertension |
|
|
Define antepartum hemorrhage |
Vaginal bleeding from 24 weeks gestation |
|
|
Causes of antepartum hemorrhage |
Placental causes 1. Placental abruption 2. Placenta praevia 3. Vasa praevia Local causes 4. Cervicitis 5. Cervical ectropion 6. Cervical carcinoma 7. Vaginal trauma 8. Vaginal infection |
|
|
How to prevent rhesus isoimmunization |
Intramuscular administration of anti-D immunoglobulins |
|
|
Signs of fetal anemia |
1. Polyhydramnios 2. Enlarged fetal heart 3. Ascites & pericardial effusions 4. Hyperdynamic fetal circulation (raised peak velocity in MCA?) 5. Reduced fetal movement 6. Abnormal CTG with reduced variability, eventually a 'sinusoidal' |
|
|
What is the complications of multiple pregnancies |
Fetal complications: 1. Preterm birth 2. FGR 3. Cerebral palsy 4. Stillbirth Maternal complications: 5. Hypertensive disorder 6. Thromboembolic disorder 7. APH 8. PPH |
|
|
In diamniotic twin pregnancy, what separates the two cavities? |
Separated by a thick three-layer membrane consist of a fused amnion in the middle with chorions on either side |
|
|
In monozygotic twin pregnancy, what determines the chorionicity and the amniocity? |
+ If the zygote split shortly after fertilization = DCDA + If the zygote splits between day 4 and day 8 post-fertilization = MCDA + If the zygote splits between day 8 and day 12 post-fertilization = MCMA
|
|
|
What is the prognosis of intrauterine death of one fetus in a dichorionic twin pregnancy |
+ If the death occur in the second or third trimester, it may be associated with the onset of labor for the survived fetus + Although some pregnancy may continue uneventfully and even deliver at term. |
|
|
What is the prognosis of intrauterine death of one fetus in a monochorionic twin pregnancy |
+ May result in immediate complications for the survivor i.e. death or brain damage, with subsequent neurodevelopment handicap. |
|
|
How is fetal death of one of the fetus in monochorionic pregnancy affect the surviving fetus. |
+ There are placental vascular anastomoses between the two fetus + With the death, it will cause acute hypotensive episode + In turn will cause hemodynamic volume shift from the live to the dead fetus Acute relase of vasoactive substance to the living circulation may also play a role |
|
|
How is twin-to-twin transfusion syndrome (TTTS) occurs? |
+ Abnormal development of unbalance vascular anastomoses between the two fetus + More AV connections occurring in one direction than the other + Alteration in the hydrostatic and osmotic forces |
|
|
There are 4 type of vascular connections (anastomoses) between monochorionic fetuses; AV, VA, AA, and VV Which one is protective against TTTS? |
AA |
|
|
How to diagnose TTTS? |
Based on ultrasound criteria: 1. Single placental mass 2. Concordant (similar?) gender 3. Oligohyrdramnios in one sac and polyhydramnios in another sac, based on Max. Veritcal Pool (MVP) 4. Discordant bladder appearance 5. Hemodynamic and cardiac compromise |
|
|
What is TAPS in multiple pregnancy |
Twin Anemia-Polycythemia Sequence (TAPS) + Larger inter-twin hemoglobin difference + Anemia in one twin and Polycythemia in the other + But no oligo- polyhydramnios sequence seen (unlike TTTS) |
|
|
What are the fetal complication of TAPS |
1. Fetal & placental thrombosis in the polycythemic fetus 2. Hydrops fetalis in the anemic fetus |
|
|
Management of TTTS |
Serial fortnightly ultrasound in monochorionic pregnancy for early detection of TTTS from 16 to 24 weeks When TTTS is diagnosed, management option include: 1 Expectant management 2 Amnioreduction 3 Septostomy 4 Fetoscopic laser ablation of vascular anastomoses |
|
|
What are the possible complications for monochorionic monoamniotic MCMA twin pregnancy |
1. Perinatal mortality 2. Cord entanglement 3. Neurological morbidity 4. Congenital anomalies i.e. neural tube defect / abd. wall & urinary tube defect 5. |
|
|
High risk pregnancy for post partum VTE that requires post-natal LMWH? How long is the LMWH therapy for this group? |
LMWH therapy for at least 6 weeks High risk group: 1. Any previous VTE 2. Anyone requiring antenatal LMWH 3. High risk thrombophillia 4. Low risk thrombophillia with positive family history |
|
|
Intermediate risk pregnancy for post partum VTE that requires post-natal LMWH?How long is the LMWH therapy for this group |
At least 10 days postnatal prophylactic LMWH
Intermediate risk:
1. Emergency Caesarean section in labor
2. BMI 40 or over
3. Readmission or prolonged (atleast 3 days) admission during puerperium
4. Any surgical procedure during puerperium except immediate repair of perineum
5. Medical comorbidities i.e. cancer, HF, active SLE, IBD, etc |
|
|
In uncomplicated MCMA pregnancy, what is the timing and mode of delivery? |
Caesarean section at 32 - 34 weeks after course of corticosteroids
(Due to risk of cord entanglement and death) |
|
|
In uncomplicated DCDA pregnancy, what is the timing and mode of delivery? |
Vaginal delivery is possible if the presenting twin is cephalic Normally delivery from 37 weeks onwards |
|
|
What test can be performed to identify patient in preterm labor? |
Fetal fibronectin (fFN) levels in cervicovaginal fluid. If present between 22 to 36 weeks, predict a preterm delivery (PTD) |
|
|
What is tocolytics? Example of tocolytics? |
Tocolytics are used to suppress preterm birth and delay delivery 1. Calcium ch blocker i.e. nifedipine 2. Oxytocin receptor antagonist i.e. atosiban |
|
|
How PPROM is diagnosed |
+ Clinical history + Speculum examination = pool of liquor in the vagina |
|
|
Indications for cervical cerclage |
1. Multiple midtrimester loses / preterm deliveries 2. Cervix shortens (<25mm) with hx of cervical surgery / prev. preterm birth 3. Cervix is dilating in the absence of contraction |
|
|
Preventions of preterm delivery |
1. Vaginal progesterone 2. Cervical cerclage |
|
|
Define pre-eclampsia. |
+ hypertension of atleast 140/90 mmHG. + recorded at 2 separare occasions at least 4 hours apart + presence of at least 300mg protein in 24hour urine collection + onset after the 20th week + in previously normotensive woman + resolve completely by the sixth postpartum week |
|
|
Risk factors for pre eclampsia |
1. First pregnancy 2. Prev. hx of pre eclampsia 3. >10 years since last pregnancy 4. Maternal age >40 5. BMI >35 6. Family hx of pre eclampsia 7. Booking diastolic BP of >80 mmHg 8. Booking proteinuria (of >1+ on more than 1 occasion or quantified at >0.3 g/24h) 9. Multiple pregnancy 10. Certain u/l medical condition i.e. htn / renal / dm |
|
|
What is HELLP syndrome and its clinical feature |
Hemolysis, elevated liver enzymes and low platelets. + epigastric pain + nausea + vomiting + absent or mild hypertension or mild hypertension or mild hypertension |
|
|
Complication of HELLP syndrome |
1. AKI 2. Placenta abruptio 3. Stillbirth |
|
|
Clinical presentation of pre eclampsia |
Majority is asymptomatic or vague flu like symptoms.
1. Frontal headache
2. Visual disturbance
3. Epigastric pain / tenderness
4. Vomiting
5. Swelling of the face, hand, and feet 6. Hypertension 7. Hyperreflexia 8. Clonus |
|
|
Blood pressure target in management pre eclampsia |
150 / 80-100 mmHg |
|
|
Degree of hypertension in pre eclampsia |
Mild: 140-149 / 90-99 mmHg Moderate: 150-159 / 100-109 Severe: >160 / >110 |
|
|
Antihypertensive agents in pre eclampsia |
1. Labetalol 2. Nifedipine 3. Methyldopa 4. IV hydralazine / Labetalol |
|
|
What is given as prevention for eclampsia? |
IV Magnesium sulphate Prohylactically given 24h prior to planned time of delivery in pre eclampsia pt. |
|
|
In pre eclamptic patient, ideally delivery at term. But what is the threshold for considering planned early birth? |
1. Inability to control BP with medications 2. Maternal SPO2 <90% 3. Progressive deterioration of liver function, renal function, hemolysis or platlet count 4. Ongoing neuro features i.e. severe headache, visual disturbance, eclampsia 5. Placenta abruptio 6. Reversed end diastolic flow in umbilical artery 7. Non reassuring CTG 8. Stillbirth |
|
|
Define FGR |
Failure of the fetus to achieve its genetic growth potential |
|
|
Causes for SGA fetus |
1. Constitutionally small
2. Placental insufficiency 3. FGR FGR FGR
4. Fetal infection
5. Chromosomal abnormalities 6. Congenital anomalies |
|
|
Causes of fetal growth restriction (FGR) |
Reduced fetal growth potential 1. Aneuploidies i.e. trisomy 18 2. Single gene defects i.e. Seckel's syndrome 3. Structural abnormalities i.e. renal agenesis 4. Intrauterine infection i.e. CMV Maternal factors 5. Undernutrition 6. Maternal hypoxia 7. Drugs Placental factors 8. Reduced uteroplacental perfusion i.e. pre eclampsia / sickle cell 9. Reduced fetoplacental perfusion i.e. single umbilical artery / TTTS |
|
|
Commonest cause of symmetrical and asymmetrical FGR |
Symmetrical FGR 1. Chromosomal disorder 2. Fetal infectiona 3. Chronic hypertension 4. CKD Asymmetrical FGR 1. Uteroplacental insufficiency - fetal hypoxia |
|
|
Pregnancies at risk of FGR |
1. Multiple pregnancy 2. Hx of FGR in prev. pregnancy 3. Current heavy smoker 4. Current drug user 5. U/l medical disorders i.e. htn/dm 6. SFH less than expected |
|
|
Risk factors requiring intrapartum prophylaxis for GBS (penicilin or clindamycin) |
1. Intrapartum fever > 38c 2. Prolonged (>18h) rupture of membrane 3. Prematurity < 37 weeks 4. Previous infant with GBS 5. Incidental detection of GBS in current pregnancy 6. GBS bacteruria |
|
|
What is the AP and transverse diameter of the pelvic inlet? |
AP = 11cm Transverse = 13.5cm |
|
|
What is the AP and transverse diameter of the midpelvis |
AP = 12cm Transverse = 12cm |
|
|
What is the AP and transverse diameter of the pelvic outlet |
AP = 13.5cm Transverse = 11cm |
|
|
What is the most favorable fetal head position for labor? |
Occipito-anterior (OA) position |
|
|
length of suboccipito-bregmatic diameter |
9.5 cm |
|
|
Length of suboccipito-frontal diameter |
10cm |
|
|
Length of occipito-frontal diameter |
11.5cm |
|
|
Length of occipito-mental diameter |
13cm |
|
|
length of submento-bregmatic diameter |
9.5cm |
|
|
What is effacement |
+ Lower segment of the uterus become thinner and more stretched + Eventually, the cervix is being 'taken up' (effacement) into the lower segment of the uterus forming a continuum |
|
|
Define onset of labor |
Presence of strong, regular, painful contractions resulting in progressive cervical changes In practice, the diagnosis is suspected when awoman presents with contraction-like pains, and is confirmed when the midwifeperforms a vaginal examination that reveals effacement and dilatation of thecervix |
|
|
Define 'latent phase' of first stage of labor |
time between the onset of regular painful contractions and 3–4 cmcervical dilatation
|
|
|
Define 'active phase' of first stage of labor
|
time between the end of the latent phase (3–4 cm dilatation) and fullcervical dilatation (10 cm). |
|
|
Define 'passive phase' of second stage of labor |
time between full dilatation and the onset ofinvoluntary expulsive contractions.
|
|
|
Define 'active phase' of second stage of labor |
time between the onset of maternal urge to push until the baby is delivered. |
|
|
Define third stage of labor |
time from delivery of the fetus or fetuses until complete delivery of theplacenta(e) and membranes.
|
|
|
Outline the mechanism of labor |
1. Engagement 2. Descent 3. Flexion 4. Internal Rotation 5. Extension 6. Restitution 7. External Rotation 8. Delivery of shoulder and body |
|
|
What happen to fetus in fetal hypoxia |
+ A switch from aerobic to anaeobic metabolism + Generation of lactic acid and hydrogen ions + May overwhelm buffer system and cause metabolic acidosis |
|
|
Indication for continuous EFM during labor |
1. Significant meconium staining of amniotic fluid 2. Abnormal FHR 3. Maternal pyrexia 4. Fresh vaginal bleeding 5. Augmentation of contraction with oxytocin infusion 6. Maternal request |
|
|
Sign of placental separation |
1. Apparent lengthening of the cord 2. Small gush of blood from the placental bed 3. Rising of the uterine fundus to above the umbilicus 4. Uterine contraction resulting in firm globular feel on palpation |
|
|
Active management of third stage of labor (reducing the incidence of PPH) |
1. IM oxytocin 10 IU (as the anterior shoulder is delivered or immediately after delivery of the baby) 2. Early clamping and cutting of the umbilical cord 3. Controlled cord traction |
|
|
Findings suggestive of cephalo-pelvic disproportion (CPD) |
1. Fetal head is not engaged 2. Progress is slow or arrest despite efficient uterine contractions 3. Vaginal examination shows sever moulding or caput formation 4. Head is poorly applied to the cervix 5. Haematuria |
|
|
Causes of poor progress in the first stage of labor |
1. Dysfunctional uterine activity 2. Cephalopelvic disproportion (CPD) 3. Malpresentation 4. Abnormalities of the birth canal i.e. fibroids, cervical dystocia (cervix that effaces but fails to dilate) |
|
|
Causes of poor progress in second stage of labor |
1. Secondary dysfunctional uterine activity (weak, inefficient contraction may be secondary to maternal dehydration or ketosis) 2. Narrow midpelvis (android pelvis) 3. Resistant perineum (esp. nulliparous) 4. Persistent OP position |
|
|
Indications for epidural analgesia |
1. Prolonged labour / oxytocin augmentation 2. Maternal hypertensive disorder 3. Multiple pregnancy 4. Selected maternal medical conditions 5. High risk of operative intervention |
|
|
Contraindications for epidural analgesia |
1. Coagulation disorders (low platelet) 2. Local or systemic sepsis 3. Hypovolemia 4. Inadequate proper personel or equipment |
|
|
Relative contraindications to VBAC |
1. Two or more previous caesarean section scars 2. Requiring IOL 3. Previous childbirth suggestive of CPD' 4. Previous 'classical' caesarean section scar (upper segment) in an ABSOLUTE CONTRAINDICATION |
|
|
Common reasons for IOL |
1. Prolonged pregnancy (post-date) 2. PROM 3. Maternal hypertensive disorder i.e. pre eclampsia 4. Maternal diabetes 5. Twin gestation 6. Intrahepatic cholestasis of pregnancy 7. Fetal macrosomia in the absence of maternal diabetes |
|
|
When should IOL be performed following PROM at term? |
Approximately 24 hours following membrane rupture
|
|
|
Contraindications for IOL |
Absolute: 1. Placenta previa 2. Severe fetal compromise 3. Deteriorating maternal condition i.e. due to major APH, severe pre eclampsia or cardiac disease Relative: 4. Breech presentation 5. Previous caesarean section 6. Preterm |
|
|
How is prostaglandin E2 is given during IOL |
Tablet or gel, inserted vaginally into the posterior fornix. Usually requires 2 doses, at least 6 hours apart Alternatively, a controlled-release pessary is also availabel and is left in place up to 24 hours |
|
|
Methods of IOL |
1. Vaginal prostaglandin E2 2. IV oxytocin infusion 3. ARM 4. 'membrane sweeping' usually requires combinations of those especially in primiparous |
|
|
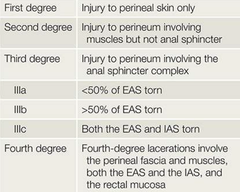
Grading of perineal tears |
|
|
|
Indication for instrumental delivery |
Fetal indications: 1. Suspected fetal compromise i.e. pathological CTG, abnormal pH Maternal indications: 2. Lack of progress in second stage of labor 3. Maternal exhaustion/distress/vomitting 4. Medical indications to avoid prolong pushing or valsalva i.e. cardiac problem, cerebral vascular disease. |
|
|
The ventouse compared to forceps is significantly more likely to be associatedwith:
|
1. Failure to achieve a vaginal delivery. 2. Cephalohaematoma (subperiosteal bleed). 3. Retinal haemorrhage. 4. Maternal worries about the baby |
|
|
The ventouse compared to forceps is significantly less likely to be associatedwith:
|
1. Use of maternal regional/general anaesthesia. 2. Significant maternal perineal and vaginal trauma. 3. Severe perineal pain at 24 hours. |
|
|
Example of non-rotational forceps |
Neville Barnes orSimpson forceps |
|
|
Example of rotational forceps |
Kiellandforceps |
|
|
Most common indications for caesarean section |
1. Previous caesarean 2. Malpresentation i.e. breech 3. Failure to progress in labor 4. Suspected fetal compromise in labor 5. Multiple pregnancy 6. placenta previa/abruptio |
|
|
Risk factors for post partum hemorrhage |
1. Uterine atony 2. Placenta previa / accreata 3. Previous multiple caesarean section 4. Perineal trauma 5. Full bladder 6. DIC |