Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
67 Cards in this Set
- Front
- Back
|
A patient is recieving 5mg morphine IR q 4 hours. Her pain is controlled, figure out a dose for ER tablets.
|
5mg morphine sulfate x 6 doses = 30 mg morphine sulfate
divide bid for MS contin = 15mg MS contin po bid |
|
|
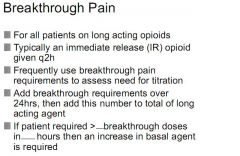
How do you figure out dose of IR morphine sulfate for breakthrough pain?
|
10-20% of morphine dose
|
|
|
The pt is using 6 tabs of 5mg morphine sulfate for breatkthough pain. He is also taking 30mg a day of MS contin. His pain is now 6/10, figure out new dose.
|
6 breakthrough doses x 5mg = 30mg morphine/day in breakthrough doses
pt aleady taking 15mg MS contin bid = 30mg/day 30mg daily + 30mg breakthrough = 60mg/day dose should now be 30mg MS contin po bid new prn dose should be 5-10mg |
|
|
Which of the following is accurate regarding acute pain?
A) acute pain follows injury to the body B) objective signs such as tachycardia, hypertension, and diaphoresis are often present C) establishing a diagnosis is a priority and treatment should be delayed until a diagnosis is made |
A) acute pain follows injury to the body
B) objective signs such as tachycardia, hypertension, and diaphoresis are oftn present |
|
|
what is the preferred route of delivery for opiod therapy?
|
oral
|
|
|
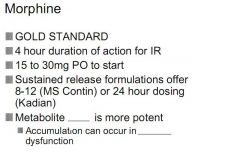
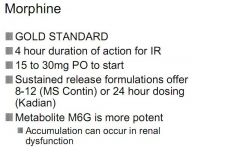
Which opioid agent is considered the gold statard, the agent to which all other agents are compared?
|
morphine
|
|
|
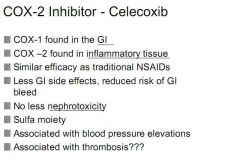
Which NSAID is available for parenteral use?
|
ketorolac
|
|
|
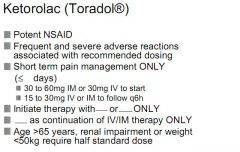
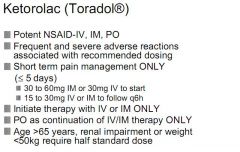
What are some limitations of ketorolac?
|
5 days total therapy
IV to PO conversions only (oral not to be initiated first) adverse rxns (anaphylaxis, GI ulceration) renal dosing |
|
|
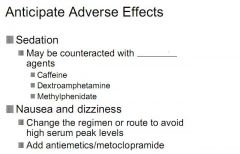
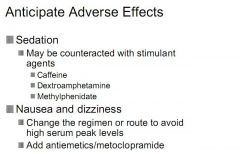
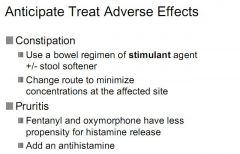
What are some methods to manage opioid induced side effects?
|
change opioid
add preventative agent alter route of administration to avoid high peak levels |
|
|
13. MT is receiving MS Contin 60mg q12h. She has been having trouble with nausea and the physician would like to try her on oxycodone. What dose of oxycodone would you recommend for her?
Dosing would be equivalent if using 30mg as equivalent for oxycodone but you would still need to reduce dose by 25% for incomplete cross tolerance |
120mg oxycodone x .75 = 90mg
Divide q12h for 45mg q12h – based on oxycodone availability use 40mg q12h Or, if using 20mg oxycodone as equivalent to 30mg morphine then, 120mg MS Contin daily = x x = 80mg oxycodone = 40mg po q12h 30mg 20mg with dose reduction 30mg po q12h |
|
|
The most common reason for unrelieved pain in the American healthcare system is:
|
failure to assess
|
|
|
SD’s pain is well controlled using 8 tabs Percocet 5/325 per 24 hours. Please convert this to MS Contin
|
8 tabs Percocet 5mg = 40mg oxycodone
40mg oxycodone/20mg (equianlagesic dose) = x mg / 30mg (morph. equi. dose) X = 60mg Since pain is well controlled, decrease by 25% to get 45mg morphine/day Easiest to go with 15mg q8h If using 30mg oxycodone equivalent then, 40mg oxycodone = 40mg morphine sulfate but need to reduce dose by 25% 40mg x 0.75 = 30mg use 15mg MS contin q 12h |
|
|
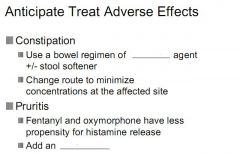
What should a bowel regimen include to prevent opioid induced constipation?
|
a stimulant agent +/- a stool softener
|
|
|
What is physical dependence?
|
a physiologic state of neuro-adaptiation which is characterized by the emergence of a withdrawal syndrome if druge use is stopped or decreased abruptly
|
|
|
what is Tolerence?
|
increased dose needed to feel same effect
|
|
|
what is addiction?
|
use of substances for their psychic effects and is chacterized by compulsive use despite harm
|
|
|
What is pseudoaddiction?
|
patter of drug seeking behavior of pain pts who are receiving inadequate pain management that can be mistaken for addiction
|
|
|
What is pain?
|
WHATEVER THE PT SAYS IT IS
|
|
|
what is neuropathic pain?
|
signal processing is abnormal
nervous system is impaired or injured |
|
|
What is allodynia?
|
experiencing pain to normally unpainful stimuli
|
|
|
What is aqtique?
|
fentanyl lolly pop approved for breathrough pain in cancer pts
|
|
|
When switching doses a new opiate dose should be reduced by how much?
|
25%
|
|
|
Is there a ceiling with opioid dosing?
|
NO
|
|
|
|
|
|
|
|
|
|
|

|

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|

|