Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
119 Cards in this Set
- Front
- Back
|
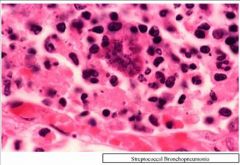
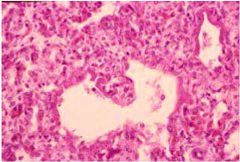
Acute Bronchopneumonia - The alveoli are filled with PMNs, fibrin and necrotic debris. The alveolar walls have begun to fragment producing the abscess cavity
|
|
|
Acute Epiglottitis
|
|
|
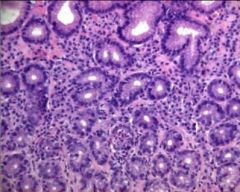
Acute Gastritis - Neutrophils in Glands
|
|
|
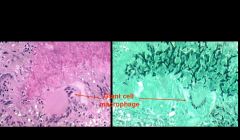
Acute Lobar Pneumonia - Pneumonia – neutrophil and macrophage exudate (grossly “grey hepatisation”)
|
|
|
Acute Supurative Pylonephritis
|
|
|
Acute Supurative Pylonephritis
|
|
|
Amoebic infasion of colonic crypt
|
|

|
Ascaris
|
|

|
ASCARIS LUMBRICOIDES
|
|

|
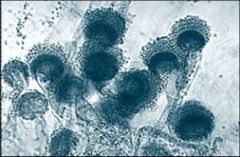
Aspergillus fumigatus
|
|
|
Aspergillus fumigatus
|
|

|
Bronchiectasis
|
|

|
Bronchopneumonia
|
|

|
Bronchopneumonia
|
|
|
Cerebral Toxoplasmosis
|
|
|
Bronchopneumonia
|
|
|
Cestode - Taenia Solium
|
|
|
Chronic Hepatitis B
|
|
|
|
CMS in Gastric Mucosa - Halo with Eosinophilic Inclusions
|
|
|
Coccidioides and Blastomyces
|
|
|
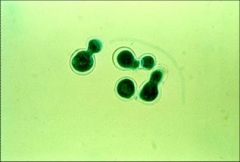
Coccidioides and Blastomyces - Budding
|
|
|
CMS in Gastric Mucosa - Halo with Eosinophilic Inclusions
|
|
|
CMV Inclusions - HALO
|
|
|
Cyst - Egg - Stained with PAS
|
|
|
Cocciodiodes Immitis - Spherule with Spores
|
|
|
Cocciodiodes Immitis - Spherule with Spores
|
|
|
Cyst - Eggs in Cyst
|
|
|
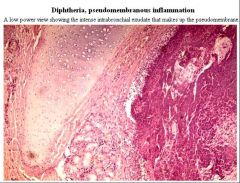
Diphtheria - Pseudomembranous Inflammation
|
|
|
Dyssentary - Crypt with inflammation inside
|
|
|
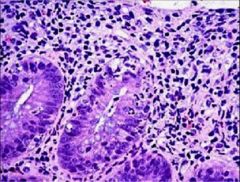
Dyssentery - Neutrophils in colonic crypt - cryptitis - acute colitis
|
|
|
Fungi
|
|
|
Gastritis
|
|
|
Gastritis - Neutrophils inside Foveoli
|
|
|
Gastrointestinal Fungal Infections
|
|
|
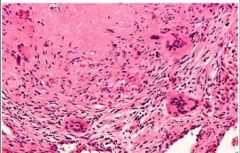
Giant Cell
|
|
|
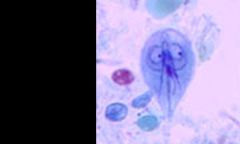
Giardia
|
|
|
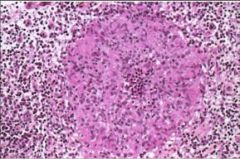
Granuloma - Not necrotizing because no necrosis in middle
|
|
|
Granuloma with Neutrophils - Bartonella Henselae
|
|
|
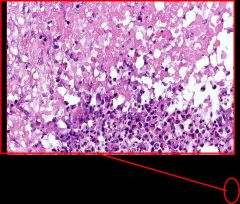
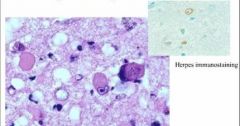
Herpes Encephalitis
|
|
|
Herpes Esophagitis
|
|
|
Herpes Virus - Multiple epithelial cells aggregated
|
|
|
Host Fibrosis trying to corner worm cyst
|
|
|
Host membrane against Cyst - middle is fibrosis with blood vessels - far right is Eosiniphils - left is Dense Fibrosis
|
|
|
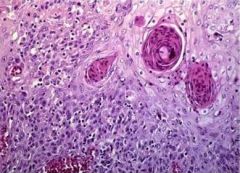
HPC Invasive SCC 2
|
|
|
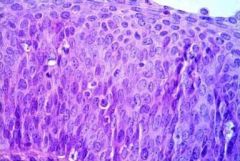
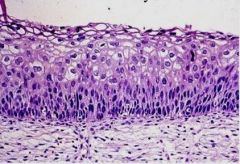
HPV Carcinoma In Situ
|
|
|
HPV Condyloma
|
|
|
HPV Invasic SCC
|
|
|
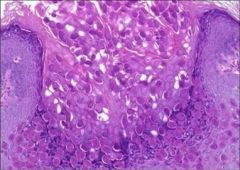
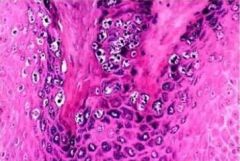
HPV Koilocytosis - Koilocytes are cells with halo around dark nucleus
|
|
|
HSV
|
|
|
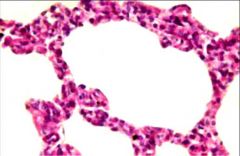
Interstitial inflammation of lung
|
|
|
Interstitial Viral Pneumonitis
|
|
|
Interstitial Viral Pneumonitis
|
|
|
Kidney - Left Mononuclear interstitial inflammation - Right is normal
|
|
|
Leishmania in Spleen
|
|
|
Leishmania inside cell
|
|
|
Lobular Pneumonia
|
|

|
Lobular Pneumonia
|
|
|
Lobular Pneumonia - Bacterial - Intralobular Septae with Neutrophils
|
|
|
Lung Aspergillosis
|
|
|
Lung Abscess
|
|
|
Lung Aspergillosis with Giant Cell Macrophage - HE
|
|
|
Lung Granuloma
|
|
|
Molluscum bodies inside epidermis
|
|
|
Molluscum bodies inside epidermis
|
|
|
Necrotizing Inflammation
|
|
|
Necrotizing Inflammation of Blood Vessel
|
|
|
Lung Necrotizing Granuloma
|
|
|
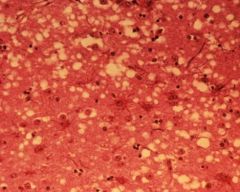
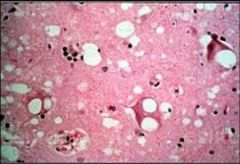
Neuron with Vacuolization - CJD
|
|
|
Neuron with Vacuolization - CJD
|
|
|
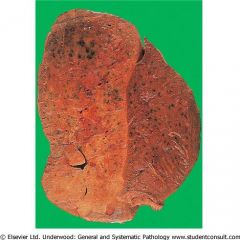
Pneumonia – fibrinopurulent exudate in alveoli (grossly “red hepatisation”)
|
|

|
Pseudomembranous colitis
|
|

|
Pseudomembranous colitis
|
|
|
Scarring of Lung - Pneumonia Complication
|
|

|
Scolex
|
|
|
Pulmonary Gangrene
|
|
|
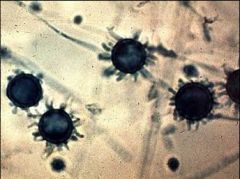
Scolex Parasite - Hooks visible
|
|
|
Shigella Dyssentery - Surface epithelium gone - neutrophils = acute inflammation
|
|
|
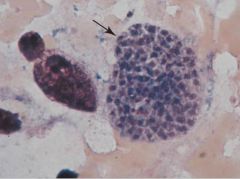
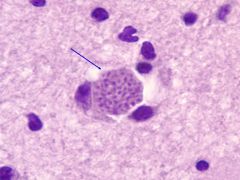
Toxoplasma Pseudocyst
|
|

|
Trematodes - Schistosoma
|
|

|
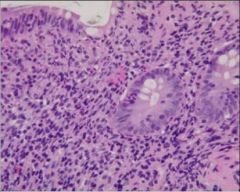
Trophozoite invasion of colonic crypt - narrow entry way and widens base above muscularis to form flask shape - Erosion at top
|
|
|
Tuberculosis
|
|
|
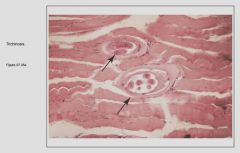
Trichinella spiralis - Trichinosis - Parasite between muscle fibers and fibrous tissue
|
|

|
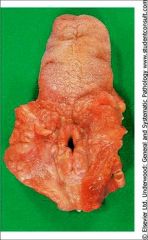
Typhoid Fever with Perforation of the Ileum
|
|

|
Typhoid Liver Nodules
|
|

|
Verruca Vulgaris
|
|
|
Viral Esophagitis
|
|
|
Verruca Vulgaris
|
|
|
West Nile Virus
|
|
|
Viral Pneumonia with Diffuse Fibrous Organization
|
|
|
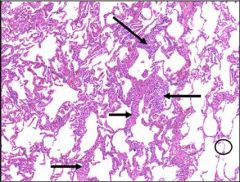
Viral Pneumonia with Linear Fibrin Membrane Deposits - 3 conditions can produce this - Viral Infection, ARDS, DAD (diffuse alveolar damage)
|
|
|
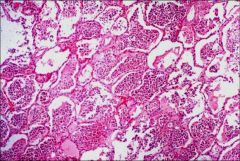
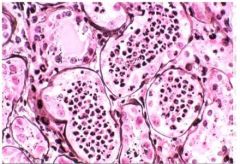
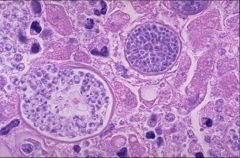
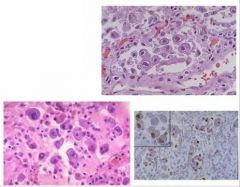
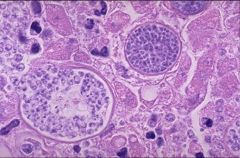
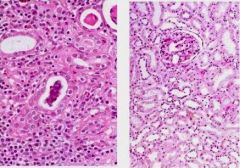
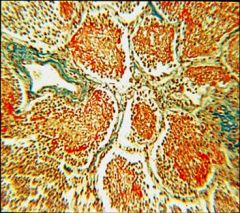
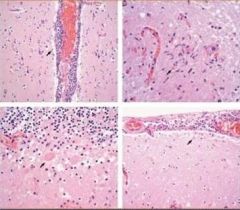
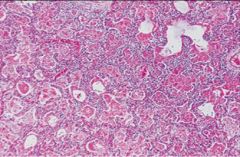
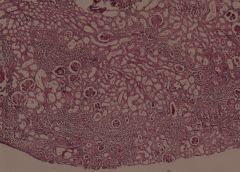
Cytomegalic inclusion disease (KIDNEY) X4
Interstitial mononuclear infiltration and tubular widening In the majority of the proximal convoluted tubules we see enlargement of the epithelial cells The nuclei of these cells are also enlarged and contain a huge inclusion body surrounded by a clear halo |
|
|
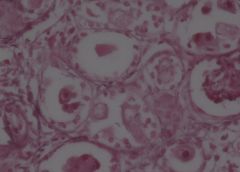
Cytomegalic inclusion disease (KIDNEY) X40
Interstitial mononuclear infiltration and tubular widening In the majority of the proximal convoluted tubules we see enlargement of the epithelial cells The nuclei of these cells are also enlarged and contain a huge inclusion body surrounded by a clear halo |
|
|
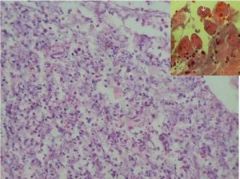
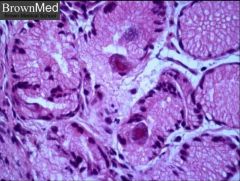
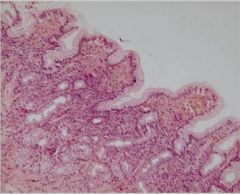
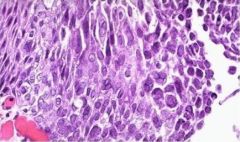
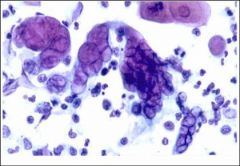
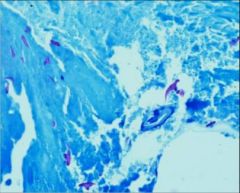
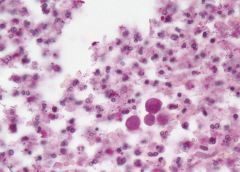
Candida in stomach. X2
This is a PAS stained slide of an ulceration of the stomach in a 60 year-old female. The mucosa and submucosa layers show neutrophil infiltration and fibrin. Also seen are macrophages, lymphocytes and necrotic epithelial cells. The main finding is that of large quantities of Candida Albicans, which shows two main forms: 1) Elongated nonbranching (pseudohyphae) 2) Round bodies (blastospores) This type of infection is seen mainly in Immunocompromised hosts |
|
|
Candida in stomach. X2
This is a PAS stained slide of an ulceration of the stomach in a 60 year-old female. The mucosa and submucosa layers show neutrophil infiltration and fibrin. Also seen are macrophages, lymphocytes and necrotic epithelial cells. The main finding is that of large quantities of Candida Albicans, which shows two main forms: 1) Elongated nonbranching (pseudohyphae) 2) Round bodies (blastospores) This type of infection is seen mainly in Immunocompromised hosts |
|
|
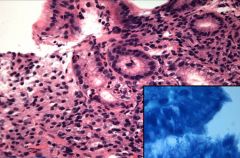
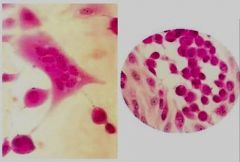
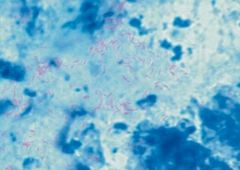
Candida in stomach. X20
This is a PAS stained slide of an ulceration of the stomach in a 60 year-old female. The mucosa and submucosa layers show neutrophil infiltration and fibrin. Also seen are macrophages, lymphocytes and necrotic epithelial cells. The main finding is that of large quantities of Candida Albicans, which shows two main forms: 1) Elongated nonbranching (pseudohyphae) 2) Round bodies (blastospores) This type of infection is seen mainly in Immunocompromised hosts |
|
|
Candida in stomach. X10
This is a PAS stained slide of an ulceration of the stomach in a 60 year-old female. The mucosa and submucosa layers show neutrophil infiltration and fibrin. Also seen are macrophages, lymphocytes and necrotic epithelial cells. The main finding is that of large quantities of Candida Albicans, which shows two main forms: 1) Elongated nonbranching (pseudohyphae) 2) Round bodies (blastospores) This type of infection is seen mainly in Immunocompromised hosts |
|
|
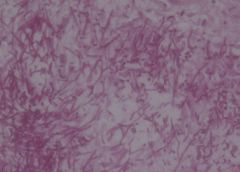
Candida in stomach. X40
This is a PAS stained slide of an ulceration of the stomach in a 60 year-old female. The mucosa and submucosa layers show neutrophil infiltration and fibrin. Also seen are macrophages, lymphocytes and necrotic epithelial cells. The main finding is that of large quantities of Candida Albicans, which shows two main forms: 1) Elongated nonbranching (pseudohyphae) 2) Round bodies (blastospores) This type of infection is seen mainly in Immunocompromised hosts |
|
|
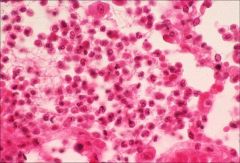
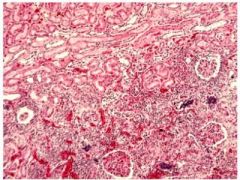
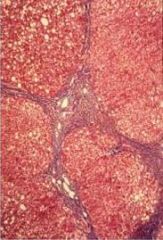
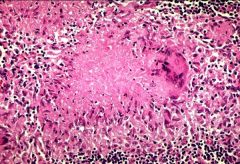
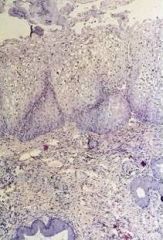
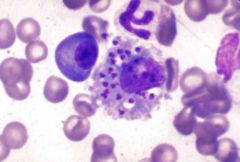
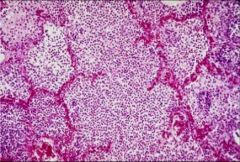
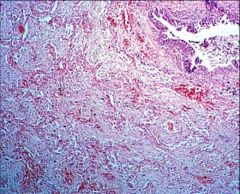
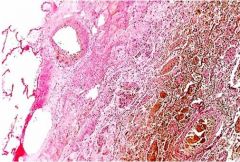
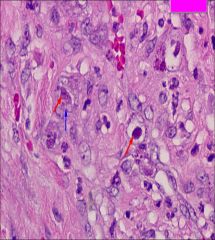
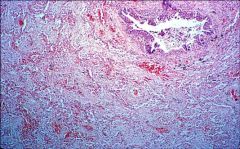
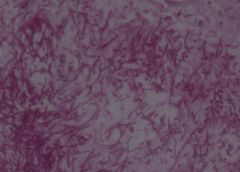
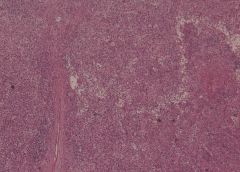
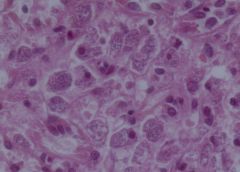
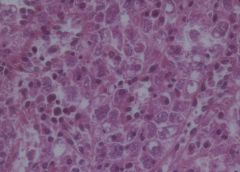
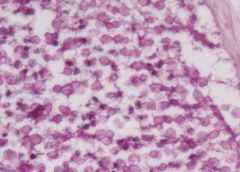
Kala Azar (Leishmaniasis) of spleen X4
On macroscopic examination extensive areas of infarction were found. On histology the normal architecture of the organ was not preserved. The white pulp was atrophic and the sinusoidal pattern of the red pulp was effected. Here and there blood vessels with hyalinization as well as areas of congestion and hemosiderin deposits were found. On high power exam many macrophages with several leishmania bodies were found. Those cells can be recognized due to the small eccentric nuclei and large cytoplasm. |
|
|
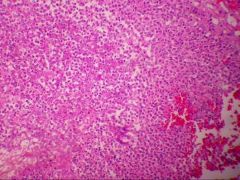
Kala Azar (Leishmaniasis) of spleen X60
On macroscopic examination extensive areas of infarction were found. On histology the normal architecture of the organ was not preserved. The white pulp was atrophic and the sinusoidal pattern of the red pulp was effected. Here and there blood vessels with hyalinization as well as areas of congestion and hemosiderin deposits were found. On high power exam many macrophages with several leishmania bodies were found. Those cells can be recognized due to the small eccentric nuclei and large cytoplasm. |
|
|
Kala Azar (Leishmaniasis) of spleen X40
On macroscopic examination extensive areas of infarction were found. On histology the normal architecture of the organ was not preserved. The white pulp was atrophic and the sinusoidal pattern of the red pulp was effected. Here and there blood vessels with hyalinization as well as areas of congestion and hemosiderin deposits were found. On high power exam many macrophages with several leishmania bodies were found. Those cells can be recognized due to the small eccentric nuclei and large cytoplasm. |
|

|
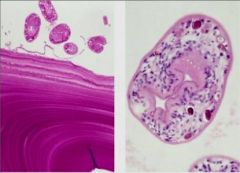
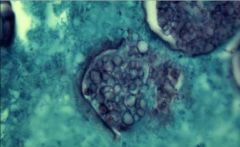
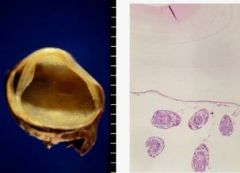
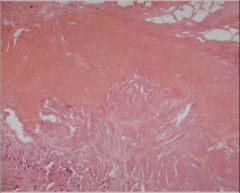
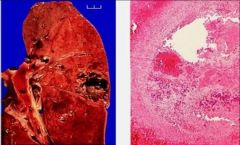
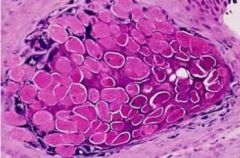
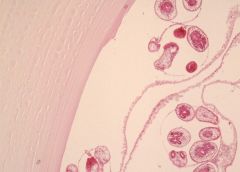
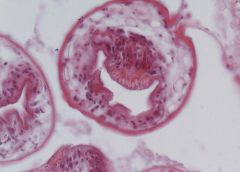
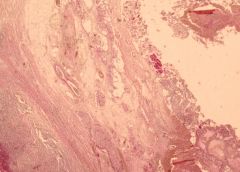
Hydatid cyst of liver x2
See cystic structre. Inside lumen see structure and another types of membrane. Have thick membrane on surface and content of cyst also has a membrane and round shape structures (scolices). Large laminated acellular thick membrane (all glycoproteins) and then a broken germinative layer and then scolices. Outside should see host layer with inflammation and inflammatory cells and fibrosis. |
|

|
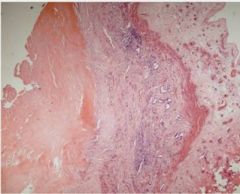
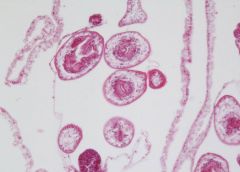
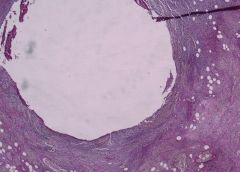
Hydatid cyst of liver
4x: see laminated thick but no cells inside. |
|
|
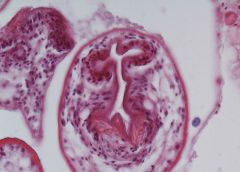
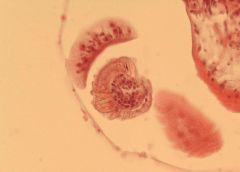
Hydatid cyst of liver
20x: See scolices – see hooks: like teeth. See membrane: germinative membrane – is epithelium. |
|
|
Hydatid cyst of liver
20x: See scolices – see hooks: like teeth. See membrane: germinative membrane – is epithelium. |
|
|
Hydatid cyst of liver
60x: See hooks that help attach. 60xb,c,d: see other cell @ diff angle– see hooks with lumen |
|
|
Hydatid cyst of liver
60x: See hooks that help attach. 60xb,c,d: see other cell @ diff angle– see hooks with lumen |
|
|
Hydatid cyst of liver
60x: See hooks that help attach. 60xb,c,d: see other cell @ diff angle– see hooks with lumen |
|
|
Hydatid cyst of liver
60x: See hooks that help attach. 60xb,c,d: see other cell @ diff angle– see hooks with lumen |
|

|
Hydatid cyst of liver
60x: See hooks that help attach. 60xb,c,d: see other cell @ diff angle– see hooks with lumen |
|
|
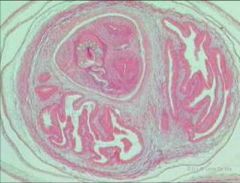
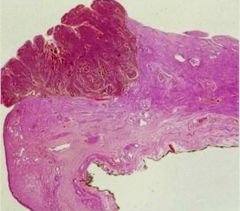
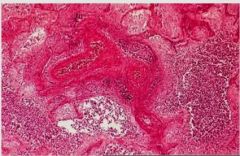
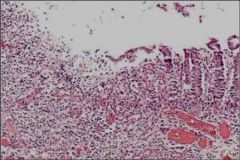
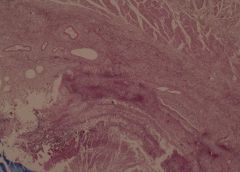
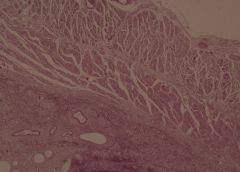
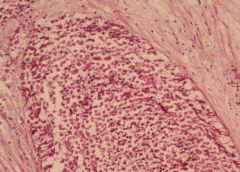
Acute suppurative appendicitis in amebiasis X2
These PAS-stained cross-sections of the appendix demonstrate innumerable vegetative parasites within vascular channels. The organism, entamoeba histolytica (15-40 microns in diameter), is ingested through contaminated water and food or direct fecal-oral contact. The parasites ability to encyts enables it to survive in most environments for weeks to months. Once excysted, the ameba invade the mucosa producing classic flask-shaped ulcers characteristically seen in the cecum and ascending colon, followed in order by the sigmoid, rectum and appendix. Penetration of the bowel wall may produce peritonitis, or pericolic amebomas; more frequently the parasites drain into the portal venous system producing hepatic abscesses, and potentially there after lung and brain abscesses. In this instance the suppurative inflammation has produced extensive ulceration and necrosis of the mucosa with a heavy polymorphonuclear leukocytic infiltration. The inflammatory process involves the entire thickness of the wall -there is also a fibrinosuppurative exudate over-lying the serosa. |
|
|
Acute suppurative appendicitis in amebiasis X2
These PAS-stained cross-sections of the appendix demonstrate innumerable vegetative parasites within vascular channels. The organism, entamoeba histolytica (15-40 microns in diameter), is ingested through contaminated water and food or direct fecal-oral contact. The parasites ability to encyts enables it to survive in most environments for weeks to months. Once excysted, the ameba invade the mucosa producing classic flask-shaped ulcers characteristically seen in the cecum and ascending colon, followed in order by the sigmoid, rectum and appendix. Penetration of the bowel wall may produce peritonitis, or pericolic amebomas; more frequently the parasites drain into the portal venous system producing hepatic abscesses, and potentially there after lung and brain abscesses. In this instance the suppurative inflammation has produced extensive ulceration and necrosis of the mucosa with a heavy polymorphonuclear leukocytic infiltration. The inflammatory process involves the entire thickness of the wall -there is also a fibrinosuppurative exudate over-lying the serosa. |
|
|
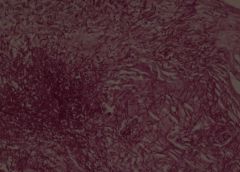
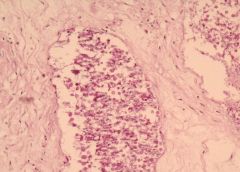
Acute suppurative appendicitis in amebiasis X10
These PAS-stained cross-sections of the appendix demonstrate innumerable vegetative parasites within vascular channels. The organism, entamoeba histolytica (15-40 microns in diameter), is ingested through contaminated water and food or direct fecal-oral contact. The parasites ability to encyts enables it to survive in most environments for weeks to months. Once excysted, the ameba invade the mucosa producing classic flask-shaped ulcers characteristically seen in the cecum and ascending colon, followed in order by the sigmoid, rectum and appendix. Penetration of the bowel wall may produce peritonitis, or pericolic amebomas; more frequently the parasites drain into the portal venous system producing hepatic abscesses, and potentially there after lung and brain abscesses. In this instance the suppurative inflammation has produced extensive ulceration and necrosis of the mucosa with a heavy polymorphonuclear leukocytic infiltration. The inflammatory process involves the entire thickness of the wall -there is also a fibrinosuppurative exudate over-lying the serosa. |
|
|
Acute suppurative appendicitis in amebiasis X10
These PAS-stained cross-sections of the appendix demonstrate innumerable vegetative parasites within vascular channels. The organism, entamoeba histolytica (15-40 microns in diameter), is ingested through contaminated water and food or direct fecal-oral contact. The parasites ability to encyts enables it to survive in most environments for weeks to months. Once excysted, the ameba invade the mucosa producing classic flask-shaped ulcers characteristically seen in the cecum and ascending colon, followed in order by the sigmoid, rectum and appendix. Penetration of the bowel wall may produce peritonitis, or pericolic amebomas; more frequently the parasites drain into the portal venous system producing hepatic abscesses, and potentially there after lung and brain abscesses. In this instance the suppurative inflammation has produced extensive ulceration and necrosis of the mucosa with a heavy polymorphonuclear leukocytic infiltration. The inflammatory process involves the entire thickness of the wall -there is also a fibrinosuppurative exudate over-lying the serosa. |
|
|
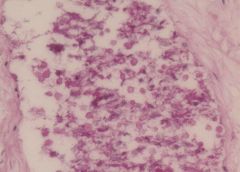
Acute suppurative appendicitis in amebiasis X40
These PAS-stained cross-sections of the appendix demonstrate innumerable vegetative parasites within vascular channels. The organism, entamoeba histolytica (15-40 microns in diameter), is ingested through contaminated water and food or direct fecal-oral contact. The parasites ability to encyts enables it to survive in most environments for weeks to months. Once excysted, the ameba invade the mucosa producing classic flask-shaped ulcers characteristically seen in the cecum and ascending colon, followed in order by the sigmoid, rectum and appendix. Penetration of the bowel wall may produce peritonitis, or pericolic amebomas; more frequently the parasites drain into the portal venous system producing hepatic abscesses, and potentially there after lung and brain abscesses. In this instance the suppurative inflammation has produced extensive ulceration and necrosis of the mucosa with a heavy polymorphonuclear leukocytic infiltration. The inflammatory process involves the entire thickness of the wall -there is also a fibrinosuppurative exudate over-lying the serosa. |
|
|
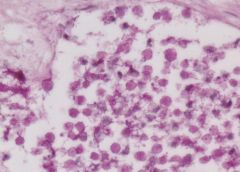
Acute suppurative appendicitis in amebiasis X60
These PAS-stained cross-sections of the appendix demonstrate innumerable vegetative parasites within vascular channels. The organism, entamoeba histolytica (15-40 microns in diameter), is ingested through contaminated water and food or direct fecal-oral contact. The parasites ability to encyts enables it to survive in most environments for weeks to months. Once excysted, the ameba invade the mucosa producing classic flask-shaped ulcers characteristically seen in the cecum and ascending colon, followed in order by the sigmoid, rectum and appendix. Penetration of the bowel wall may produce peritonitis, or pericolic amebomas; more frequently the parasites drain into the portal venous system producing hepatic abscesses, and potentially there after lung and brain abscesses. In this instance the suppurative inflammation has produced extensive ulceration and necrosis of the mucosa with a heavy polymorphonuclear leukocytic infiltration. The inflammatory process involves the entire thickness of the wall -there is also a fibrinosuppurative exudate over-lying the serosa. |
|
|
Acute suppurative appendicitis in amebiasis X40
These PAS-stained cross-sections of the appendix demonstrate innumerable vegetative parasites within vascular channels. The organism, entamoeba histolytica (15-40 microns in diameter), is ingested through contaminated water and food or direct fecal-oral contact. The parasites ability to encyts enables it to survive in most environments for weeks to months. Once excysted, the ameba invade the mucosa producing classic flask-shaped ulcers characteristically seen in the cecum and ascending colon, followed in order by the sigmoid, rectum and appendix. Penetration of the bowel wall may produce peritonitis, or pericolic amebomas; more frequently the parasites drain into the portal venous system producing hepatic abscesses, and potentially there after lung and brain abscesses. In this instance the suppurative inflammation has produced extensive ulceration and necrosis of the mucosa with a heavy polymorphonuclear leukocytic infiltration. The inflammatory process involves the entire thickness of the wall -there is also a fibrinosuppurative exudate over-lying the serosa. |
|
|
Acute suppurative appendicitis in amebiasis X60
These PAS-stained cross-sections of the appendix demonstrate innumerable vegetative parasites within vascular channels. The organism, entamoeba histolytica (15-40 microns in diameter), is ingested through contaminated water and food or direct fecal-oral contact. The parasites ability to encyts enables it to survive in most environments for weeks to months. Once excysted, the ameba invade the mucosa producing classic flask-shaped ulcers characteristically seen in the cecum and ascending colon, followed in order by the sigmoid, rectum and appendix. Penetration of the bowel wall may produce peritonitis, or pericolic amebomas; more frequently the parasites drain into the portal venous system producing hepatic abscesses, and potentially there after lung and brain abscesses. In this instance the suppurative inflammation has produced extensive ulceration and necrosis of the mucosa with a heavy polymorphonuclear leukocytic infiltration. The inflammatory process involves the entire thickness of the wall -there is also a fibrinosuppurative exudate over-lying the serosa. |
|
|
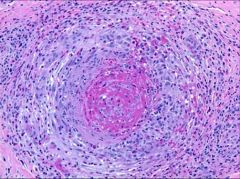
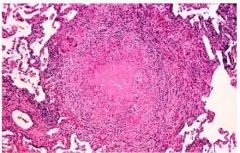
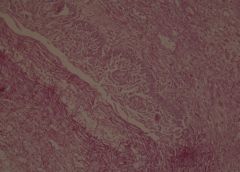
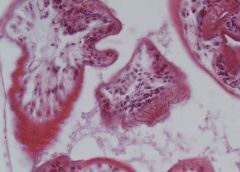
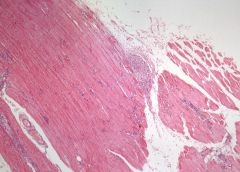
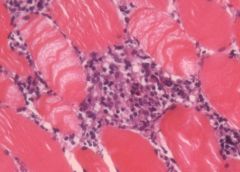
Parasitic myostitis (Trichinosis) X4
4x: See skeletal muscle fibres: long fibres and nuclei at periphery of fibres. See occasionally too many cells between muscle fibres. See in middle a localized inflammatory fossa – a granuloma with epithelioid cells and giant cells. Trichinosis is caused by ingestion of inadequately cooked meat containing viable cysts of trichinella spiralis. The larvae, released in the intestine, penetrate the lacteals and eventually are drained into the blood. Dissemination and widespread cell damage may produce an interstitial myocarditis, an interstitial eosinophilic pneumonitis or meningitis and gliosis. However, the most important localization is within skeletal muscles, where the larvae penetrate a muscle cell, become encysted, and in this manner may survive in a dormant state for years, protected in the “Nurse cell” from both immune an phagocytic destruction. Death of the larva and its “Nurse cell” evokes and inflammatory reaction, followed in time by calcification of the larva, thus permitting retrospective diagnosis. |
|
|
Parasitic myostitis (Trichinosis)
|