Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
10 Cards in this Set
- Front
- Back
|
What are the clinical SXS of bladder cancer?
|
1) Painless hematuria
2) Urinary frequency, urgency, dysuria 3) Cystitis, Pyelonephritis (obstruction/retention) 4) Lymph node mets (rare) |
|
|
Is a screening test available for bladder cancer?
|
Cystoscopy, however bladder cancer is so rare screening is limited to pts with a PRIOR DX of bladder cancer.
|
|
|
What are the risk factors for bladder cancer?
|
1) Toxins (alinine dyes)
2) Drugs (cytoxan, phenacetin) 3) Smoking 4) Schistosomiasis 5) Prior hx of bladder CA |
|
|
What are the incidence percentages for papillary vs. transitional cell carcinomas?
|
Papillary CA: 80%
Transitional Cell: 20% |
|
|
Why are bladder cancer patients followed for so many years?
|
Bladder CA has a very high recurrence rate (50% or greater in all cases)
|
|
|
What are the subtypes of Urothelial/Transitional Cell CA?
|
1) Flat (carcinoma in situ)
2) Papillary 3) Invasive |
|
|
What is the "Field Effect" in relation to bladder CA?
|
Entire urothelium is affected by carcinogen, and is therefore at equal risk. Bladder CA is therefore often multifocal in origin.
|
|
|
What pathologic features are important in determining Bladder CA patient management?
|
1) Tumor grade
2) Tumor stage 3) Tumor location |
|
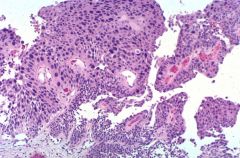
Name the pathology!
|
High-Grade Papillary Carcinoma
* Note variation in size/shape of nuclei * Presence of papillary "fibro-vascular" structures |
|
|
How is bladder cancer treated?
|
Low Grade - scoop it out (TURB)
Hi Grade but IntraBladder - "BCG" attenuated bacteria, makes immune response to tumor Muscle Invasive - radical cystectomy Mets - MVAC (Methotrexate, Vinblastine, Adriomycin, Cytoxan) |