Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
188 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
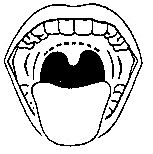
Mallampati Classification
|
Airway Evaluation Classification
Class I: Visualization of Soft Palate, Fauces, Uvula, Anterior and Posterior Tonsilar Pillars (Fauces = Mucosa over Palatopharyngeus & Palatoglossus) Class II: Soft Palate, fauces, uvula Class III: Soft Palate, Base of Uvula Class IV: Cannot See soft palate |
#surgicalpt
|
|
|
Class I Airway
|
Mallampati Classification: Visualization of Soft Palate, Fauces, Uvula, Anterior and Posterior Tonsilar Pillars
|
#surgicalpt
|
|
|
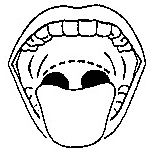
Class II Airway
|
Mallampati Classification: Soft Palate, fauces, uvula
|
#surgicalpt
|
|
|
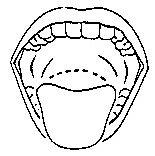
Class III Airway
|
Mallampati Classification:
Soft Palate, Base of Uvula |
#surgicalpt
|
|
|
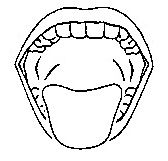
Class IV Airway
|
Mallampati Classification:
Cannot See soft palate |
#surgicalpt
|
|
|
Mallampati Airway Classification Class I
Visualization of Soft Palate, Fauces, Uvula, Anterior and Posterior Tonsilar Pillars |
|
|
|
Mallampati Airway Classification Class 2
Visualization of Soft Palate, Fauces, Uvula |
|
|
|
Mallampati Airway Classification Class 3
Visualization of Soft Palate, Base of Uvula |
|
|
|
Mallampati Airway Classification Class 4
Cannot See Soft Palate |
|
|
|
Cardiac Risk Assessment
|
<35 yo & ∅ Cardiac Hx: EKG
--- if normal → pt good >35 or Cardiac Hx: EKG ± Stress test, Echo |
#surgicalpt
|
|
|
Goldman's Risk Assessment for Non-Cardiac Surgery
Level 1: What Are the Critera Level 2: How Many Points Level 3: Interpret the Totals |
S3 gallop or JVD: 11 pts
MI w/in 6 mo: 10 pts >5 PVC's/ min: 7 pts Neither Sinus Rhthym nor SR w/ APC's: 7 pts >70 yo: 5 pts Emergent Operation: 4 pts Intrathoracic, intraperitonal or aortic surgery: 3 pts Significant Aortic Stenosis: 3 pts Poor General Medical Condition: 3 pts ≤5pts → class 1: 1% Risk of life threatening complixns 6-12 pts → class 2: 5% risk 13-25 → class 3: 11% risk >25 → class 4: 22% risk page 19 |
#surgicalpt
#mastercard #needsbreakdown |
|
|
Aortic Stenosis on the Pre-Op Eval
|
↑ risk for Ischemia → MI → Sudden Death
3 points on Goldman's Risk Assessment for Non-Cardiac Surgery |
#surgicalpt
|
|
|
Abdominal Surgery & Respiratory Function
|
↓ Vital Capacity by 50% and Functional Risidual Capacity by 30%
|
#surgicalpt
|
|
|
Risk Factors for Pulmonary Complications
|
Known Pulmonary Dz
abnormal PFT's: FEV <11, max breathing capacity < 50% predicted, FEV1 <70% predicted, VO2 <20 Smoking >60 yo Obesity Uppder abdominal or thoracic Surgery Long OR time So an Obese 60 yo COPDer |
#surgicalpt
|
|
|
Decreasing Pulmonary Complications
|
Reduce Risk:
↓ smoking 8 weeks pre-op optimize bronchodilator therapies incentive spirometry early post-op ambulation chest physical therapy/OMM DVT prophylaxis by SCD sequential compression device and subcu heparin NB: because their mechanism is to acccentuate systemic thrombolysis, one SCD will work as well as 2 if one lg is injured |
#surgicalpt
|
|
|
Mortality of elderly pt w/ post-op pneumonia
|
pneumonia has highest mobidity/mortality of all pulmonary complications
50% in elderly |
#quickfact
|
|
|
Platelet Count vs. Bleeding
|
>50k: unlikely w/ hemostasis
>20k: excessive surgical bleeding >10k: spontaneous bleeding <10k massive spontaneous GI bleed NB: BUN >100 → nonfnx platlets --corrected by DDVAP ie Desmopressin 1 pack of platelets ≈ ↑ 10k |
#surgicalpt
|
|
|
Mortality of Pt:
NH3 >150 |
75%
|
#surgicalpt
#quickfact |
|
|
Mortality of Pt
INR > 2 |
50%
|
#surgicalpt
#quickfact |
|
|
Return of Bowel Function: Timeline
|
Small Intestine
then Stomach then Colon |
#quickfact |
|
|
Tappered vs Cutting Needles
|
Cutting needle: sharp tip with sharp edges. Used for skin sutures.
Tapered Needles: sharp tip but smooth, round edges: less traumatic. Used for deeper (non-skin) ts. |
#suturing
|
|
|
acholic stool
|
light-colored stool as a result of decreased bile content
|
#recall
#dissected |
|
|
light-colored stool as a result of decreased bile content
|
acholic stool
|
#recall
#dissected |
|
|
amaurosis fugax
|
transient visual loss in one eye
|
#recall
#dissected |
|
|
bariatric
|
baro = weight
iatro = doctor the medicine/surgery of weight loss |
#recall
|
|
|
celiotomy
|
incision into peritoneal cavity
aka laprotomy |
#recall
|
|
|
enterolysis
|
lysis of peritoneal adhesions
NB: enteroclysis = contrast study of small bowel |
#recall
#dissected |
|
|
vocab: lysis of peritoneal adhesions
|
enterolysis
NB: enteroclysis = contrast study of small bowel |
#recall
#dissected |
|
|
Excisional Biopsy
|
Removal of Entire Tumor
|
#recall
#dissected |
|
|
Vocab: Removal of Entire Tumor
|
Excisional Biopsy
|
#recall
#dissected |
|
|
vocab: transient visual loss in one eye
|
amaurosis fugax
|
#recall
#dissected |
|
|
Incisional Biopsy
|
Biopsy with only a slice of tumor removed
|
#recall
#dissected |
|
|
Vocab: Biopsy with only a slice of tumor removed
|
Incisional Biopsy
|
#recall
#dissected |
|
|
Inspissated
|
Hard
|
#recall
|
|
|
Lieno-
|
slpenic
|
#recall
|
|
|
-orraphy
|
surgical repair
|
#recall
|
|
|
-pexy
|
fixation into place
|
#recall
|
|
|
Plicae circulares vs semilunares
|
ciculares: small intestine
semilunares: large intestine |
#recall
#dissected |
|
|
Plicae semilunares vs circulares
|
ciculares: small intestine
semilunares: large intestine |
#recall
#dissected |
|
|
Folds in intestinal mucosa
|
plicae ciculares: small intestine
plicae semilunares: large intestine |
#recall
#dissected |
|
|
Succus
|
Fluid
eg succus entericus is fluid from bowel lumen |
#recall
#dissected |
|
|
Tenesmus
|
urge to defecate with ineffectual straining
|
#recall
#dissected |
|
|
urge to defecate with ineffectual straining
|
tenesmus
|
#recall
#dissected |
|
|
Succus Entericus
|
fluid from bowel lumen
|
#recall
#dissected |
|
|
W → D
|
Wet to Dry Dressing
damp gauze dressing placed on a wound and removed after the dressing dries to the wound, providing microdebridement |
#recall
|
|
|
Constant dullness to percussion in Left Flank/LUQ and resonance to percussion in right flank
|
Ballance's Sign
Seen with Splenic Rupture/Hematoma |
#recall
#dissected |
|
|
Physical Finding indicated of Splenic Rupture/Hematoma
|
Ballance's sign
constant dullness to percussion in left flank/LUQ and resonance to percussion in right flank. |
#recall
#dissected |
|
|
Beck's Triad
|
Of cardiac tamponade
1. JVD 2. ↓ Heart Sounds 3. ↓ BP |
#recall
#dissected |
|
|
JVD w/ ↓ BP and soft heart sounds
|
Beck's triad of cardiac tamponade
|
#recall
#dissected |
|
|
Physical Exam Findings of Cardiac Tamponade
|
Beck's Triad
1. JVD 2. ↓ Heart Sounds 3. ↓ BP |
#recall
#dissected |
|
|
Bergman's Triad
|
Fat Emboli Sro
1. Mental Status Changes 2. Petechiae often in Axilla 3. Dyspnea |
#recall
#dissected |
|
|
SOB, mental status deterioration and thoracic petechiae
|
Bergman's triad of Fat Emboli
|
#recall
#dissected |
|
|
Fat Emboli Physical Exam Clues
|
Bergman's Triad
1. Mental Status Changes 2. Petechiae often in Axilla 3. Dyspnea |
#recall
#dissected |
|
|
Blumer's Shelf
|
Metastatic Dz to rectouterine pouch of douglas or rectovesical pouch. creates a shelf palpable on DRE
|
#recall
#dissected |
|
|
Palpable "shelf" on DRE
|
Blumer's Shelf
Metastatic Dz to rectouterine pouch of douglas or rectovesical pouch. |
#recall
#dissected |
|
|
Boas' sign
|
right subscapular pain 2° to cholelithiasis
|
#recall
#dissected |
|
|
right subscapular pain 2° to cholelithiasis
|
Boas' sign
|
#recall
#dissected |
|
|
Borchardt's triad
|
Gastric Volvulus
1. Emesis followed by retching 2. Epigastric Distention 3. Failure to pass NGT |
#recall
#dissected |
|
|
Pt vomits and retches. Epigastrium is distended by NGT will not insert.
|
Borchardt's triad of Gastric Volvulus
|
#recall
#dissected |
|
|
Presentation of Gastric Volvulus
|
Borchardt's triad
1. Emesis followed by retching 2. Epigastric Distention 3. Failure to pass NGT |
#recall
#dissected |
|
|
Carcinoid Triad
|
Flushing
Diarrhea Right-sided Heart Failure |
#recall
#dissected |
|
|
Right Sided Heart Failure
Diarrhea Flushing |
Carcinoid Triad
|
#recall
#dissected |
|
|
Charcot's Triad
|
Cholangitis:
1. Fever 2. Jaundice 3. RUQ pain |
#recall
#dissected |
|
|
Pt presents with RUQ, fever and jaundice.
|
Chacot's Triad of Cholangitis
|
#recall
#dissected |
|
|
Cholangitis presentation
|
Charcot's Triad
1. Fever 2. Jaundice 3. RUQ pain |
#recall
#dissected |
|
|
Courvoisier's Law
|
Enlarged nontender gallbladder = obstruction of common bile duct, most commonly pancreatic cancer
Not seen 2° to cholelithiasis "Koor-vwah-ze-ay" |
#recall
#dissected |
|
|
Enlarged non-tender gallbladder
|
Courvoisier's Law
obstruction of common bile duct, most commonly pancreatic cancer Not seen 2° to cholelithiasis "Koor-vwah-ze-ay" |
#recall
#dissected |
|
|
Cullen's Sign
|
Periumbilical bruising 2° to retroperitoneal hemorrhage
think acute hemorrhagic pancreatitis |
#recall
#dissected |
|
|
periumbilical bruising
|
Cullen's Sign 2° to retroperitoneal hemorrhage
think acute hemorrhagic pancreatitis |
#recall
#dissected |
|
|
Cushing's Triad
|
of Increased Intracranial Pressure
HTN, bradycardia, irregular respirations |
#recall
#dissected |
|
|
Presentation of Increased ICP
|
Cushings Triad
HTN, Bradycardia, irregular respirations |
#recall
#dissected |
|
|
Pt is bradycardic, hypertensive and has irregular breathing pattern
|
Cushing's Triad of Increased ICP
|
#recall
#dissected |
|
|
Dance's sign
|
empty RLQ in children with ileocecal intussusception
|
#recall
#dissected |
|
|
Presentation of ileocecal intussusception
|
Dance's sign: empty RLQ
|
#recall
#dissected |
|
|
Empty RQL
|
Dance's sign of ileocecal intussusception
|
#recall
#dissected |
|
|
Fothergill's Sign
|
mass palpable while there is tension on abdominal musculature (sitting halfway upright) → mass is in abdominal wall
used to differentiate intra-abdominal masses from intramural masses |
#recall
#dissected |
|
|
differentiating between intra-abdominal mass and mass in abdominal wall
|
Forthergill's Sign
mass palpable while there is tension on abdominal musculature (sitting halfway upright) = mass is in abdominal wall |
#recall
#dissected |
|
|
Fox's sign
|
echymosis of inguinal ligamnet seen in retroperitoneal bleeding
|
#recall
#dissected |
|
|
Ecchymosis of inguinal ligmanet
|
Fox's sign, seen with retroperitoneal bleeding
|
#recall
#dissected |
|
|
Goodsall's rule
|
anal fistulae course in a straight path anteriorly and a curved path posteriorly from midline
|
#recall
#dissected |
|
|
course of anal fistulae
|
Goodsall's rule: anal fistulae course in a straight path anteriorly and a curved path posteriorly from midline
|
#recall
#dissected |
|
|
Grey Turner's Sign
|
Ecchymosis of Flank in pts with retroperitoneal hemorrhage
|
#recall
#dissected |
|
|
ecchymosis of the flank in absence of flank trauma
|
Grey Turner sign of retroperitoneal hemorrhage
|
#recall
#dissected |
|
|
Haaman's Sign
|
Crunching sound on auscultation of heart from ephysematous mediastinum/pneumomediastium
|
#recall
#notdissected |
|
|
Howship-Romberg sign
|
Pain along the inner aspect of the thigh
seen with obturator hernia as a result of nerve compression |
#recall
#dissected |
|
|
Presentation of an obturator hernia
|
Howship-Romberg sign: pain along inner aspect of thigh
|
#recall
#dissected |
|
|
Pt presents with pain along inner aspect of thigh
|
Howship-Romberg sign of obturator hernia (nerve compression)
|
#recall
#dissected |
|
|
Kehr's sign
|
severe left shoulder pain in pts with splenic rupture
|
#recall
#dissected |
|
|
Severe left shoulder pain in pt with blunt trauma
|
Kehr's sign of splenic rupture
|
#recall
#dissected |
|
|
Kelly's sign
|
visible peristalsis of ureter in resposne to contact (squeezing, retraction) used to identify ureter during surgery
|
#recall
#dissected |
|
|
How can you ID the ureter during surgery
|
Kelly's sign: visible peristalsis irt squeezing or retratction
|
#recall
#dissected |
|
|
Where does the colon perforate?
|
Cecum because increased radius
Laplace's law: Wall tension = Pressure * Radius |
#recall
#dissected |
|
|
Laplace's Law
|
Wall tension = pressure * radius
(eg colon preferentially perforates at cecum because of large radius) |
#recall
#dissected |
|
|
Lower quadrant pain mid-cycle
|
Mittelschmerz, due to ovluation
|
#recall
#dissected |
|
|
Mittelschmerz pain
|
lower quadrant pain midcycle due to ovulation
|
#recall
#dissected |
|
|
Obturator sign
|
pain with internal rotation of leg (hip and knee flexed)
seen in pts with appendicits/pelvic abscess |
#recall
#dissected |
|
|
Pain elicited by internal rotation of leg (hip & knee bent)
|
Obturator sign of appendicitis or pelvic abscess
|
#recall
#dissected |
|
|
Catgut sutures
|
purified collagen from intestines of cows or sheep (not cats)
come as plain or chromic chromic has been treated with chromium salts → ↑ collagen crosslinks → more resistant to breakdown |
#recall
|
|
|
vicryl suture
|
absorbable
braided microfilaments of polymerized (lactide + glycoside) strength retention 60% at 2 weeks 10% at 4 weeks NB: never use purple for skin closure → tatooing |
#recall
|
|
|
PDS
|
absorbable
monofilament polymer of polydioxanone (fishing line) strength retention: 75% at 2 weeks 50% at 4 weeks 25% at 6 weeks takes 6 months to completely resorb |
#recall
|
|
|
Silk
|
non-absorbable suture
|
#recall
|
|
|
Prolene
|
non-absorbable suture
|
#recall
|
|
|
nylon
|
nonabsorbable fishing line
NB: PDS is absorbable "fishign line" |
#recall
|
|
|
monocryl
|
absorbable monofilament suture
|
#recall
|
|
|
What kind of suture should be used for biliary tract or urinary tract:
|
absorbable - else nidus for stone formation
|
#recall
|
|
|
Absorbable vs Non-Absorbable Suture Materials
(List) |
Absorbable: Catgut, Vicryl, PDS, Monocryl
Non-absorbable: Silk, Prolene, Nylon |
#recall
|
|
|
Delayed Primary Closure
|
aka tertiary intention
a wound is allowed to remain opened for a time → allows for debridement & wound care to ↓ bacterial count; wound is then closed. |
#recall
|
|
|
GIA device
|
gastrointestinal anastomosis device
laws two rows of staples and automatically cuts between them |
#recall
|
|
|
OP note
|
PPP SAFE DISC
Preop Dx Post-Op Dx Procedure Surgeon & Assistance Anesthesia: GET (general endotracheal) Fluid I/O EBL Drains Specimen Complixns |
|
|
|
Suture Ligature
|
aka Stick Tie
Suture anchored by passing needle through large vessel before wrapping it around vessel (ultimately occluding vessel). Prevents knot slippage. |
#recall
|
|
|
Stick Tie
|
ie Suture Ligature
Suture anchored by passing needle through large vessel before wrapping it around vessel (ultimately occluding vessel). Prevents knot slippage. |
#recall
|
|
|
Retention Suture
|
Large Suture (2-0) tied full thickness through abdominal wall minus periteonum. Used for dehiscence-risk wounds.
|
#recall
|
|
|
How long before a suture leaves a scar on skin?
|
10 days.
sutures should be removed as soon as wound healed enough to withstand normal wear and tear. |
#recall
|
|
|
How long should a suture be left in?
|
Face: 5 days
Abdomen: 7 days Extremities: 10 days Back & Joints: 14 days sutures should be removed as soon as wound healed enough to withstand normal wear and tear. 10 days = scar |
#recall
|
|
|
Placing an NG tube
--what length? --process --how can you be sure? --when can you feed? |
Length: w/ pts head turned to side, from nose around ear and down to 5 cm beyond xiphoid
Lube tube and advance it straight back. Have pt tilt head forward and drink water with a straw. Be sure: inject air while auscultating epigastrium. listen for "swishing" Want to feed? get a CXR first! |
#recall
|
|
|
Kocher incision
|
right subcostal for open cholecystectomy.
|
#recall
|
|
|
Rocky-Davis incision
|
Transverse invision across Mcburney's point
|
#recall
|
|
|
Pfannenstiel incision
|
Low transverse incision (supra-pubic) with abdominal muscles retracted laterally. Used for gyn.
|
#recall
|
|
|
Lithotomy
|
a surgical position, pt lying supine with legs spread
|
#recall
|
|
|
Surgical Pt Position: Supine with hips & knees flexed, legs spread, ankles in stirrups
|
lithotomy
|
#recall
|
|
|
Pt going into surgery already on meds
|
discontinue anti-hypertensives, oral hypoglycemics, insulin.
Diabetics can be on 1/2 dose lente + D5 NS IV |
#recall
|
|
|
Bowel Prep
|
GoLYTELEY, oral neomycin + erythromycin + IV antibiotics before invision.
No actual data to support use. |
#recall
|
|
|
Who gets a pre-op EKG?
|
>40 yo
|
#recall
|
|
|
Billroth procedure
|
Billroth 1: antrectomy (pylorectomy) + gastroduodenostomy
Biillroth 2: antrectomy + gastrojujunostomy Pn: 1 has one exit from stomach, 2 has 2. |
#recall
|
|
|
Brooke ileostomy
|
ileostomy folded onto itself to protrude form abdomen ~2cm to allow easy appliance placement & collection of succus
|
#recall
|
|
|
Bassini herniorrhaphy
|
approximation of transversus abdominis aponeurosis & conjoint tendon to reflection of (Poupart's) Inguinal ligament
|
#recall
|
|
|
McVay Herniorrhaphy
|
approximating transversus abodminus and conjoint tendon to Cooper's ligament (pubic perisoteum)
|
#recall
|
|
|
Shouldice herniorrhaphy
|
imbrication of transversalis fascia, transversus abdominis aponeurosis and conjoint tendon and approximation of the transversus abdominis aponeurosis and conjoint tendon to inguinal ligament
|
#recall
|
|
|
plug and patch herniorrhaphy
|
prosthetic plug pushes hernia sac in and then is covered with a prosthetic patch
|
#recall
|
|
|
APR
|
Adomino-Perineal Resection.
Removal of rectum and sigmoid colon through adominal and perineal incisions → colostomy. Used for rectal cancers <8cm from anal verge. |
#recall
|
|
|
LAR
|
Low Anterior Resection.
Resection of low rectal tumors through an anterior abomdinal incision |
#recall
|
|
|
Hartmann's procedure
|
Proximal colostomy + distal stapled off colon/rectum which is not removed.
|
#recall
|
|
|
Mucous fistula
|
distal end of colon brought ot abdominal skin as a stoma.
proximal end → colostomy |
#recall
|
|
|
Kocher maneuver
|
dissection of duodenum from right-sided peritoneal attachment to allow mobilization and visualization of the back of duodenum/pancrea
|
#recall
|
|
|
Puestow procedure
|
side-to-side anastamosis of jejunum to filleted pancreas.
|
#recall
|
|
|
Stamm gastrostomy
|
gastrostomy placed by open surgical incision and tacked to the abodminal wall.
|
#recall
|
|
|
Enterolysis
|
Lysis of peritoneal adhesions
|
#recall
|
|
|
Simple Mastectomy
|
removal of breast and nipple without removal of nodes
|
#recall
|
|
|
Graham patch
|
plugging gastric or duodenal perforation with omentum, securing it with stitches
|
#recall
|
|
|
Heineke-Mickulicz pyloroplasty
|
Longitdinal incision through all layers of pylorus, then sewn closed perpendicular to incision → nonfunx pylorus (used after truncal vagotomy)
|
#recall
|
|
|
pringle maneuver
|
temproary occlusion of porta hepatis to help control liver blood flow when liver is bleeding
|
#recall
|
|
|
Modified radical mastectomy
|
removal of breast, nipple and axilary LN w/o mucle removal
|
#recall
|
|
|
Fem-pop bypass
|
femoral artery to popliteal artery bypasss using saphenous/synthetic graft. to bypass blockage in femoral artery
|
#recall
|
|
|
Hartmann's pouch
|
rectal stump after resection of colonic segment w/ colostomy
|
#recall
|
|
|
Truncal vagotomy
|
transection of vagus nerve trunks
NB: must provide drainage procedure for stomach because pylorus will not relax w/o vagus (pyroplasty) |
#recall
|
|
|
What reverses the deleterious effects of steroids on wound healing?
|
Vitamin A
|
#recall
|
|
|
Dakin Solutn
|
Dilute Sodium Hypochlorite (Bleach)
Used in contaimnated wounds |
#recall
|
|
|
Jackson-Pratt drain removal
|
1. Stitch removal
2. Sucxn discontinuation 3. Slow pull |
#recall
|
|
|
Penrose drain
|
open drainage via thin rubber hose.
increased infection rate v jackson-pratt grenade |
#recall
|
|
|
Incidence of Hernias
|
10% lifetime
50% indirect 25% direct 5% femoral |
#recall
|
|
|
Complete vs. Incomplete Hernias
|
Complete- sac and contents protrude all the way through
Incomplete- defect exists without complete protrusion |
#recall
|
|
|
En Masse Hernia Reduction
|
Reduction of hernia sac + contents together without contents exiting the sac
|
#recall
|
|
|
Littre's hernia
|
Hernia w/ Meckel's Diverticulum
|
#recall
|
|
|
Petersen's Hernia
|
Seen after Roux en Y bypass
small bowel through mesinteric defect of roux limb |
#recall
|
|
|
Lumbar hernia
|
Petit's or Grynfeltt's hernias
|
#recall
|
|
|
Petit's Triangle
|
Lat
External Oblique Iliac Crest |
#recall
|
|
|
Grynfeltt's Triangle
|
12th Rib
QL Internal Oblique |
#recall
|
|
|
Richter's hernia
|
incarceration of only one side of the bowel.
Strangulation → reduction → perforation w/o signs of obstrx |
#recall
|
|
|
Hesselbach's Hernia
|
Under inguinal ligament lateral to femoral vessels
|
#recall
|
|
|
Bochdalek's hernia
|
through posterior diaphragm
"Boch Da Lek" think Back on The Left |
#recall
|
|
|
Morgagni's Hernia
|
anterior parasternal diaphragmatic hernia
|
#recall
|
|
|
Properitoneal hernia
|
between peritonerum and transversalis fascia
|
#recall
|
|
|
Coopers hernia
|
through femoral canal and tracking to scrotrum or labium majus
|
#recall
|
|
|
Amyand's Hernia
|
Hernia contains ruptured appendix
|
#recall
|
|
|
DDx: mass in a healed C-section
|
hernia & endometrioma
|
#recall
|
|
|
Direct Inguinal Hernia Incidence
|
1% M>F
Increases with age |
#recall
|
|
|
Nerves in the inguinal canal
|
ilioinguinal nerve: runs with spermatic cord
--if you cut it → numbness of inner thigh & lateral scrotum, should go away in 6 mo prophylactic cutting removes risk of entrapement and ↓ post-op pain Genital Branch of the Genitofemoral Nerve: runs in spermatic cord. Motor to cremaster, sensory to anterior scrotum. |
#recall
|
|
|
Incidence of Indirect Hernia
|
5% M & W
|
#recall
|
|
|
What is in the spermatic cord?
|
Cremasteric Muscule Fibers
Vas Deferens Testicular Artery & Pampiniform Venous Plexus Genital branch of the genitofemoral nerve |
#recall
|
|
|
Cord Lipoma
|
Preperitoneal Fat on Cord Strx pushed in by hernial sack. remove surgically.
|
#recall
|
|
|
Boundaries of the Femoral Canal
|
Cooper's ligament
Inguinal Ligament Femoral Vein laterally Lacunar ligament medially. |
#recall
|
|
|
Howship-Rhomberg sign
|
pain along medial aspect of proximal thigh
indicative of nerve compression from obturator hernia. |
#recall
|
|
|
pain along medial aspect of proximal thigh
|
Howship-Rhomberg sign
indicative of nerve compression from obturator hernia. |
#recall
|
|
|
Corona Mortis
|
retropubic anastamosis between the epigastric artery and the obturator artery.
|
|
|
|
Inguinal Ligament is a thickening of the....
|
External Oblique Aponeurosis
|
|
|
|
Bogros Space
|
Extraperitoneal but Retroinguinal Space where mesh is placed
|
|
|
|
Where is mesh placed?
|
Bogros Space
Extraperitoneal but Retroinguinal |
|
|
|
Gimbernat's Ligament
|
Lacunar Ligament
a posteriorly oriented aponeurosis between the inguinal ligament and coopers ligament near the pubic symphsysis |
|
|
|
Reflected Inguinal Ligament
|
Inguina ligament fibers which continue medially to form contralateral aponeurosis
|
|
|
|
Iliopubic tract
|
Transversalis Fascia which inserts into inguinal ligament. Forms posterior wall of inguinal canal. The part seen when observing via laproscopy.
|
|
|
|
The Superficial Inguinal Ring is composed of...
|
External Oblique
Splits into medial and lateral crura |
|
|
|
Genitofemoral Nerve
|
L1-L2 from Lumbar Plexus
Descends along anterior surface of psoas Femoral Branch: Lateral Part of femoral triangle Genital Branch: anterior scrotum/labia majorum |
|
|
|
Innervation of the Scrotum
|
Fenital Branch of teh Genitofemoral Nerve: atnerior surface
Anterior scrotal nerves from teh ilioinguinal nerve posterior scrotal nerves from the perineal branch of the pudendal nerve Perineal branches of the psterior cutaneous nerve of the thigh |
|
|
|
Arterial supply of the Scrotum
|
Posterior scrotal branches of the perineal artery from the internal pudendal artery
anterior scrotal branches of the deep external pudendal artery from teh femoral artery cremasteric artery from the inferior epigastric artery |
|
|
|
Cremasteric Muscle is a continuation of the ...
innervated by the ... |
internal oblique
innervated by the genital branch of the genitofemoral nerve supplied by the cremasteric artery ariseing off the inferior pigastric artery |
|
|
|
Dartos fascia is a continuation of the ...
|
Scarpa's Fascia of the abdomen
Colle's fascia of the perineum |
|
|
|
Spermatic Cord
|
External spermatic fascia (external oblique)
Cermasteric fascia & Muscle (Internal oblique)--genital branch of the genitofemoral nerve Internal fascia: transveraslis abdominus |
|
|
|
Arterial Supply of the Ductus Deferens
|
Artery of the Ductus Deferens -- arises off the inferior epigastric artery
|
|