Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
59 Cards in this Set
- Front
- Back
|
Most commonly dislocated Joint
|
GlenoHumoral
|
|
|
Glenohumoral joint is dislocated due to lack
|
Bony stability
|
|
|
Shoulder is composed of
|
Glenoid, Humurus, scapula, acromium, and soft tissue
|
|
|
rotator cuff is composed of four muscles
|
(SITS) Supraspinatus, Infraspinatus, Teres minor, Subscapularis
|
|
|
Chronic Shoulder Pain
|
Look for frozen Shoulder, Tears in the rotator cuff
|
|
|
History of acute shoulder pain
|
The patient should be asked about shoulder pain, instability, stiffness, locking, catching and swelling.
|
|
|
frozen shoulder, dislocation or glenohumeral joint arthritis
|
can present as Stiffness or loss of motion
|
|
|
Pain with throwing
|
anterior glenohumeral instability
|
|
|
complain of generalized joint laxity
|
multidirectional glenohumeral instability
|
|
|
subtle signs of a cervical spine disorder
|
Neck pain and pain that radiates below the elbow
|
|
|
Pneumonia, cardiac ischemia and peptic ulcer disease, Gall Bladder, Heart attack
|
present with shoulder pain
|
|
|
DX: Serratus anterior or trapezius dysfunction
|
Sign: Scapular winging, trauma, recent viral illness
|
|
|
DX: Posterior shoulder dislocation
|
Sign: Seizure and inability to passively or actively rotate affected arm externally
|
|
|
Dx: Rotator cuff tear; suprascapular nerve entrapment
|
Sign: Supraspinatus/infraspinatus wasting
|
|
|
Dx: Cervical disc disease
|
Sign: Pain radiating below elbow; decreased cervical range of motion
|
|
|
Dx: joint pain and impingement Glenohumeral joint instability
|
Sign: Shoulder pain in throwing athletes; anterior glenohumeral joint pain and impingement
|
|
|
Dx: Labral disorder
|
Sign: Glenohumeral joint instability
Pain or "clunking" sound with overhead motion |
|
|
Dx: Impingement
|
Sign: Nighttime shoulder pain
|
|
|
Dx: Multidirectional instability
|
Sign: Generalized ligamentous laxity
|
|
|
evaluation of the painful shoulder, the neck and elbow should also be examined
|
pain can be referred to the shoulder from disease in these areas
|
|
|
Inspection
|
Pt. movement, Visual differences, swelling
|
|
|
Palpation
|
examination of the acromioclavicular and sternoclavicular joints, the cervical spine and the biceps tendon. The anterior glenohumeral joint, coracoid process, acromion and scapula should also be palpated for any tenderness and deformity.
|
|
|
Apley bra test
|
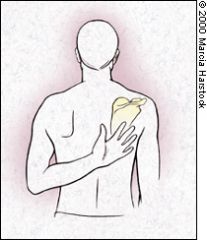
Adduction, internal rotation
|
|
|
Appley Scratch
|
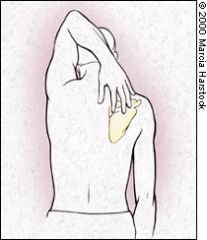
Testing abduction and external rotation.
|
|
|
Supraspinatus examination ("empty can" test)
|
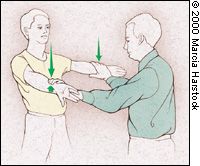
patient attempts to elevate the arms against resistance while the elbows are extended, the arms are abducted and the thumbs are pointing downward
|
|
|
Glenohumeral motion can be isolated
|
holding the patient's scapula with one hand while the patient abducts the arm
|
|
|
Infraspinatus/teres minor examination
|

The patient attempts to externally rotate the arms against resistance while the arms are at the sides and the elbows are flexed to 90 degrees
|
|
|
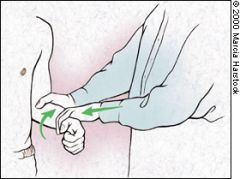
Subscapularis function is assessed with the lift-off test
|
The patient rests the dorsum of the hand on the back in the lumbar area. Inability to move the hand off the back by further internal rotation of the arm suggests injury to the subscapularis muscle
|
|
|
modified version of the lift-off test
|
hand of the affected arm on the abdomen and resists the examiner's attempts to externally rotate the arm.
|
|
|
Neer's test for impingement of the rotator cuff tendons under the coracoacromial arch
|

The arm is fully pronated and placed in forced flexion.
|
|
|
Dugas Test
|
Reach across the body anteriorly and touch the opposite shoulder. the elbow should be flat on chest. Negative means Subluxation or dislocation
|
|
|
Drop arm test
|
A possible rotator cuff tear. Arm is completely abducted and the slowly lowered to waist.
|
|
|
Spring Test
|
AC joint push down on the clavicle watch for excessive movement. Injured by falling with outstretched arms
|
|
|
Yergason test
|
biceps tendon instability or tendonitis. The patient's elbow is flexed to 90 degrees, and the examiner resists the patient's active attempts to supinate the arm and flex the elbow.
|
|
|
Dawburns sign
|
Subacromium Bursa
Deep Palp. over LI15 and TB14 pain lessened with arm bent and abducted 40 degrees |
|
|
Shoulder tests should be followed by
|
Cervical tests for referred radiculopathy
|
|
|
Proximal Clavicular fractures
|
-middle one third of the clavicle
-concomitant posterior dislocation of the sternoclavicular joint -A standard anteroposterior (AP) view radiograph |
|
|
Displaced distal clavicular fractures
|
result in disruption of the stabilizing ligaments of the acromioclavicular joint. Fractures of this type are more difficult to immobilize properly, and patients with this problem should generally be referred to an orthopedist for further evaluation
|
|
|
Humeral fractures
|
-direct blow or a fall onto an outstretched hand
- |
|
|
Scapular fractures
|
-result from a direct blow to the scapular area or from extremely high-force impact elsewhere to the thorax. The patient usually has tenderness at the fracture site, and arm abduction is painful. The neck and scapular body are most commonly involved.
- |
|
|
Glenohumoral Dislocation
|
-Most shoulder dislocations are anterior
-humeral head usually is palpable anteriorly, and the diagnosis is often confirmed by locating a dimple in the skin beneath the acromion -Shoulder dislocation is treated with relocation of the humerus -Return to mobilization in 7-10 days |
|
|
A sprain
|
is an injury to a ligament--a stretching or a tearing
|
|
|
strains
|
are usually the result of overuse--prolonged, repetitive movement of the muscles and tendons.
|
|
|
Acromioclavicular Joint Sprain and Separation
|
-well-localized swelling and tenderness over the AC joint
|
|
|
Sternoclavicular Joint Sprain and Separation
|
-SC joint injury will complain of pain, particularly with shoulder adduction. Localized tenderness and deformity
-posterior dislocation can be life-threatening because of compression of the trachea and great vessels of the neck -Radiographic 40-degree cephalic tilt view |
|
|
Rotator Cuff Tear
|
-common in persons older than 40 years
- |
|
|
Impingement Syndrome
|
m, the tendons of the rotator cuff can be impinged between the bony structures of the arch and the humerus. The impingement syndrome was described by Neer17,18 as a series of pathologic changes in the supraspinatus tendon:
stage I causes hemorrhage and edema; stage II, tendonitis and fibrosis; stage III, tendon degeneration of the rotator cuff and biceps, bony changes and tendon rupture. -Patients who present with impingement syndrome complain of pain over the anterolateral aspect of the shoulder that does not radiate below the elbow. |
|
|
frozen shoulder
|
Adhesive capsulitis results from thickening and contraction of the capsule and causes loss of range of motion and pain.
|
|
|
Biceps tendonitis
|
is initially managed with rest, ice, NSAIDs and corticosteroid injections and, when conservative management fails, tendon transfer.
|
|
|
Labral Injury
|
Common in throwing athletes
|
|
|
nerve impingement
|
referral numbness, tingling, dermatomal distribution
|
|
|
vessel compression
|
distal goes numb, reperfusion tingling,
|
|
|
trigger point
|
irritable spot in skeletal muscle trigerring a referred pain
|
|
|
Space occupying lesion SOL
|
-tumor bone fragment
-Valsava test- bearing down positive recreates pain |
|
|
Cervical compression test
|
-disk herniation
-IVF: intervertebral foramen |
|
|
Adson's test for TOS
|
is done to assess compression of the subclavian artery by the Anterior Scalene.
The test is performed as follows: 1)Monitor the patient's radial pulse at the wrist while you abduct, extend, and externally rotate the upper extremity at the shoulder joint (keeping the elbow straight) 2)Have the patient take a deep breath, rotate, and extend their head TOWARD the side being tested The test is positive if there is a marked decrease or absence of the radial pulse. |
|
|
TOS
|
Thoracic Outlet syndrome
|
|
|
Eden's Test
|
The examiner locates the radial pulse and draws the patient's shoulder down and back into extension with elbow extended, as the patient lifts their chest in an exaggerated "at attention or military" posture. A deep breath can be taken and held for 10 seconds. A positive test is indicated by an absence of a pulse. This test is particularly effective in patients who complain of symptoms while wearing a backpack or a heavy jacket.
|
|
|
Wright's Test (for pectoralis minor involvement)
|
-lymph
- Patient hyper-abducts arm above head to 180°, examiner palpates pulse and compares to uninvolved arm. |