Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
47 Cards in this Set
- Front
- Back
|
What are the age/location of specific soft tissue lesions - rhabdomyosarcoma, synovial sarcoma, liposarcoma
|
rhabdomyosarcoma - kids
synovial sarcoma - young adults liposarcoma and MFH - older adults location: 40% in lower extremity, especially thigh; deep worse than superficial |
|
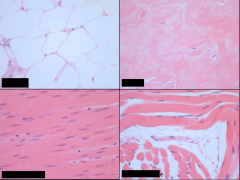
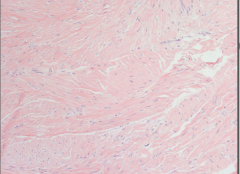
What tissue types are each of these?
|
Upper left - adipose
Upper right - fibrous Lower left - smooth muscle Lower right - skeletal muscle |
|
|
What are the grades of malignant (sarcomas) tumors?
|
Grade relates to prognosis
•Grade I, low, well-differentiated •Grade II, moderate, moderately differentiated •Grade III, high, poorly differentiated –Mitotic rate, necrosis especially important |
|
|
How is staging important in soft tissue tumors?
|
Staging is important in prognosis
–Size •<5 cm sarcoma: 30% of cases will have metastasis •>20 cm sarcoma: 80% of cases will have metastasis Overall 10yr survival rate for sarcoma: 40% |
|
|
Describe fibrous tumor-like proliferations
|
Reactive processes which are not aggressive
–Nodular fasciitis –Myositis ossificans •Locally aggressive – ‘fibromatoses’ –Superficial –Deep |
|
|
Describe nodular fasciitis
|
•Self-limited fibroblastic proliferation
•Presentation: –Adults; volar forearm, chest, back –Several weeks of solitary, rapidly growing, sometimes painful mass –Preceding trauma noted in 10-15% •Over time may spontaneously regress •Rarely recur after excision Gross: several cm in diameter, nodular, poorly defined margins •Histology: –very cellular with plump, immature fibroblasts (‘tissue-culture’ appearance) –Myxoid stroma –Often conspicuous nucleoli, mitoses presentW |
|
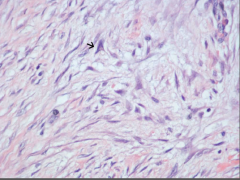
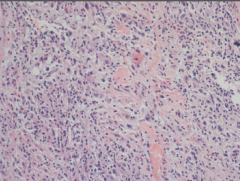
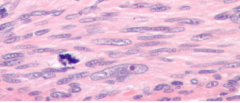
What is this?
|
Nodular fasciitis
Note triangle-shaped fibroblast |
|
|
Describe myositis ossificans
|
Post-traumatic bony metaplasia
•Presentation: –Athletic adolescents/young adults –Proximal muscles of extremities –Initially swollen/painful, evolves to painless, hard, well demarcated mass, bony on Xray •Simple excision is curative •Differential diagnosis: osteosarcoma |
|
|
Describe superfical and deep fibromatoses
|
Infiltrative fibroblastic proliferations
–May be locally aggressive –May recur after excision •Disfiguring, disturb function, +/- painful •Two clinicopathologic groups –1) superficial and 2) deep –Histologically similar Gross: 1-15 cm size, gray-white, firm, rubbery, poorly demarcated •Histology: cell of origin is myofibroblast –Plump cells, broad sweeping fascicles –Penetrate adjacent tissue –Infrequent mitoses –Early lesions cellular, later are less cellular with abundant collagen (esp. superficial ones) |
|
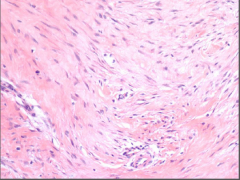
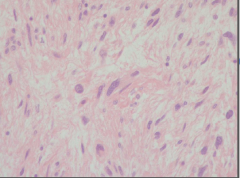
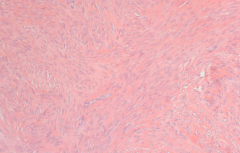
What is this?
|
Fibromatosis
|
|
|
What are the characteristics of SUPERFICIAL fibromatoses
|
- presentation: M> F, early presentation, deformation of hand (often b/l), foot penis
- eponyms: palmar fibromatosis = Dupuytren's contracture, penile = Peyronie's disease - may stabilize or resect +/- recurrence - may show trisomy 3 or trisomy 8 |
|

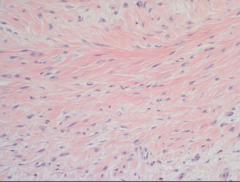
What is this?
|
Palmar fibromatosis - Dupuytren's contracture
|
|
|
Describe deep fibromatoses
|
Any age, but most frequent teens-30s
•Muscles of trunk or extremity –Shoulder, thigh, chest wall, back •Abdominal wall and abdominal cavity –In abdomen, often called “desmoid tumor” –Present with abdominal signs •(abd or flank pain, bowel obstruction, hydronephrosis, etc.) -APC gene (5q21-q22) mutation •Beta-catenin gene overexpression •Component of Gardner syndrome –Autosomal dominant –Germline mutation of APC gene –Fibromatoses, intestinal adenomas, osteomas |
|
|
Treatment of fibromatoses
|
Do not metastasize
•Treatment: –Some superficial ones may stabilize –Resection, but often recur, repeatedly –Some respond to tamoxifen –Others insensitive to chemo/radiation |
|
|
Describe fibrous/fibrohistiocytic tumors
|
Benign
–Fibroma –Benign fibrous histiocytoma (aka dermatofibroma) •Malignant –Fibrosarcoma –Malignant fibrous histiocytoma *‘histiocytic’ does not describe cell origin! |
|
|
Describe fibroma
|
Rare, most often a small ovarian mass
•Gross: well-demarcated, round, firm, white nodule •Histology: mature fibroblasts, copious collagen |
|
|
Describe fibrous histiocytoma
|
Common benign lesion
•Presentation: –Adults, dermis or subcutis, firm nodule, <1 cm •Histology: –Bland, mature fibroblasts with interlacing histiocyte-like cells •Cured by simple excision |
|
|
Describe fibrosarcoma
|
•Presentation:
–Adults –Deep tissue of thigh, knee, retroperitoneum –Slow growth, present years once diagnosed •>50% recur locally after excision •Metastasize hematogenously (lungs) Gross: –Soft, unencapsulated, infiltrative –Areas of hemorrhage and necrosis •Histology: varies, may be: –Bland, like a fibromatosis –Cellular, with herringbone pattern –Pleomorphic with many mitoses and necrosis |
|
|
What is the histology of fibrosarcoma?
|
HERRINGBONE PATTERN
|
|
What is this?
|
Fibrosarcoma
|
|
|
Describe malignant fibrous histiocytoma
|
Historically represented variety of sarcomas
•Histology: –Pleomorphic, bizarre giant cells –Storiform (swirling) architecture –Necrosis, hemorrhage, many mitoses •Very aggressive behavior •Currently MFH is a diagnosis of exclusion –aka pleomorphic sarcoma, NOS •Immunohistochemistry: –Doesn’t stain for: •S-100 (lipo) •Desmin (rhabdo, leio) •Smooth muscle actin (leio) •Myogenin or myoD1 (rhabdo) •Cytokeratin or EMA (synovial sarcoma) |
|
What is this?
|
Malignant fibrous histiocytoma
|
|
What is this?
|
Malignant fibrous histiocytoma
|
|
|
Describe tumors of fat
|
Benign: Lipoma
•Malignant: Liposarcoma •Immunohistochemistry: –Usually positive for S-100 |
|
|
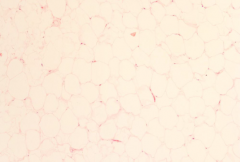
Describe lipoma
|
Most common soft tissue tumor of adults
•Presentation: –Adults, usually solitary, slowly enlarging, mobile, painless mass •Complete excision usually curative Gross: soft, yellow, encapsulated •Histology: mature adipocytes •May be subclassified by: –Other histologic features: conventional, myolipoma, spindle cell, myelolipoma, angiolipoma, pleomorphic –characteristic chromosomal rearrangements (don’t worry about these) |
|

What is this?
|
Lipoma
|
|
|
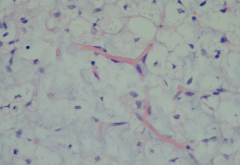
Describe liposarcoma
|
Presentation:
–Adult, 5th and 6th decades, mass or functional changes, in deep soft tissues or viscera •Gross: –Fatty, may be tan-white, have hemorrhage or necrosis •Histology: –Varies, type is prognostically important –Diagnostic cell is the lipoblast |
|
|
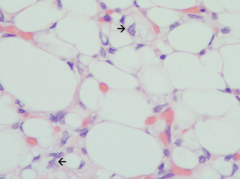
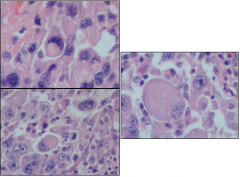
What is this? What is at the arrow?
|
Liposarcoma
Lipoblast with scalloped nucleus |
|
What is this?
|
Liposarcoma
Lipoblast with scalloped nucleus |
|
|
Histology of liposarcoma
|
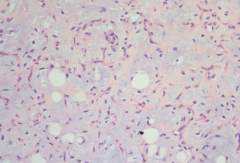
Well-differentiated:
–Mature adipocytes with some lipoblasts •Myxoid: –As above, but with a bluish, mucoid matrix, and chicken-wire vascular pattern •Round cell: –Lipoblasts present, but majority are small, round cells •Pleomorphic: –Significant pleomorphism Well-differentiated and myxoid: indolent •Round cell and pleomorphic: aggressive, recur after excision, metastasize to lungs |
|
What is this?
|
Well-differentiated liposarcoma
|
|
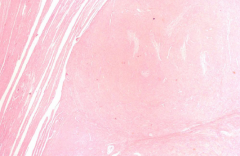
What is this?
|
Myxoid liposarcoma
|
|
What is this?
|
Myxoid liposarcoma, high power
|
|
|
Mutations in liposarcoma
|
Well-differentiated: amp 12q
–Increased transcription of MDM2 gene –Product binds, inactivates p53 (tumor suppressor) •All myxoid (and some round cell): t(12;16) –CHOP gene (adipocyte differentiation) on 12q13 –FUS gene (transcription factor) on 16p |
|
|
Describe smooth muscle tumors
|
Benign: leiomyoma
•Malignant: leiomyosarcoma •Immunohistochemistry: –Usually positive for vimentin, desmin, smooth muscle actin (SMA) |
|
|
Describe leiomyoma
|
Most common presentation: uterine “fibroids”
–Adult female with pelvic fullness, discomfort –Pregnancy and delivery complications •Gross: –Very well-circumscribed masses –Tan-to-white whorled cut surfaces •Histology: –Bands of smooth muscle cells with no mitotic activity |
|

What is this?
|
Leiomyoma
|
|
What is this?
|
Leomyoma
|
|
What is this?
|
Leiomyoma
|
|
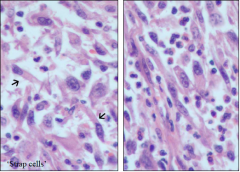
What is this?
|
Leiomyosarcoma
Presentation: –Adults, female>male –Skin: firm painless masses –Deep tissue of extremities: mass, impaired function –Retroperitoneum: abdominal symptoms •Histology: –spindle cells with cigar-shaped nuclei, +mitoses –interweaving fascicles Treatment: excision or radiation, or both •Prognosis: –Cutaneous/superficial: small, easy to treat –Retroperitoneal: large, difficult to excise, death by local extension and metastasesD |
|
|
Describe skeletal muscle tumors
|
Benign: rare: rhabdomyoma
•Malignant: rhabdomyosarcoma •Immunohistochemistry: –Usually positive for vimentin, desmin, myogenin, MyoD1 |
|
|
Describe rhabdomyosarcoma
|
Kids and adolescents
–Most common soft tissue neoplasm –Head/neck or genitourinary tract •Gross: depends on location –Hollow organs of GU: may be gelatinous, grape-like (sarcoma botryoides) –In solid tissue: infiltrating mass Histology: diagnostic cell: rhabdomyoblast –Rich in thick and thin filaments –May be elongated (tadpole cell or strap cell, cross striations may be visible) or round –If very poorly differentiated, may look like small round blue cell, so immunohistochemistry needed •Histology: pattern variants are prognostic –Embryonic, pleomorphic, alveolar –(better --> mid --> worse prognosis) Most cases have t(2;13) –Chromosome 2: PAX3 gene, upstream of skeletal muscle differentiation gene –Chromosome 13: FKHR gene –Chimeric protein likely disregulates skeletal muscle differentiation |
|
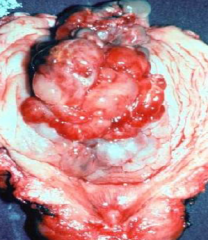
What is this?
|
Sarcoma botryoides - rhabdomyosarcoma in hollow organ
Most cases have t(2;13) –Chromosome 2: PAX3 gene, upstream of skeletal muscle differentiation gene –Chromosome 13: FKHR gene –Chimeric protein likely disregulates skeletal muscle differentiation |
|
What tumor is this?
|
Rhabdomyosarcoma
•Histology: pattern variants are prognostic –Embryonic, pleomorphic, alveolar –(better --> mid --> worse prognosis) Most cases have t(2;13) –Chromosome 2: PAX3 gene, upstream of skeletal muscle differentiation gene –Chromosome 13: FKHR gene –Chimeric protein likely disregulates skeletal muscle differentiation |
|
What is this?
|
Rhabdomyosarcoma
•Histology: pattern variants are prognostic –Embryonic, pleomorphic, alveolar –(better mid worse prognosis) Most cases have t(2;13) –Chromosome 2: PAX3 gene, upstream of skeletal muscle differentiation gene –Chromosome 13: FKHR gene –Chimeric protein likely disregulates skeletal muscle differentiation |
|
|
Describe synovial sarcoma
|
Not comprised of synovial cells
•Presentation: –Young adults; 20-40 y.o. –Deep soft tissue around joints of extremities •60-70% around knee Histology: –Biphasic; spindle cells and epithelial-like cells –Monophasic: entirely spindle cells •May require immunohistochemistry •Send for genetic studies! •Immunohistochemistry: –Both epithelial, spindle cells + for cytokeratin •Most are t(X;18) • fusion product SSX/SYT –Combines SYT gene (transcription factor) with SSX1 or SSX2 gene (transcription inhibitors) •Specific translocation relates to prognosis –SSX1 involvement yields poorer prognosis Treatment is aggressive –Limb-sparing surgery –Chemotherapy •Metastasizes to lung, bone, lymph nodes •Survival: –5 year: 25-62% –10 year: 10-30% |
|
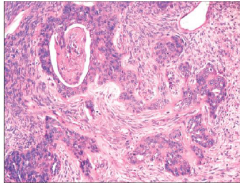
What is this?
|
Synovial sarcoma
|