![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
115 Cards in this Set
- Front
- Back
|
Family hx for acute coronary syndrome |
female relatives <65 male relatives <55 |
|
|
Risk factors for Ischemic heart dz |
1) DM (most important) --> equivalent to having CAD for lipid management 2) HTN (most common) 3) Tobacco use 4) Hyperlipidemia 5) Peripheral arterial dz 6) obesity 7) inactivity 8) fam hx |
|
|
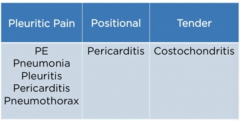
CAD chest pain alternatives |
does NOT change with body position does NOT change with respiration does NOT change with tenderness response to nitrates does NOT always mean CAD |
|
|
Chest pain not CAD |
|
|
|
Potential physical findings for MI |
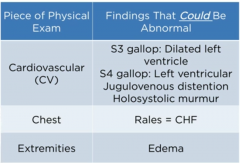
S3 --> volume overload so should add diuretics |
|
|
Mechanism of S3 gallop |
rapid ventricular filling during diastole as soon as mitral valve opens, blood rushes into ventricle causes splash sound transmitted as S3 |
|
|
Mechanism of S4 gallop |
sound of atrial systole into a stiff or non-compliant left ventricle occurs just before S1 occurs with any type of left ventricular hypertrophy S4 is bang of atrial systole |
|
|
EKG changes & tx |
ST elevation --> thrombolytics within 30 mins of presenting or 12 hrs of onset of pain or angioplasty within 90 minutes of getting in the door (prefer angioplasty, if not possible, then thrombolytics) ST depression --> LMWheparin Chest pain + new LBBB --> thrombolytics within 12 hrs |
|
|
Most accurate test for MI |
CK-MB or troponin start to rise 3-6 hours after onset of pain within 4 hrs, only thing that is elevated is myoglobin for re-infarction --> CK-MB (stays elevated for 1-2 days whereas troponin is elevated for 1-2 weeks) |
|
|
Troponin components |
Troponin C --> binds Ca to activate actin:myosin interaction (C for Ca) Troponin T --> binds to tropomyosin (T for tropomyosin) Troponin I --> blocks or inhibits actin:myosin interaction (I for inhibition) |
|
|
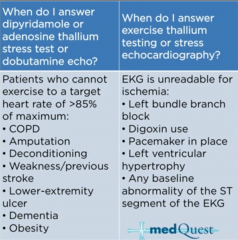
Stress test vs ECHO |
|
|
|
Most accurate test to detect EF |
nuclear ventriculogram (MUGA scan) |
|
|
Mechanism of nuclear testing |
nuclear isotopes are picked up by Na/K ATPase of normal myocardium to myocardium, thallium looks like K if cardiac tissue is alive and perfused, then it will be picked up with nuclear isotope decreased uptake = damage |
|
|
Anticoagulation for ACS |
aspirin + either prasugrel or clopidogrel or ticagrelor |
|
|
Mechanism of P2Y12 antagonists |
clopidogrel, prasugrel, & ticagrelor block aggregation of plt to each other by inhibiting ADP-induced activation of P2Y12 receptor clopidogrel and prasugrel are thienopyridine class prasugrel is contraindicated in pts with stroke, >80yo, other bleeding d/o everyone getting an angioplasty and/or stent receives a P2Y12 antagonist |
|
|
Contraindications for thrombolytics |
1) severe HTN (>180/>110) 2) surg within last 2 weeks 3) hx of hemorragic stroke |
|
|
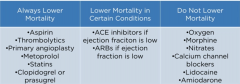
Tx for ACS |
All reduce mortality
beta-blockers (eg metoprolol)
ACEI (eg lisinopril) --> lower mortality in systolic dysfunction (not clear in inferior wall MI)
statins
Aspirin
Clopidogrel |
|
|
Tx for ACS & effect on mortality reduction |
|
|
|
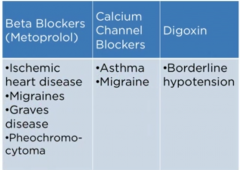
When to use CCB... |
intolerance to beta-blockers severe reactive airway dz (asthma) cocaine-induced chest pain coronary vasospasm/prinzmetal angina |
|
|
Pacemaker placement after acute MI |
3rd degree AV block (rt coronary artery block bc it supplies AV node) mobitz II 2nd degree AV block bifascicular block NEW LBBB symptomatic bradycardia |
|
|
Lidocaine or amiodarone for acute MI |
ONLY with v-tach or v-fib |
|
|
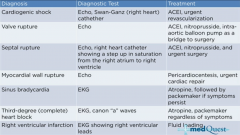
Complications of MI |
|
|
|
GPIIa/IIIa inhibitor use |
eg abciximab for ACS with angioplasty and stent NO benefit for STEMI |
|
|
Indications for CABG |
3 vessel with >70% stenosis LT main artery >70% stenosis 2 vessel dz in a diabetic |
|
|
Coronary artery disease equivalents |
1) DM 2) peripheral artery dz 3) aortic dz 4) carotid dz 5) anyone with stroke give statins to all these ppl |
|
|
RF in lipid management |
1) tobacco use 2) high BP (>140/90) 3) on BP meds 4) low HDL chol (<40) 5) fam hx (females <65 & males <55) 6) age of patient (males >45 & females >55) give statins with (& goal is LDL <100): 1 risk --> LDL >190 2 risks --> LDL >160 CAD equivalent --> LDL >130 CAD & DM --> goal is LDL <70 |
|
|
Carvedilol |
beta-1, beta-2, & alpha-1 receptor antagonist anti-arrhythmic, -ischemic, -hypertensive |
|
|
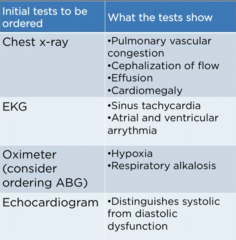
Initial testing for CHF |
|
|
|
Phosphodiesterase inhibitors |
imamrinone & milrinone (similar to dobutamine) only used in acute pulm edema increase contractility decrease afterload (like vasodilators) dopamine also increases contractility but bc of alpha-1 agonist properties --> vasoconstriction so increases afterload |
|
|
Respiratory alkalosis |
fluid overload --> hypoxia --> hyperventilation --> dec pCO2 --> alkalosis hypoxia leads to resp alkalosis |
|
|
Acute management of pulmonary edema |
Furosemide --> preload reduction Oxygen Nitrates Morphine if pt doesnt improve, add positive inotrope (eg dobutamine, imamrinone, milrinone) |
|
|
Indications for synchronized cardioversion |
Chest pain, shortness of breath, hypotension, confusion means you're not getting enough perfusion can do synchronized cardiversion with v tach, v fib, a fib |
|
|
V tach & stable |
give lidocaine or amiodarone or procainamide |
|
|
Chronic management of CHF |
ECHO to distinguish btwn systolic vs diastolic dysfunction systolic failure that lowers mortality: ACEI b-blocker (metoprolol or carvedilol) spirolactone or eplerenone (aldosterone inhibitor) diuretics digoxin (not for acute setting) diastolic failure (no drugs actually lower mortality): b-blockers diuretics always wrong for diastolic failure --> digoxin or spirolactone can also give implantable cardioverter/defibrillator |
|
|
Biventricular defibrillator & CHF |
severe CHF AND wide QRS (>120 msec) |
|
|
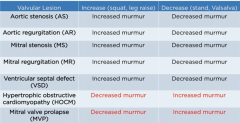
Valsalva maneuver |
exhalation against closed glottis thoracic pressure increases which leads to decrease in venous return if improves, then can tx with diuretics |
|
|
Standing vs squatting position |
when you stand, the leg veins open which leads to increased blood flow to legs & thereby decreasing venous return to heart squatting has opposite effect bc it closes the veins in the legs thereby increasing venous return to heart |
|
|
Valvular heart disease |
ALL p/w SOB & normally worse with exertion or exercise ALL will have 1) murmur & 2) rales on lung exam Can also possibly have peripheral edema, carotid pulse findings, or gallops |
|
|
Valvular heart disease RFs |
HTN MI/ischemia Rheumatic fever --> most common is MV stenosis but can affect any valve Young pts --> MV prolapse, HOCM, MV stenosis, Bicuspid AV |
|
|
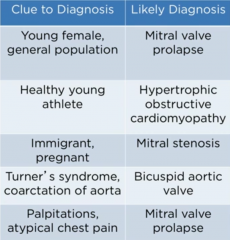
Clues to valvular dz dx |
|
|
|
Murmurs |
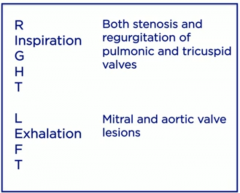
Systolic murmurs: aortic stenosis (AS) --> goes to carotid mitral regurg (MR) --> goes to axilla Diastolic murmurs: aortic regurg (AR) --> diastolic decrescendo on lt lower sternal border mitral stenosis (MS) Right sided murmurs increase with inhalation --> increase venous return Left sided murmurs increase with exhalation |
|
|
Left vs Right murmurs |
|
|
|
Summary of valvular lesion and preload maneuvers |
|
|
|
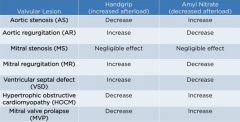
Handgrip & effect on cardiac blood flow |
compresses arteries of arm leading to increased afterload opposite effect of ACEI Regurg lesions worsen with handgrip hence you treat them with ACEI handgrip improves murmur of MVP, HOCM, & AS hence you do not want to treat these with ACEI |
|
|
Amyl Nitrate & effect on cardiac blood flow |
vasodilator & dilates peripheral arteries so decreases afterload similar to giving ACEI improves murmur for AR/MR hence you tx with ACEI worsens murmur for MVP, HOCM, & AS hence never tx these with ACEI decreases pressure in aorta thus increasing gradient btwn LV & aorta making AS worse |
|
|
Summary of valvular lesion and afterload maneuvers |
|
|
|
Location and radiation of murmurs |
Aortic stenosis 2nd RIGHT intercostal space radiates to carotid crescendo-decresendo
Pulmonic valve murmurs 2nd LEFT intercostal space
Aortic regurg (& VSD) lower LEFT sternal border
Mitral regurg apex & radiates to axilla |
|
|
Valvular heart dz testing |
best initial test: ECHO most accurate test: left heart catheterization |
|
|
Valvular heart dz tx |
Regurg lesions --> vasodilators (eg ACEI, ARBs, nifedipine) Stenotic lesions --> anatomic repair MS is balloon valvuloplasty even/esp in preg pt AS is surgical repair |
|
|
Aortic stenosis presenting Sxs |
most common is chest pain 50-80% of AS are assoc with CAD syncope & CHF are less common pt also tends to be older |
|
|
Aortic stenosis prognosis |
with: CAD --> 3-5 yr avg survival syncope --> 2-3 yr avg survival CHF --> 1.5-2 yr avg survival |
|
|
Testing for aortic stenosis |
best initial test is transthoracic ECHO (TTE) transesophageal ECHO (TEE) is more accurate MOST ACCURATE is left heart catheterization bc it gets pressure gradient |
|
|
Aortic valve gradient |
pressure difference btwn left ventricle & aorta normal gradient - <30mm Hg moderate disease - 30-70mm Hg severe disease - >70mm Hg |
|
|
Valve replacement for AS |
bioprosthetic valves (porcine or bovine) last 10 yrs --> DO NOT require anti-coagulation Mechanical valves must be treated with warfarin Balloon dilation of AS ONLY if pt is too sick to undergo surgery |
|
|
Causes of aortic regurg |
HTN rheumatic heart dz endocarditis cystic medial necrosis SOB & fatigue are most common presentations |
|
|
Aortic regurg physical findings |
quincke pulse: arterial or capillary pulsations in fingernails water-hammer pulse (Corrigan's pulse): high bounding pulses Musset's sign: head bobbing with each pulse Duroziez's sign: murmur heard over femoral artery Hill sign: BP gradient much higher in lower extremities diastolic decrescendo murmur |
|
|
Aortic regurg testing |
TTE initial test TEE more accurate left heart cath most accurate |
|
|
Aortic regurg tx |
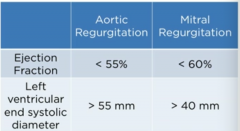
ACEI, ARBs, or nifedipine can add loop diuretic (furosemide) surgery if EF <55% (even ASx) OR LV end systolic diameter >55mm |
|
|
Mitral stenosis & pregnancy |
MS can manifest in preg pt for first time bc of increased plasma volume |
|
|
Unique findings for mitral stenosis |
in addition to SOB like other valve issues, can also see: dysphagia - large left atrium presses on esophagus hoarseness - pressure on recurren laryngeal nerve a-fib --> strokes |
|
|
Murmur of mitral stenosis |
diastolic rumble with opening snap (extra sound in diastole) S3 loud opening snap occurs earlier as dz progresses |
|
|
Causes of mitral regurg |
HTN ischemic heart dz anything that dilates heart |
|
|
Murmur of mitral regurg |
holosystolic heard best at apex & radiates to axilla increases with leg raising, squatting, handgrip decreases with standing, valsalva, amly nitrate |
|
|
Reasons for surgery in regurg |
|
|
|
Ventricular septal defects |
holosystolic murmur at lower left sternal border (can be described as machinic murmur) can lead to SOB if large enough murmur worsens with exhalation, squatting, or leg raise |
|
|
Atrial septal defects |
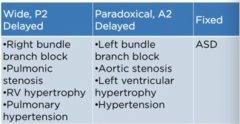
fixed splitting of S2 can tx with percutaneous or catheter devices repair indicated when shunt ratio >1-1.5 |
|
|
Causes of splitting of S2 |
|
|
|
Causes of dilated cardiomyopathy |
ETOH adriamycin radiation chagas' dz dilated cardiomyopathy = decreased EF = systolic failure |
|
|
Tx of dilated cardiomyopathy |
Increase survival: ACEI/ARBs b-blocker spironolactone digoxin decreases sxs but does NOT prolong survival |
|
|
Hypertrophic cardiomyopathy |
SOB on exertion S4 gallop hypertrophic cardiomyopathy = normal EF = diastolic dysfunction |
|
|
Tx of hypertrophic cardiomyopathy |
Nothing improves survival but tx with:
b-blocker diuretics digoxin & spironolactone DO NOT show any benefit |
|
|
S4 sound |
S4 = decreased compliance S4 gallop = LV hypertrophy S4 DOES NOT mean u have to add additional tx |
|
|
Causes of restrictive cardiomyopathy |
sarcoidosis amyloidosis hemochromatosis cancer myocardial fibrosis glycogen storage dz |
|
|
Sx of restrictive cardiomyopathy |
SOB Kussmaul sign --> inhalation causes increase in jugular venous pressure instead of normally decreases (also seen in constrictive pericardititis) |
|
|
Testing for restrictive cardiomyopathy |
EKG - low voltage ECHO endomyocardial bx - most accurate diagnostic test of the etiology |
|
|
Pericarditis |
Chest pain that is: pleuritic positional (better when leaning fwd & worse when leaning back) sharp & brief friction rub (but only in 30%) vast majority are secondary to viruses can also be due to collagen-vascular dz (eg lupus) or trauma |
|
|
Testing for pericarditis |
EKG - ST elevation and PR depression in all leads |
|
|
Tx of pericarditis |
NSAIDs (naproxen, aspirin, or ibuprofen) if pain persists after 2 days, add prednisone orally colchicine decreases freq of reoccurrences |
|
|
Pericardial tamponade |
can be complication of pericarditis left & right atriums are affected first right heart cath will show equalization of all pressures in the heart during diastole & wedge pressure will be same as right atrial and pulm artery diastolic pressure |
|
|
Sxs of pericardial tamponade |
SOB hypotension JVD clear lungs (SOB + hypotension + JVD + lung sounds = pulm edema) pulsus paradoxus - decrease in BP during inhalation >10mm Hg can cause the pulse go away electrical alternans - change in height of QRS |
|
|
Tx of pericardial tamponade |
best initial tx - pericardiocentesis long term - pericardial window placement NEVER GIVE DIURETICS |
|
|
Constrictive pericarditis |
pericardium is overly tight p/w SOB & signs of right heart failure (edema, JVD, HSM, ascites) unique features kussmaul sign pericardial knock (extra sound in diastole from heart hitting calcified thickenedpericardium) |
|
|
Testing for constrictive pericarditis |
CXR - shows calcification EKG - low voltage CT and MRI - thickening of pericardium |
|
|
Tx for constrictive pericarditis |
diuretic surgical removal of pericardium |
|
|
Aortic dissection |
chest pain radiating to back btwn scapula described as very severe & ripping BP can be different btwn arms best initial test - CXR showing widened mediastinum most accurate test - CT-A, MR-A,TEE |
|
|
Tx of aortic dissection |
b-blocker with first screen in addition to EKG & CXR after b-blocker, use nitroprusside to control BP |
|
|
Abdominal Aortic Aneurysm |
screening with u/s (smoking men 65-75) repair if >5cm with endovascular repair smaller ones just need to be monitored |
|
|
Law of LaPlace |
wall tension = radius x pressure wider aorta = widens faster need to decrease BP and/or repair |
|
|
Peripheral arterial dz |
claudication (pain in extremities on exertion) can get smooth and shiny skin loss of hair and sweat glands loss of pulses in the feet |
|
|
Testing for PAD |
best initial test - Ankle-brachial index (ABI) normal ABI >0.9 (pressure is > in ankle than brachial when standing) >10% difference = obstruction most accurate test - angiography |
|
|
Tx for PAD |
best initial tx - aspirin need to have BP control with ACEI LDL <100 control DM unique drug is cilostazol marginally effective is pentoxifylline DO NOT GIVE CCB exercise as tolerated |
|
|
PAD vs spinal stenosis |
spinal stenosis - worse walking DOWNhill PAD - worse walking UPhill, cycling, or sitting pulses & skin exam are also normal with spinal stenosis |
|
|
Acute arterial embolus |
very sudden loss of pulse cold extremity very painful usually assoc with valvular dz or a-fib tx with heparin |
|
|
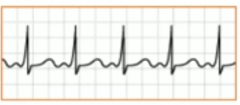
Atrial fibrillation |
palpitations irregular pulse HTN is most common cause of a-fib can also be caused by ischemia or cardiomyopathy |
|
|
A-fib EKG |

|
|
|
Tx of A-fib |
Unstable patient (chest pain, SOB, hypotension, confusion) next step in management is synchronized cardioversion stable patient: if HR >100-110 lower with b-blocker, CCB (only diltiazem or verapamil), or digoxin once rate controlled, anti-coagulate with warfarin, dabigatran, or rivaroxaban if a-fib present for >2 days |
|
|
CHADS score |
Chf Htn Age >65 Dm Stroke/TIA (worth 2 points)
0 or 1 = aspirin 2+ = warfarin, dabigatran, or rivaroxaban |
|
|
Atrial flutter |

similar to a-fib with only difference being rhythm is regular at presentation |
|
|
Tx of a-flutter or a-fib |
|
|
|
Multifocal Atrial Tachycardia |
atrial arrhythmia assoc with COPD/emphysema avoid b-blocker EKG - polymorphic P waves with different atrial foci |
|
|
Supraventricular tachycardia |
palpitations and tachycardia NOT assoc with ischemia regular rhythm with ventricular rate of 160-180 |
|
|
Tx of supraventricular tachycardia |
unstable patients --> synchronized cardioversion stable patients --> vagal maneuvers (carotid sinus massage, ice immersion of the face, Valsalva) if vagal maneuvers dont work --> IV adenosine long term management - radiofreq catheter ablation |
|
|
Wolff-Parkinson-White syndrome |
WPW presents as SVT that can alternate with ventricular tachycardia caused by abnormal piece of neuralized cardiac muscle going around AV node conduction in aberrant tract is faster so PR interval shortens (<120msec) and is delta wave on EKG CCB & digoxin force conduction through aberrant tract so are contraindicated in tx of WPW can result in either atrial or ventricular arrhythmia |
|
|
WPW EKG |
short PR causes delta wave |
|
|
Tx of WPW |
if pt is in SVT or VT from WPW --> procainamide long-term therapy - radiofreq catheter ablation |
|
|
Ventricular tachycardia |
can p/w palpitation, snycope, chest pain, or sudden death for stable pt amiodarone lidocaine procainamide Mg for unstable pt synchronized cardioversion |
|
|
Ventricular fibrillation |
presents with sudden death tx with unsynchronized cardioversion |
|
|
Steps in management for V-fib |
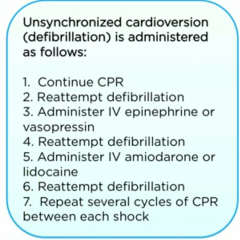
first is unsynchronized cardioversion then... |
|
|
3 questions of syncope evaluation |
1) loss of consciousness sudden or gradual? sudden --> cardiac or seizures gradual --> metabolic/hypogly, toxicity, anemia, hypoxia 2) regaining of consciousness sudden or gradual? sudden --> cardiac gradual --> seizure 3) Cardiac exam normal --> ventricular arrhythmia abnormal --> structural heart dz CANNOT HAVE SYNCOPE FROM CAROTIDS SO DO NOT DO CAROTID DOPPLER |
|
|
Tx post-MI |
all pts should get: 1) b-blocker 2) ACEI 3) Aspirin 4) clopidogrel 5) high-intensity statin (eg rosuvastatin) REGARDLESS of baseline LDL |
|
|
Causes of prolonged QT |
1) congenital 2) hypomagnesium 3) hypokalemia 4) drugs (eg fluoroquinolones & antipsychotics) predisposes to torsade de pointes |
|
|
Indications for ICD implantation |
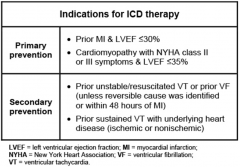
automated implantable cardioverter-defibrilliator |
|
|
Treating MR |
tx with surgery when: 1) MR with sxs (eg exercise intolerance, dyspnea, fatigue) 2) Asx with LV hypertrophy, pulm HTN, or new onset a-fib if none of the above, manage by close monitoring & biannual ECHO |
|
|
Sick sinus syndrome |
aka bradycardia-tachycardia syndrome usually alternates btwn SVT & bradycardia caused by chronic SA node dysfunction usually occurs in elderly with multiple co-morbidities & p/w lightheadedness or presyncope a-fib is most common type of tachy in this condition tx with pacemaker to control bradycardia & use meds to control rate for tachy |
|
|
Dabigatran |
direct thrombin inhibitor a-fib with CHADS-65 of 2+ --> can be used in NON-VALVULAR dz |