Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
83 Cards in this Set
- Front
- Back
|
What identifies a tumor of the bronchus as SCC?
|
keratin formation and lack of gland formation.
|
|
|
What brown pigment can surround neuronal tissue?
|
keratin
|
|
|
In a _______, it has been shown the stromal cells are the neoplastic(monoclonal) cells while the surrounding epithelial cells are secondary(non-neoplastic).
|
fibroadenoma(breast)
|
|
|
What are some ectodermally derived structures?
|
Hair, sebacious glands, epidermis
|
|
|
Name some endodermally derived tissue. Mesodermally derived?
|
respiratory type mucosa with ciliated epithelium and small mucous glands.
Mesodermal - cartilage and fat |
|
|
Differentiate between lymphoma and carcinoma in the lymph.
|
Carcinomas fill subcapsular sinus while lymphomas generally replace entire node.
|
|
|
This can indicate adenocarcinoma.
|
cytoplasmic mucin vacuoles.
|
|
|
Numerous white tan tumors present on liver? Primary or metastatic?
|
Metastatic. If primary it would have just been one or few nodes.
|
|
|
What is notable about pancreatic cancer?
|
Bone metastasis often cause osteoblastic changes as opposed to osteolytic.
|
|
|
How would a patient with lung carcinoma metastatic to bone present?
|
bone pain
|
|
|
If I have an metastatic adenocarcinoma in the liver, where is a possible point of origin for primary tumor?
|
Pancreas. It could have travelled through portal venous system.
|
|
|
What is/causes pseudomyxoma peritonei?
|
It is when the peritoneal cavity fills with mucin/tumor. Can be caused by mucinous colon carcinoma. Sometimes referred to as "jelly belly"
|
|
|
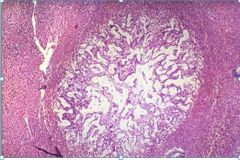
How would a benign thyroid follicular adenoma present?
|
rapid enlargement of thyroid
|
|
|
Describe thyroid adenomas
|
well formed, uniformly regular shaped, cuboidal follicular epithelial cells with normal polarity.
|
|
|
Describe reasons to favor a benign adenomatous polyp vs a carcinoma.
|
size(> 2cm), lack of invasion
abnormal architectural structures would indicate carcinoma |
|
|
Describe a likely characteristic of colon villous adenoma
|
inability to produce mucin
|
|
|
well differentiated adenocarcinoma retaining ability to make glands
|
|
|
How would a carcinoma presenting in the head of the pancreas obstructing the bile duct present?
|
painless jaundice
|
|
|
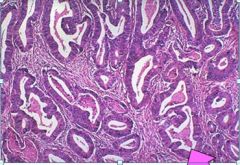
Adenocarcinoma of pancreas. Note few but present gland formation identifying adenocarcinoma. Also, vascular invasion is shown.
|
|
|
perineural invasion by adenocarcinoma cells
|
|

|
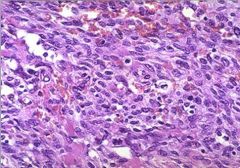
This malignant tumor may be an adenocarcinoma arising from the columnar epithelial lining of the bronchus or a squamous cell carcinoma arising from squamous metaplasia.
|
|

differentiate adenocarcinoma, SCC and neuroendocrine small cell carcinoma.
|
Differential diagnosis includes adenocarcinoma, squamous cell carcinoma and neuroendocrine small cell carcinoma (oat cell carcinoma). The latter two are typically central (as in this case). Adenocarcinoma is usually peripheral (scar cancer).
|
|
|
Squamous cell carcinoma (SCCA) of bronchus. Haphazard cords of infiltrating cells. Keratin formation but no glands identify this as SCCA.
|
|
|
Intercellular bridges, which indicate desmosomes are a feature of?
|
SCCA
|
|
|
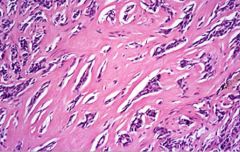
leiomyoma
|
|
|
leomyosarcoma
|
|
|
osteoid produced by osteosarcoma
|
|
|
Patients with FAP have a mutation in what gene?
|
APC
|
|
|
Patients with NF-1 have a mutation in what gene?
|
neurofibromin.
RAS and GTPase activity that downreglates RAS |
|
|
What determines homing of cancer cells to organs?
|
Anatomic considerations(drainage...lymph/vascularization)
Tumor cells may have receptors for endothelial cells on certain organs Certain tissues may not favor metastases because the microenvironment may inhibit proteolytic enzymes needed for invasion by tumor cells |
|
|
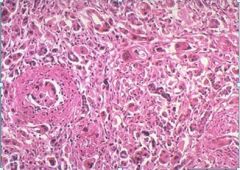
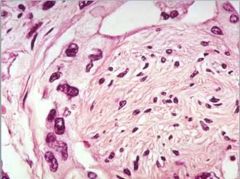
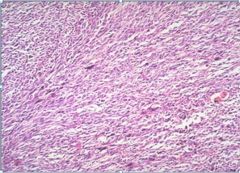
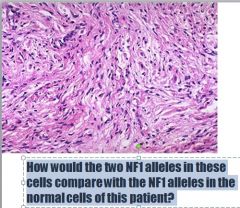
Neurofibroma, spindle cells with features of Schwann cells and fibroblasts in wavy bundles, uniform in shape and size. Nuclei are elongated, curved. There is little pleomorphism or mitotic activity.
|
|
|
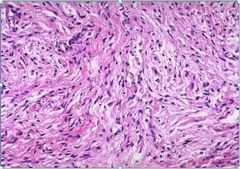
Neurofibrosarcoma. Compared to neurofibroma, it is more hyperchromatic with larger nuclei, more variation in shape, size, higher N:C ratio. Mitoses are present.
|
|
|
What route of metastasis is commonly used by sarcomas?
|
Sarcomas spread by invading blood vessels.
|
|
|
What factors induce vascularization (angiogenesis) of tumor?
|
Two important ones are basic fibroblast growth factor (bFGF) and vascular endothelial growth factor (VEGF) produced by tumor cells or by host cells like macrophages that accumulate in tumors).
|
|
|
How frequently are mutations in TP53, RAS, and APC seen in other types of malignancies?
|
p53 is most common gene mutated in human cancer, mutated in > 50% of all malignancies.
RAS is most common mutated protooncogene in human cancer, mutated in 15-20% of malignancies. APC mutation is seen in very few other tumors (eg, gastric, esophageal cancers) |
|
|
What are the functions of p53 and RAS in normal cells?
|
p53 is “guardian of genome”. With DNA damage, normal p53 gene causes cell cycle arrest in G1, providing time for repair of DNA damage. If repair is successful, cells enter cycle again; if not successful, p53 gene causes cell death by apoptosis.
RAS is normally a signal-transduction molecule. When cells receive growth promoting stimulus, RAS-GDP is converted to RAS-GTP which is active form of RAS, and sends growth promoting signals to nucleus. Normally, RAS-GTP is rapidly converted to its inactive form by hydrolysis of GTP to GDP |
|
|
How does genomic instability influence neoplastic transformation?
|
Genomic instability contributes to neoplastic transformation indirectly, by predisposing to mutations in protooncogenes and tumor suppressor genes
|
|
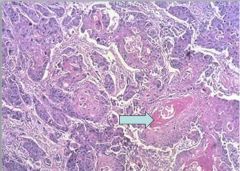
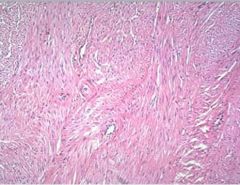
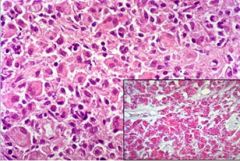
What is this? What stage? What would consistency of tumor be based on stromal appearance? What is the pink material in between tumor cells?
|
Breast adenocarcinoma
Moderately differentiated Hard and gritty. Collagen makes it hard or scirrhous. Collagen Gland formation can’t be seen readily, because glands are compressed by thick collagenous stroma. |
|
|
How is estrogen receptor expression involved in etiology of this tumor?
|
Estrogen may bind to receptors on tumor cells and promote growth.
Estrogen is not mutagenic, but it is a tumor promoter, not a tumor initiator. |
|
|
Significant of CSF samples in terms of cancer?
|
If signet ring cells are found it indicates that cancer has metastasized a lot(Stage IV)
|
|
|
which mutations associated with initation?
|
APC
|
|
|
Which mutations associated with tumor progression?
|
p53, RAS, DCC
|
|
|
Other than Colon cancer, what else is Colon carcinoembryonic antigen increased in?
|
gastric, pancreas, lung or breast cancer.
also alcoholic cirrhosis, hepatitis, UC, Crohn disease. Healthy smokers |
|
|
What must invasive cells be capable of to perpetuate?
|
Invasive cancer cells must be able to bind to basement membrane and extracellular matrix by laminin receptors and fibronectin receptors.
To degrade ECM, they produce proteolytic enzymes (e.g., collagenase). |
|
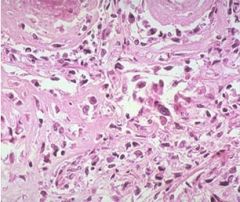
what is this?
|
metastatic colon adenocarcinoma to liver
|
|
|
NF I patients have benign neurofibromas in or attached to nerve trunks. NF I patients have increased risk of _________
|
neurofibrosarcoma (Malignant Peripheral Nerve Sheath Tumor).
|
|
|
In a neurofibroma, it is likely that both NF1 alleles are inactive. By comparison, normal cells of a NF1 patient have only one inactivated allele. This inactive NF1 is inherited in the germline providing the first hit, according to the two-hit hypothesis of tumor development.
|
|
|
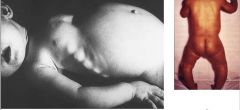
Describe Kwashiorkor
|
Kwashiorkor. “Sugar baby” In this form of malnutrition, due to protein deprivation, subcutaneous fat and muscle mass are relatively spared.
There is generalized edema (due to hypoalbuminemia), reflected in puffy eyelids, face and extremities. |
|
|
Describe Marasmus
|
Marasmus When dietary protein and calorie deficiencies are proportional, subcutaneous fat and skeletal muscle are catabolized to provide energy, amino acids, initially sparing viscera.
|
|
|
Describe what the liver of a malnourished child would look like.
|
Liver of child with kwashiorkor is yellow, fatty, due to reduced serum levels of carrier proteins.
The liver of the child with marasmus is normal, extremities show wasting. |
|
What is wrong with this child?
|
Rachitic Rosary Defective bone mineralization leads to overgrowth at costochondral junctions, producing bead-like expansions (hence designation rosary).
Pigeon-breast deformity also apparent. Rickets - Hypocalcemia due to vitamin D deficiency leads to insufficient mineralization of osteoid matrix, causing weakness of bones. In a growing, ambulatory child, this weakness causes legs to bow outward, producing a varus deformity. |
|
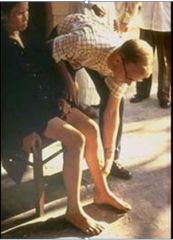
Whats up here?
|
Beriberi, ankle edema. Beriberi is manifestation of thiamine (vitamin B1) deficiency, characterized by high-output congestive heart failure, resulting in peripheral edema, as evident in dependent pitting edema in this patient.
In U.S., alcoholism is a common cause of thiamine deficiency. |
|

What's up?
|
Pellagra, dermatitis, before and after treatment
Dermatitis of niacin deficiency has redness, thickening, roughening, scaling of exposed skin, most noticeable on the hands, neck and nose. It can also affect mucous membranes of mouth and vagina. |
|

Why?
|
Zinc deficiency leads to distinctive rash, known as acrodermatitis enteropathica, typically surrounds eyes, nose, mouth, anus, extremities.
Growth retardation, altered immune function, and infertility also occur with zinc deficiency. |
|

what?
|
Skin, follicular hemorrhage, vitamin C deficiency
Hemorrhages have affected hair follicles, producing small red dots (petechiae). Periosteum, joint spaces and central nervous system can also be affected. |
|
|
Describe lung that has pnuemocystis pneumonia
|
heavy, red, atelectactic
bilateral fluffy infiltrates, prominent at hilum, base. |
|
|
normal lung
|
|
|
How is response to therapy assessed in AIDS patients?
|
PCR amplification of HIV-1 is currently the method of choice for assessing viral load and response to therapy in patients with AIDS.
|
|
|
What other types of specimens are typically collected to detect Pneumocystis?
|
Bronchial washings or sputum samples are collected to diagnose Pneumocystis
|
|
|
HIV stratification of categories is based on....
|
CD4 count
>500 ul is low probability of progression <200 is high probability of progression |
|
|
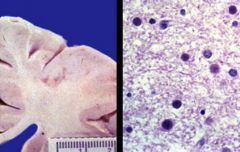
most common CNS disease in AIDS. What does it look/present like?
|
Primary HIV encephalitis causes progressive decline in cognitive function, with memory loss, withdrawal. Affects deep gray matter, white matter, causes white matter pallor,
|
|
|
What stain is used for myelin?
|
Luxol fast blue
|
|
|
Can you think of another disease in immunosuppressed patients that may result in demyelination?
|
Progressive multifocal leukoencephalopathy is another disease that may result in demyelination in this patient population.
|
|
|
How does HIV-1 meningoencephalitis differ pathologically from HIV-1 aseptic meningitis, which occurs 1 to 2 weeks after seroconversion?
|
HIV-1 aseptic meningitis, although not well studied, typically shows a mild lymphocytic meningitis with some myelin loss. HIV-1 meningoencephalitis is typified by a parenchymal inflammatory reaction that occurs in a scattered and perivascular pattern.
|
|
|
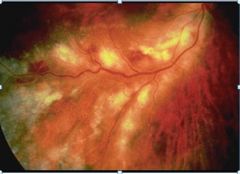
What happens to retina in AIDS?
|
CMV infection - hemorrhage, purulent exudate, ulceration, CMV inclusions in retinal cells.
|
|
|
What are more common organs involved by CMV infection in immunocompromised host?
|
Most often, CMV is in salivary glands, kidneys, liver, lungs, gut, pancreas, thyroid gland, adrenal, brain (to name a few!).
|
|
|
CMV
|
|
|
Microglial nodule with multinucleated giant cell. Oligodendroglia, astrocytes, macrophages proliferate as response to injury, forming microglial nodules.
Specificity for HIV-1 can be demonstrated with immunoperoxidase stain with antibody for HIV p24 antigen. |
|

What's wrong?
|
Small bowel, nodular Mycobacterium avium-intracellulare infection
|
|
|
What are common pathogens producing diarrhea in patients with AIDS?
|
The common pathogens producing diarrhea in patients with AIDS include Mycobacterium avium-intracellulare, Cryptosporidium or Isosporidium, and cytomegalovirus. In addition, a general rule is that any pathogen that infects the immunocompetent patient may also infect the immunocompromised patient, which would put all the common bacterial and viral pathogens on this list as well
|
|
|
How would the MAI picture differ pathologically from cryptosporidiosis?
|
Cryptosporidium is not invasive, they attach to superficial portions intestinal epithelium. MAI are in histiocytes in lamina propria, submucosa.
|
|
|
Small bowel, Mycobacterium avium-intracellulare infection Mucosa packed with histiocytes. Organisms in histiocytes stain red with acid-fast stain.
|
|
|
How do CMV infections differ in immunocompetent vs. immunosuppressed patients?
|
In immunocompetent, acute CMV infection resembles acute infectious mononucleosis.
In immunosuppressed, CMV disease, whether (acquired primarily or by reactivation), can be disseminated, fulminant, lethal with multiorgan involvement. |
|
|
What sort of cells does CMV turn up in?
|
CMV may infect a variety of cell types, including epithelial, endothelial, mesenchymal cells
|
|
What is this...
Point out where each structure is.... Pseudomembrane Necrotic mucosa Residual crypts Macrophage nucleus CMV inclusion |
CMV infection of colon
|
|
|
What are the similarities, pathogenetically, between this picture and Clostridium difficile-associated pseudomembranous colitis?
|
Both CMV and Clostridium difficile may produce colitis with pseudomembranes. In CMV disease, the pseudomembranes result from direct epithelial necrosis and, probably more importantly, ischemic necrosis secondary to vascular damage by CMV. In C. difficile-associated pseudomembranous colitis, the pseudomembranes result from toxin-mediated destruction of the epithelium, as well as ischemic necrosis secondary to thrombosis of underlying small vessels.
|
|
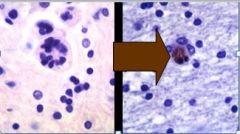
What is important about the image on the left? What caused it?
|
PML is caused by a papovavirus that infects the oligodendroglia directly, causing necrosis. Because the oligodendroglia produce myelin, demyelination occurs in the infected areas, noted in the image on the left. The characteristic histologic feature of PML, seen on the right, is infection of the oligodendroglial nuclei, resulting in a glassy smudged appearance of the chromatin.
|
|
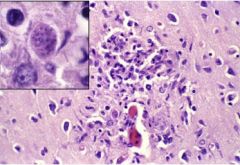
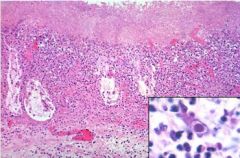
What is seen that is important in these pictures?
What is this caused by? |
This shows an area of necrosis infiltrated by reactive, rod-shaped, microglial cells. Such clusters of microglial cells are called microglial nodules. The high-power inset demonstrates a cyst of Toxoplasma organisms containing multiple bradyzoites.
Toxoplasmosis, an opportunistic infection. It affects AIDS and bone marrow transplant |
|
|
What other organs are most commonly involved by Toxoplasma?
|
Toxoplasma causes pneumonitis, lymphadenitis, chorioretinitis, encephalitis.
|
|
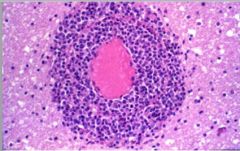
What is important about this?
|
CNS lymphoma cause mass in brain, perivascular lymphomatous infiltrate. Characteristically B-cell neoplasms associated with EBV reactivation in immunosuppressed population. Majority contain EBV genome.
Virus most likely causes prolonged B-cell activation, with superimposed additional genetic alterations, cells become malignant. |
|
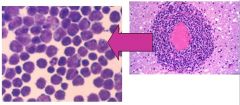
What is this from?
|
CSF sample taken from a patient affected with CNS lymphoma due to EBV.
|
|
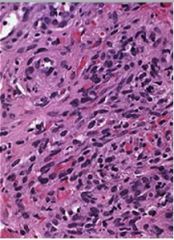
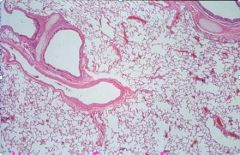
What is this?
|
Sample of Kaposi Sarcoma
sarcoma purple-red vascular tumor with plump spindled cells outlining vascular spaces. Extravasated erythrocytes are also common. KS has been associated with Kaposi sarcoma-associated herpes virus (KSHV) found in virtually all Kaposi sarcomas, both AIDS-associated and non-AIDS associated. The jury is still out on whether virus causes lesion, is cofactor, or is incidental. |
|
|
What is the intestinal manifestation of Kaposi Sarcoma?
|
Patients with Kaposi sarcoma may have life-threatening hemorrhage from intestinal involvement by Kaposi sarcoma
|