Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
130 Cards in this Set
- Front
- Back
|
define papule, macules, patch, plaques, nodules, bulla, vesicles, pustules. wheals, lichenification, and scale
|
macules- flat color change less than 5mm
patch - flat color change more than 5mm papule- raised lesion less than 5mm plaque- raised lesion usually flat top more than 5mm nodule- eleveated rounded top more than 5mm bulla- more than 5mm blister vesicles- less than 5mm bllister pustules- puss full wheals- red hives lichenifcatino- caused when an area is over scratched or rubbed leads to color change scale- whitish boarder due to hypertrophy of stratum corneum |
|
|
what is hyperkeratosis
|
hypertrophy of the stratum corneum
|
|
|
what is parakeratosis
|
when there is nuclei in the stratum corneum due to excessively rapid growth
|
|
|
what is hypergranulosis?
|
thickening of the stratum granulosum
|
|
|
what is Acanthosis?
|
when the whole epidermis is thickened espeacially the stratum spinosum
|
|
|
what is papillomatosis?
|
when the epidermis forms papules
|
|
|
what is dyskeratosis?
|
abnormal growth and development of keratinocytes.
|
|
|
what is acntholysis
|
break down of keratinocytes adhesion to each other makeing them more rounded should make you think of pemphigus
|
|
|
what is vaculolar
|
damage to the stratum basalis from lymphocyte injury leads to halo areas with destuction to the lower keratinocytes.
|
|
|
what is spongiosis
|
edema in the epidermis leads to mini blister
|
|
|
what is hydropic change
|
inter and intra cellular edema often brought on by infections like herpies.
|
|
|
exocytosis
|
inflamatory cells like lymphocytes moving up into the epidermis
|
|
|
what is lentiginous
|
proliferation along the basal layers of the epidermis mainly used in melanocytic lesions
|
|
|
what is solar elastosis
|
when over exposed to sun fibroblasts make elastic fiber mix that leads to loss of stability can cause wrinkles.
|
|
|
where do seborrheic keratosis usually arise
|
can occur anywhere but mainly on trunk
|
|
|
what is leser-trelat
|
sudden burst of seborrheic keratosis indicative of paraneoplastic syndrome sign of underlying malignancy most commonly a GI tumor brought on by growth facto alpha
|
|
|
what doe seborheic keratosis look like
|
black to dark brown, stuck on appearance, greasy, age spots
|
|
|
how is seborrheic keratosis appearing under microscope
|
hyperkeratosis
aconthosis basloid keratinocytes epidermal inbaginations keratin filled HORN CYCST often contian melanin pigment |
|
|
discribe acanthosis nigricans
|
not a tumor
reactive hyperlasia in reponse to growth factor vevety thickend skind most cmomonly in flexed areas usually hyperpigmented Can be indicative of underlaying condition benign or malignant(80% benign) AD heritbable trait obesity and diabetes can be seen with GI malignancies. |
|
|
discribe actinic keratosis
|
seen in fair complexioned people
damage induced by UV thought of as a precancer can be brought on by arsenic can progress to squamous cell carcinoma |
|
|
what is the appearence of actinic keratosis
|
macule or papule that has scale
|
|
|
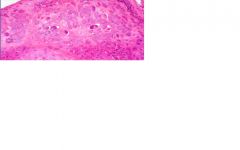
what is the appearche of actinic keratosis under microscope
|
hyperkaratosis
parakeratosis dysplasia of lower epidermis solar elastosis NOT FULL THICKNESS |
|
|
describe squamous cell carcinoma
|
2nd most common tumor arising in sun exposed sites followng basl cell carcinoma
small risk of metastize flesh colored firm ulceration |
|
|
what mutation is squamous cell carcinoma associated with
|
mutation in p53
|
|
|
what are some risk factors for squamous cell carcinoma
|
UV ligh
industrial carcinogens chronic ulcers old burns immunosuppresion xeroderma pigmentosa |
|
|
what is seen under microscopic squamous cell carcinoma
|
hyperkeratosis;pearakeratosis
acanthosis dysplasia of ENTIRE EPIDERMIS extension of tumor into dermis squamous perls solar elastosis |
|
|
what is the most common malignant skin tumor?
|
basal cell carcinoma
|
|
|
describe basal cell carcinoma
|
locally invasive but rarely metastasize
Male over 60 head and neck fair skin chronic UV exposure immunosuprrsion Nevoid basl cell carcinoma syndrome |
|
|
how does basal cell carcinoma present
|
papules or nodules
smooth surface TRANSULUCENT WITH TORTUOUS VESSELS(telangiactasia) central ulcer |
|
|
how do basal cells appear under microscope
|
retraction artifact
periperal pallsading central ulcer attach to basal layers lobules and island of blue appearing cell |
|
|
what is Nevoid basal cell carcinoma syndrome?(NBCCS)
|
AKA gorlin syndrome, basal cell nevus syndrome
multiple Basal Cell Carcinomas(less than 20 yrs) also multiple other tumors; medulloblastomas, ovarian fibromas, odontogenic keratocysts, palmar/plantar pits, intracranial calcificatino, rib abnormalities Autosomal dominant |
|
|
what is the gentic basis of NBCCS
|
PTCH gene on 9q22.3
-receptor for SHH gene product -uninhibited acitivatino of SMOOTHENED leads to increased transcription factor P53 |
|
|
discribe keratoacnanthoma
|
may be benign vs malignant probably malignant
nonagressive appear as large nodule with large central keratin filled crater cup shap keratin plug glassy keratinocytes |
|
|
what is vitiligo?
|
partial or comlete loss of pigment producing melanocytes
macuels and pathces of pigment loss hands wrists and acilae, perioral/orbaital, anogentil koebneriztion (scratching makes it worse. autoimmune/inflammatory disease may respond to UV light therapy |
|
|
what are lentigos
|
benign localized hyperlasia of melanocytes
not same as freckle(ephelis) which is just increased amount of melanin pigment linear melanocytic hyperplasia w/ thinning and elongation of rete pegs |
|
|
describe acquired melanocytic nevi
|
macules and papules
tan to black regular in shape and border less than 5mm |
|
|
what are the list of melanocytic nevi
|
junctional nevi
compound nevi intradermal nevus |
|
|
what is a junctional nevi
|
flat
melanocytes only in the epidermis |
|
|
what is a compound nevus
|
raised
melanocytes in the dermis and epidermis |
|
|
what is the intradermal nevus
|
raised
melaocytes only in the dermis |
|
|
what are the features of normal noncancerous nevus
|
symmetric
predominant nest pattern(alltogether) no mitotic figures in the dermis maturation with nuclie get smaller with descent into dermis. |
|
|
what are congenital melancytic nevi
|
large nevi born with
slightly increased risk of melanoma |
|
|
what is the clinical significance of dysplastic nevus
|
isolated lesions: no real risk
multiple lesions: slight increased risk of melanoma dysplastic nevus syndrome (atypical mole syndome, BK mole syndrome: definite increased risk |
|
|
what type of nevi are usually dysplasitc
|
compund or junctional
|
|
|
what charactizes a dysplatic nevi
|
briding nests
shouldering dermal fibroplasion single cell lentiginous proliferations irregular nuclear outlines w/hyperchromasia. |
|
|
what are the clinical warning signs of melanoma
|
enlargments of preexsting mole
itching or pain in a mole development of new pigmented lesion after 60 asymmetric shape size(>6mm) |
|
|
what is the abcde of melanoma
|
asymetry
boarder color diameter 6mm evolution |
|
|
what are the two phases of patholgic growth for melanoma
|
radial and vertical growth phase
RGP: intraepidermal growth minima dermal inovlvment VGP: signifcant invasion into dermis |
|
|
what are the implications of the radial and vertiacl growth phases
|
while in RGP removal of the spot can produce cure. once it progresses to VGP the risk for metastasis is much higher.
|
|
|
what is the most key indicator of prognosis for melanoma?
|
depth deeper the worse
Clarks level(anatomic location ie epidermis dermis. BRESLOW LEVEL measured level accurate |
|
|
what are clarks levels
|
level 1. confined to epidermis:100% cureable
level 2. invasion into papillary dermis:no real metastatic potential level 3. tumor filling papillary dermis: level 4. invasion of reticualr dermis level 5. invasion of subcutaneosu tissue |
|
|
what is breslow levels
|
perpendicular distance from granular layer(stratum granulosum first thin layer under stratum corneum) measured in MM MOST IMPORTANT PROGNOSTIC INDICATOR
breslow > 1mm will get a sentinel node procedure. |
|
|
what are the histologic features of melanoma?
|
asmmetry
irrrgular nests single cell pattern pagetoid spread-nest of melanocites moves up from the SB nuclear atypia absence of maturations dermal mitotic figures |
|
|
what are the characters of lentigo maligna melanoma
|
typically on the face
slow growing better prognosis caused by sun damage not genes |
|
|
what is the major thing to know about superficial spreading melanoma?
|
the most common subtype melanoma
|
|
|
what are the characters of acral lentiginious
|
hand and feet
most commonly seen in AA and Asian more aggresive |
|
|
What is the characters of nodular melanoma
|
lacks radial growth phase goes straight into vertical growth phase so its more aggressive
|
|
|
what are the best prognostic indicators for melanoma?
|
breslow <1.7 mm
absence /low mitotic figures brisk tumor infiltrating lymphocytes no regression femal gender location on extremity skin tumor thickness small absence of ulceration lower clincal stage |
|
|
what are important genes to understand about melanoma?
|
deletions of p16INK4A
BRAF and NRAS |
|
|
describe benign fibrous histiocytoma(BFG/dermatofibroma(DF)
|
benign dermal neoplasm of fibroblasts and histiocytes
appears most often in middle aged women appears as firm tan brown papules less than 1cm dimple sign may result from abnormal response to injury |
|
|
what is a good clue fore DF/BFG histiolgically
|
increased fibroblasts that trap(wring) colligen.
|
|
|
describe dermatofibrosarcoma protuberans (DFSP)
|
slow growing plaque, later nodular
middle aged male trunk proximal extremities most common site locally recurrent metastasis rare |
|
|
what is characteristic of DFSP
|
fat trapping
hard to get the whole thing on biopsy pinwheeling |
|
|
discribe mycosis fungoides
|
cutaneous T cell lymphoma
unocommon lymphoma but most common lymphoma of the skin older adults early stages mimic exzema progresses from patch to plaque to nodule |
|
|
how is cutaneous T cell lymphoma(mycosis fungoides) staged
|
based on surface area and lymph node involvment
|
|
|
what is sezary syndrome
|
erythrodermic stage or mycosis fungoides (when the tumor invades the blood)
|
|
|
what are the histologic features of mycosis fungoides
|
psoriasiform epidermal hyperllasia (acanthosis)
epidermotropism- malignant lymphocytes in the epidermis pautrirers microabscesses: collections of atypical lympohcytes in epidermis cerebriform nuclei- sezary lutzner cell DISEASE OF CD4 clonal subset of T cells |
|
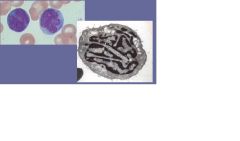
what is this a picture of?
|
sezary cell indicative of mycosis fungoides
|
|
|
what is a spongiotic pattern of inflamation
|
intraepidermal edema
|
|
|
what is psoriasiform pattern of inflammation
|
epidermal acanthosis
|
|
|
what is interface
|
damage to basal layer
|
|
|
what are the two types of interface
|
vacuolar interface- perivascular inflammatory cells around blood vessels
lichenoid interface- inflammatory cells arranged as dense band beneath epidermis |
|
|
what is bullous disease
|
blisters can be intraepidermal or subepidermal
|
|
|
what is panniculitis
|
inflammation of the fat
|
|
|
what is spongiotic dermatitis associated with
|
excema
|
|
|
what are teh primary features of spongiotic dermatitis
|
very common
intraepidermal edema accumulation of edema fluidwithin epidermis keratinocytes pull apart intraepidermal vesicles may see some acanthosis |
|
|
decribe the normal character of eczematous dermatitis
|
red papulovesicular, oozing and crusting
|
|
|
what is the pathogenesis of contact dermatitis
|
antigens processed by dendritic langerhans cells
langerhans cells migrate to regional lympho nodes antigen presentation stimulates naive T cells rash develops on re exposure secondary to cytokine production from T Cells |
|
|
what are the features of psoriasiform dermatitis
|
epidermal acanthosis main featur
variable perivasuclar infiltrate variable spongiosis seen in psoriasis |
|
|
what is the common character of psoriasis
|
chronic dermatitis
common in population develop on any age linked to increase risk for heart disease can cause a psoriactic arthritis |
|
|
what is a gene that can cause psoriasis
|
HLA cw0602
|
|
|
what is the pathology of psoriasis
|
disorder of keratinocytes hyperproliferation
cytokine soup and TNF implication exact mech unknown |
|
|
what does psoriasis look like
|
red to salmon pink plaques with silvery scale
pitted nails with yellow discoloration |
|
|
what is auspitz sign
|
seen in psoriasis
pinpoint blood hemorraghes seen after picking off scales |
|
|
what are the most common sites of psoriasis
|
extensor surfaces like knees and elbows
scalp,lumbosacral region, gluteal cleft glans penis |
|
|
what is the histiologic features of psoriasis
|
uinform acanthosis
-test tube in a rack confluent parakaratosis -retained nuclei in the SC diminished to absent granular layer thinned suprapapillary plate with dilated tortuated vessels parakeratotitc scale with neutrophils |
|
|
what is a new therapy for psoriasis
|
vitabmin D3
topical analoque has been used as a first line therapy inhibits epideramal proliferation and inducies normal differentiation |
|
|
what diseases can lead to interface dermatitis
|
perivascular:
erythema multiform/TENacute lupus erythematosus chronic lichenoid: lichen planus |
|
|
discribe erythema multiforme
|
dramatic hypersensitivity response: HSV, mycoplasma, fungal mycobacterial
drugs malignancies collagen vascular disease it is a specturm of diseases |
|
|
what is most common cause of erythema multiforme
|
Herpes simplex virus
|
|
|
what is a key feature that can be seen in erythema multiforme
|
it is variable with no typical presentation but TARGETOID lesions are common
|
|
|
what is steven johnson syndrome
|
a type of erythema multiforme
extensive disease with oral and ocular involvemtn fever children more than adults drugs are most common cause.antibiotics looks really bad |
|
|
What is toxic epidermal necrolysis
|
TEN
a type of erythema multiforme extensive sloughing skin just peels off. resembes really bad burns mucosal invovlments caused by drugs |
|
|
what is the hisoligc features of erythema multiforme
|
superifcial perivasuclar lymphocitc infiltrate
prominent edema of papillary dermis degeneration and necrosis of keratinocytes leading to full thickness necrosis |
|
|
what are the dermatalogic importances in lupus
|
systemic acute lupus- butterfly red rash
subacute lupus eryhematosus- asociated with drugs, chronic lupus erythemaotosus (discoid lupus) most common seen in derm - thin atrophic plaques with hyperpigmentation and hypopigmentation, hair loss, can present with vaculoar interface |
|
|
what can be done to diagnose lupus
|
lupus band test for immunoglobulins and complement at the DE junction. all types are usually present
|
|
|
describe lichen planus
|
chronic but sefl limiting disease
multple symmetric lesions on extremities, espeacially wrists, elbows and penis PURITIC, PURPLE, POLYGONAL, PAPULES interface dermatitus type lichenoid damage to the basal layer by a lot of lymphocytes. very itchy koebners phenomenon oral invovlment along membranes |
|
|
what is wickham stiae?
|
light whitish scale found on lichens planus
|
|
|
what is koebners phenomenon?
|
appearance of lesion along site of injury
|
|
|
what are the key aspects to catagorizing bullous dermatosis?(blisters)
|
subcorneal, intraepidermal, or subepidermal
histologic features and immunoflourescense bullae= large blister vesicles= tiny bilsters |
|
|
describe pemphigus vulgaris?
|
presents in 4-6 decade of life
autoimmune blistering disease -IgG antibodies target desmoglein in desmosomes bullous dermatosis nikolsky sign |
|
|
what are the variants of pemphigus vulgaris
|
pemhpigus vegetans(presensts wart like plaques
foliaceus (more benign form epidemic in S. Amerca. |
|
|
describe the lesions in pemphigus vulgaris
|
bullous dermatosis
flaccid fragile bullae scalp, face, acilla, groin, trunk, pressure points most often already eroded bc so fragile often has oral involvment |
|
|
what is nikolskys sign?
|
blister can be induced by simply applying pressure
|
|
|
what is the histiologic presentation of pemphigus vulgaris
|
INTRAEPIDERMAL suprabasilar blister
mixed dermal inflammatory infiltrate with eosinophils tombstome basal layer acantholysis eosinophils in epidermais(eosinophilic spongiosis |
|
|
what is seen on immunofluroescence in pemphigus vulgaris?
|
IgG and complement deposists between keratinocytes in a netlike intercellular pattern
|
|
|
discribe bullous pemphigoid
|
similar to pemphigus vulgaris
NO ORAL INVOVLMENT autoimmune disease -IgG antibodies against hemidesmosomes protiens hemidesmosomes bind epidermis to basement membrane bullae on extremities, intertriginous areas, abdomen. tense bullae not flaccid like pemphigus vulgarus often intact on arrival not erroded. |
|
|
what are the histiologic finding in bullous pemphigoid
|
SUBEPIDERMAL SPLIT
no tombstones no acantholysis eosinophils will be found in edema |
|
|
what is the immunoflourescence seen on bulllous pemphigoid
|
LINEAR IgG and complement depositino along basement membrane. NO NET PATTERN like in vulgaris
|
|
|
discribe dermatitis herpetiformis
|
visicular dermatotis not bullous
3 to 4 decade of life more in males found in extensor surfaces of extremiteis, and upper back and buttocks very itchy associated with celiac disease responds to gluten free diet IgA antibodes against basment membrane anchoring fibrils |
|
|
what is the histiologic findings on dermatits herpetiformis
|
subepidermal vesicles
neutrophilic microabscess |
|
|
what is found on immunofluorescense of dermatitis herpetiformis
|
Granular IgA deposits in dermal papillae and alonge basement membrane
|
|
|
discribe the character of Acne
|
multifactorial disorder affecting the pilosebacieous units
brought on by: androgens, folicular obstruction, propionibacterium acnes, heredity, drugs, contactants , occlusions |
|
|
what are teh histologic features of acne vulgaris
|
plugged follicle-comedone
dilated folicle-papule, pustule, cyst ruptured follicle-inflammed neutrophil nodule |
|
|
discribe panniculitis
|
inflammmation of the subcutaneous fat
|
|
|
discribe erythema nodosum
|
panniculitis
associtatied with infectinos (betat hemolyti strep) drugs (oral contraceptive, sulfonamides) sarcoidosis, IBD, presents on anterioro lower legs, tender erythematous nodules |
|
|
what is the histolgy of erythema nodosum
|
widening of CT septa of the fat with neuts, eos, lymphs, histiocytes, and multinucleated giant cells,
|
|
|
what is dermatophytosis
|
ringworm
superficial fungal infection with infectino of out keratin layer of skin |
|
|
what is gross presentation of dermatophytosis
|
expanding annular erythematoius plaque with elavated scaly border
|
|
|
what is the histologic presenation of dermatophytosis
|
hyperkeratosis
parakeratosis neutorphils in keratin hyphae in keratin PAS stain demonstrates the hyphae |
|
|
what causes warts(verrucae)
|
benign neoplasm caused by HPV
|
|
|
what subtypes of verrucae are associated with increased risk of squamous cell carcinoma
|
16, 18, 33
|
|
|
what is seen histiologically in verruca vulgaris
|
papillomatosis
aconthosis dilated toruous vessels hyperkeratosis koiocytes |
|
|
what are koilocytes
|
keritinocytes develope halos around them seen in verruca vulgaris
|
|
|
what is the presentation of molluscum contagioosum
|
common in kids
dome shaped papules with a central keratin filled crater, found on face trunk and anogenital areas easily spread though contact DNA poxvirus |
|
|
what is seen on histology in molluscum contagiosum
|
molluscum body: eosinophilic cytoplasmic inclusion in upper layer of epidermis
|
|
what is this
|
molluscom body found in molluscom contagiosum
|
|
|
discribe impetigo
|
common superfical infection
STAPHYLOCOCCUS exposed surfaces like face and upper extremeities characterisitc honely colored crust neutrophils on histology |
|
|
what are the types of herpiesvirus infectinos
|
HSV1- cold sores, fever blisters, oral infections most common, cutaneous blistering eruption , usuall linear
HSV2- genital herpes VZV- chicken pox, zoster |
|
|
what are the 4 Ms of herpes
|
cytoMegaly
Multinucleation Molding- nuclei flaten onto each other Margination-nuclear chromit pushed out to the edges of the nuclei |