Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
28 Cards in this Set
- Front
- Back
|
Abbreviations: ACh, AChe, ChR, n-Ch, m-Ch
|
ACh - acetylcholine
AChe - acetylcholinesterase ChR - cholinergic receptor nCh - nicotinic cholinergic mCh- muscarinic cholinergic |
|
|
Terms: Apnea, Bradycardia, hyperkalemia, hypokalemia, NMJ, vagolytic
|
Bradycardia-slow down heart rate
hyperkalemia- high serium K+ levels hypokalemia - low serum K levels NMJ- neuromuscular junction Vagolytic - blocking input from vagus nerve |
|
|
Enzymatic hydrolysis of acetylcholine: how and what does this do?
|
Breakdown of ACh by acetylcholinesterase in the snaptic cleft into acetate and choline
This will form inactive metabolites |
|
|
Non-depolarizing type Nicotinic Cholinergic Receptor Antagonists: Curare Like and Aminosteroids
|
Curare-like: Cisatracurium and Mivacurium
Aminosteroid type: rocuronium, pancuronium, vecuronium |
|
|
Depolarizing types of Nicotinic Cholinergic Receptor Antagonists
|
Succinylcholine
|
|
|
Neuromuscular Blocking Drugs: what do they do
|
They facilitate paralysis of muscles (intubation of trachea, mechanical ventillation, surgical procedures)
Used in an iv route in a hospital setting with anesthesia usually. Can control Convulsions (electroshock) |
|
|
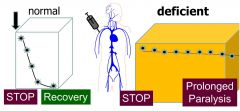
Sequence of how muscles are affected by neuromuscular blockers
|
-first the small muscles, rapid muscles are affected (eyes, fingers)
-then bigger muscles Recovery occurs in the opposite order Consciousness and sensorium: not affected at all because they do not cross blood brain barrier Overexposure causes respiratory depression which is a factor in morbidity/mortality during anesthesia |
|
|
Nicotinic Receptor Antagonist: mechanism of action
|
Blocks the site of ACh binding. Will competitively block ACh binding
|
|
|
Curare drugs and their properties: why do we not use them and how are they altered to be "curare-like" which is the form we use
|
Minimal clinical use because there is Extreme histamine release which will cause a dramatic drop in blood pressure.
Curare drugs are also hypotensive and cause ganglionic blockage in other areas of SNS We transform drugs chemically to avoid the histamine release, hypotensive and ganglionic blockage and make them curare like |
|
|
Cisatracurium
|
Slow onset (5 min)
Long acting (90 min) Clearance: SPONTANEOUSLY through blood plasma Histamine Release: NONE, absent Because of it's clearance, it is given to patients during liver and renal failure (think about why) |
|
|
Mivacurium
|
Fast onset (1 min)
Short acting (15 min) Clearance: Enzymatic Clearance through blood plasma Enzyme responsible for clearance: pseudocholinesterase/butyrylcholinesterase (same one) ^must lower dose during renal/hepatic(liver) failure |
|
|
Mivacurium Clinical Complications
|
1/3000 have defective plasma pseudocholinesterase gene: makes the enzyme activity lower
Elimination is slower in these people. At conventional doses for these people, we can have a prolonged paralysis and strong risk for apnea (loss of external breathing) |
|
|
Aminosteroid Nicotinic Cholinergic Receptor Antagonists: what are they and how do they work (competitive or noncompetitive?)
|
Pancuronium, Vecuronium, Rocuronium
Functions via Competitve Inhibition (same mech) At appropriate levels they do not accumulate in the ANS of the PNS and they do not go to the CNS |
|
|
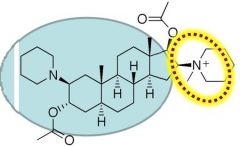
Pancuronium: qualities
|
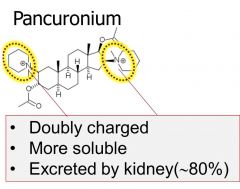
Long acting (60 minutes)
Slower onset Clearance: Renal Elimination ^this is because it is a double ion charged species Only Aminosteroid that can bind to muscarinic receptors. Has a vagolytic effect (stimulation of vagus nerve slows down heart rate) and will cause tachycardia or speeding of the heart because the vagus nerve will be inhibited |
|
|
Vecuronium and Rocuronium
|
Intermediate Acting (15-45 min)
Rocuronium Has a very rapid onset (less than 1 min) Clearance: both eliminated via biliary elimination These are singly charged, detergent like, and use biliary excretion |
|
|
Complications with Nueromuscular blockade by nondepolarizing type antagonist: what happens?
|
Paralysis of muscles due to prolonged exposure to drug
How to manage this? Either wait, intubate for respiratory failures, or manipulate the system to get ACh back into the system |
|
|
Clinical Reversal of Paralysis
|
Inhibiting acetylcholinesterase will raise ACh levels at synapse and overcome blockade by competitive nicotinic cholinergic receptor antagonists
|
|
|
Why reverse neuromuscular blockade? What drugs accomplish these?
|
NM blockade will impair respiration:
We want to restore spontaneous respiration, prevent airway aspiration Nyostigmine, pyridostigmine, edrophonium will all accomplish this. |
|
|
ACHesterase Inhibitors: how do they work
|
They work by keeping a high amount of ACh in the synaptic cleft because AChesterase cannot break down the ACh.
Then this will eventually end up overcoming the competitive inhibition. |
|
|
Neostigmine, pyridostigmine, edrophonium: what are they, what can they affect (think what receptors), and what happens with overuse? ALSO what can counter the overuse effects?
|
Charged species that will not cross into the CNS
Neostigmine and Pyridostigmine are long acting (2-4 hrs) and Edrophonium is short acting (10-20 min) These can work either at nicotinic AND muscarinic receptors Overuse can cause autonomic toxicity: peripheral muscarinic receptor effects and somatic nicotinic receptor effects Atropine can counter these effects Clinical presentations of ACHesterase inhibitors: Bradycardia, bronchospasm, bronchorrhea |
|
|
Atropine
|
mCHr Antagonist - will counter the effects of overuse/overdose of AChesterase inhibitors
|
|
|
What happens if ACHesterase inhibitors do not work to overcome the overdosage of a neuromuscular antagonist?
|
Must perform mechanical ventilation when there is substantial overexposure
|
|
|
Depolarizing Blockade of Nicotinic Cholinergic Receptors at NMJ: which drug and how?
|
Succinylcholine: two ACh molecules fused together
Partial agonist : initially contracts the muscle Phase 1: membrane depolarization with transient fasiculations which is followed by flaccid paralysis SUC has a higher affinity for nACHr so it stays bound to the receptor like an antagonist Phase II: Membrane repolarizes but SUC remains bound and receptor is desensitized to ACH SUC will also make a new resting membrane potential: about -55 mv |
|
|
Clinical Issues regarding the use of a depolarizing antagonist
|
During Phase two of SUC depolarizing antagonist mechanism:
nACHr will always be occupied by SUC and therefore it will keep K channels open. This will cause high intracellular levels of K This high level of K+ is not good especially in burn patients, traumatic injury, and can lead to heart attack |
|
|
Succinylcholine metabolism: how is it done and genetic complications?
|
Metabolized in plasma by pseudocholinesterase
Elimnated slower in synapse (synapse doesn't have as much pseudocholinesterase) 1/3000 patients have mutation in pseudocholinesterase : will cause SUC to eliminate slower than normal. Patients could experience malignant hyperthermia from too many fasiculations |
|
|
Adverse effects of Succinylcholine
|
Bradycardia via cardiac muscarinic receptors, Postoperative myalgia(muscle pain), Apnea, Malignant hyperthermia (treated with dantrolene).
SUC overexposure (esp when admin with halogenated gaseous anes.) causes excessive Ca discharge + excessive muscle contraction = a rise in body temp. ^^need to ice bath patient, administer dantrolene (ryanodine receptor antagonist which will relax muscle peripherally) |
|
|
Dantrolene: how does it work and clinical manifestations
|
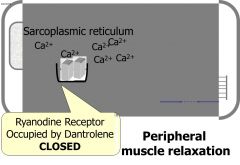
This is a ryanodine receptor antagonist and will occupy the binding site of ryanodine with dantrolene to cause peripheral muscle relaxation
there is a hepatotoxicity risk in females and patients over age 35. This is contraindicated in cirrhosis and hepatitis |
|
|
Ryanodine Receptor
|
Discharge mechanism for Ca to go outside of the SR
|