![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
316 Cards in this Set
- Front
- Back
|
Where are the kidneys located |
retroperitoneal |
|
|
What are the names of the tubes which fluid is transported from kidneys to the bladder? |
Ureters? |
|
|
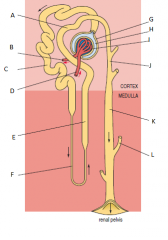
Name the 3 regions of the kidney, starting from the outer layer to the inner layer? |
1. Renal cortex 2. Renal medulla 3. Renal pelvis |
|
|
A - Distal convolute tubule B - Efferent arteriole C - Proximal convoluted tubule D - Efferent arteriole E - Ascending thick limb of loop of Henle F - Descending thin limb of loop of Henle G - Bowman's capsule (forms part of renal corpuscle) H - Bowman's space (forms part of renal corpuscle) I - Glomerulus (forms part of renal corpuscle) J - Cortical collecting duct K - Medullary collecting duct L - Collecting ducts from other nephrons |
|
|
What is the filtered fluid in the kidney referred to as? And what is the name of the tube that collects and processes this? |
filtrate - collected and processed in renal tubule |
|
|
Which structure acts as the filter in the kidney? And where is it located? |
renal corpuscle located in renal cortex |
|
|
How does filtrate leave the glomerulus to enter the renal tubule? |
Filtered out of the blood capillaries across the epithelial cells and into the tubule's lumen |
|
|
What products are mostly absorbed by the epithelial cells of the tubule? |
water, glucose, amino acids, sodium and other ions |
|
|
The 3 main processes involved in the formation of urine |
glomerular filtration tubular reabsorption tubular secretion. |
|
|
What structure do the endothelial cells in the capillaries have which assist in filtration? |
Small pores called fenestrations that allow the passage of small molecules, but large molecules, such as RBC remain |
|
|
How does the gel like extracellular matrix that is secreted by the glomerulus assist in filtration? |
They consist of negatively charged glycoproteins, and repel any other negatively charged molecules in blood (which is most protein macromolecules) |
|
|
What is the volume of fluid filtered per unit of time defined as? Typically, how much per day is this for a 70kg adult? |
Glomerular filtration rate (GFR) ~180 L/day |
|
|
What 3 factors affect rate of blood flow through glomerulus (and therefore filtration rate) |
Pressure in afferent and efferent artrioles (Note: NOT mean arterial blood pressure) Permeability of wall of glomerulus & bowmans capsule Relative concentration of proteins in capillaries & bowmans space (negative osmotic effect, H2O drawn back into capillaries) |
|
|
Where does the majority of the reabsorption of glucose, amino acids and H2O occur? |
Proximal convoluted tubule |
|
|
Describe structure of epithelium cells of descending thin limb of loop of Henle when compared to that of proximal convoluted tubule |
No microvilli and reduced amounts of mitochondria |
|
|
Where does most of the passive movement of H2O and, to a lesser extend, certain ions occur? And what happens to concentration of filtrate? |
Descending thing limb of loop of Henle Concentration of filtrate increases as osmolarity of surrounding tissue is greater than that of the filtrate, draws water in |
|
|
Where are Na+ and Cl− ions absorbed in the nephron? How is this achieved? Which ions are secreted in this area? |
In the thicker part of the ascending limb of the loop of Henle This is done by active transport, and using ATP K+ and H+ are secreted here |
|
|
When does the proximal convoluted tubule become the distal convoluted tubule? And where does it empty in to? |
After it passes close to the glomerulus This empties into the collecting duct system |
|
|
How do reabsorbed molecules return to the body? What is the name of the vascular structure around the loop of Henle? |
Tthe peritubular capillary system which surrounds the tubular system The vasa recta |
|
|
How are glucose and amino acids absorbed by the epithelial cells of the kidney tubules? |
Using active transport - they are transported with sodium ions |
|
|
How is the concentration gradient of sodium achieved to provide the active transport of glucose and amino acids? |
Using the Sodium pump (aka sodium-potassium ATPase) - i.e. sodium is forced out of the basal and lateral sides of epithelial cells to the interstitial fluid, and then removed in peritubular capillary, so concentration of Na in cell is less than that of the lumen of tubule. |
|
|
What is the limiting factor in the reabsorption of glucose or amino acids? |
he number of transporter molecules in the luminal membrane of the tubular epithelial cells. |
|
|
Why is glucose present in urine with diabetes melitus? |
Too much glucose for the transporter proteins, they become saturated so passes through filtrate and excreted with urine |
|
|
What happens to most other useful organic molecules in the first part of renal tubule is they are: 1) water soluble (give examples) 2) lipid soluble (give examples) |
They are reabsorbed by active transport in the first part of the renal tubule 1) Vitamin C (note, if excess amounts, excreted due to the lack of transporter mulecules on luminal membranes of epithelial cells 2) Vit A and D - pass straight through as they are lipophilic! Concentrations rise in body |
|
|
How is urea formed? |
The main metabolic waste product in plasma is urea, which is a nitrogen-containing molecule formed during the catabolism of amino acids |
|
|
What are the key components of waste (i.e. from metabolic reactions) that are excreted in urine? And what happens to them in the kidney? |
Urea is initially filtered at glomerulus, but approx 40-60% of this is reabsorbed. The remainder is excreted in urine. Creatnine, musculo-skeletal waste product of metabolism, initially filitered in glomerulus but not reabsorbed in tubules |
|
|
How is sodium reabsorbed in the tubules? |
By active transport and by facilitated diffusion via protein carriers in the cell membranes of the tubular epithelial cells. |
|
|
What else is affected in relation to sodium transport? |
Co-transport molecules for Na can include: -Glucose & amino acids -bicarbonate or phophate -Na rabsorption with H ions OUT of the epithelial cells |
|
|
What is the ultimate drive for Na absorption? (both active transport and diffusion) |
dependent upon the decreased concentration of sodium inside the tubular epithelial cells, a result of the action of the sodium pump |
|
|
What is the main cause of concentration difference between the tubule and epithelium to allow the passive transport of water? |
Concentration difference of sodium |
|
|
How does the re-absorption of Na affect H2O movement? |
The uptake of Na effectively causes filtrate to become dilute, which in return causes H2O to pass via osmosis out of the lumen into the epithelial cells and diffuse through the gap junction between epithelial cells |
|
|
What ions are added to the filtrate via tubular secretion? And how are these added? What other organic molecules are added via tubular secretion? |
H+ and K+ by active transport coupled with sodium reabsorption Creatinine and penecillin |
|
|
What is the formula to determine how much of a substance is excreted in urine? |
(amount of X filtered + amount of X secreted) – amount of X reabsorbed |
|
|
If a substance is neither secreted nor reabsorbed what is its renal clearance? |
The renal clearance of that substance will be equal to the glomerular filtration rate. |
|
|
Why is createnine used to assess the effectiveness of golmerular filtration? |
Is not re-absorbed and is only secreted in very small quantities, so filtration can be measured |
|
|
What will be the clearance of urea if the plasma concentration is 0.26 mg per ml and the amount excreted is 18.2 mg per min? |
18.2 / 0.26 = 70 ml / min |
|
|
Why systems are in control of the GFR? |
Endocrine and nervous system as these influence the pressures exerted and the dilation / constriction on the efferent and afferent arterioles |
|
|
Why isn't the GFR affected by mean arterial pressure? |
The glomerular system is autoregulated, i.e. when BP increases in the afferent arteries, the arterioles constrict, reducing the blood pressure in the capillaries. However if the pressure is consistently raised, the arterioles will be affected, increasing the GFR |
|
|
What 2 mechanisms are involved in the autoregulation of the kidneys? |
Myogenic mechanism tubuloglomerular feedback mechanism |
|
|
Elaborate on myogenic mechanism |
Myogenic = muscle related. When afferent artery blood pressure increase the arterioles constrict. Reduced pressure causes dilation, raising the hydrostatic pressure |
|
|
Elaborate on tubuloglomerular feedback mechanism |
Responds to the flow of filtrate within the tubule. This mechanism is controlled by specialized cells located in juxtaglomerular apparatus. These cells are macula densa cells, and juxtaglomerula cells which lie around the arterioles. These cells produce the enzyme renin, and one of its actions decrease the diameter of blood vessels, thus increasing pressure. |
|
|
What is the significance of the cell arrangement of the juxtaglomerular apparatus? |
Changes in composition and nature of filtrate in tubule, e.g. osmotic pressures, are detected by macula densa cells, which release factors that diffuse to juxtaglomerular cells which effect renin production that alter state of contraction of arterioles therefore flow rate |
|
|
What is the countercurrent multiplier system? |
The osmolarity pressure increases with distance into the medulla from the cortex. The existence of the gradient means that, as the filtrate passes along the collecting ducts, the osmolarity of the extracellular fluid surrounding the ducts increases, allowing reabsorption of water, by osmosis, along the whole length of the ducts. |
|
|
Outline the two major categories of kidney disease |
glomerulonephritis – the inflammation of the glomeruli. glomerulosclerosis – the scarring or hardening of the blood vessels of the glomerulus and kidney. |
|
|
What happens when infection causes albuminuria? |
albumin is protein found in blood which draws fluid out of tissue into blood stream to be excreted in urine. Without this protein, oedema builds up. |
|
|
What is diuresis? |
excreting large volumes of water |
|
|
When is ADH secreted? |
When osmoreceptors in the hypothalamus detect an increase in osmolarity in both extra and intracellular fluids. I.e. there is a reduced amount of water in the system. |
|
|
How does ADH enter the system? |
Hypothalmic neurons which produce ADH extend to posterior pituitary , where ADH is secreted |
|
|
How does ADH affect water reabsorption? |
It specifically affects a class of membrane proteins called aquaporins , a class of up to 4 proteins that form channels on epithelial cell membranes. ADH affects AQP2 only by increasing the amount of pores in luminal membrane - i.e. more water moves out of lumen and less is lost in filtrate |
|
|
What else stimulated ADH secretion? |
Strech receptors in cardiovascular system: Volume receptors found where veins return blood to heart - detect small changes in blood volume Baroreceptors - arterial pressure receptors |
|
|
When do we feel urge to drink? |
Thirst receptors in hypothalamus activated by increase in osmolarity of extracellular fluids. |
|
|
What happens if water levels are high? |
ADH will not be secreted, as the osmoreceptors and baroreceptors that project to the ADH-producing neurons in the hypothalamus will not be appropriately activated. If ADH is not present, the rate of water absorption in the collecting ducts will be very low, and increased volumes of dilute urine will be produced |
|
|
If there is a reduction in Sodium, the GFR is reduced (due to reduced pressure in afferent arterioles). What will this allow? |
The reduction in GFR will allow increased reabsorption of sodium, and hence also of water, reducing further sodium loss. This is another example of negative feedback. |
|
|
How does renin blood vessels |
Renin cleaves angiotensin I from angiotensinogen which is produced by the liver. This is converted to Angiotensin II via angiotensin converting enzyme which is located on endothelial cells. Angiotensin II causes constriction of blood vessels, particularly in efferent arterioles in nephron. This raises GFR. |
|
|
What happens when sympathetic nerves detect drop in BP? |
fall in blood pressure is detected by the volume and pressure receptors, activating sympathetic nerves. These cause a constriction of blood vessels, particular renal afferent arterioles, slowing down GFR. This slow down in GFR causes Renin to be released from juxtaglomerular apparatus. |
|
|
How does aldosterone affect sodium level regulation? |
It increases sodium reabsorption from the collecting ducts. It does this by stimulating an increase in the synthesis of sodium transport proteins in the epithelial cells in this region.
|
|
|
How is aldosterone secretion stimulated? |
Angiotensin II stimulates aldosterone production |
|
|
A decreased hydrogen ion concentration is known as? |
Alkalosis |
|
|
Carbon dioxide (CO2) combines with water to form carbonic acid (H2CO3), which dissociates (breaks up) to form hydrogen ions and bicarbonate ions (HCO3−). What is the chemical equation for this? |
CO2 + H2O <> H2CO3 <> HCO3 + H+ C A Bicarb |
|
|
If we were to inhale more carbon dioxide, how would this affect the equilibrium reaction shown above? |
An increase in the concentration of carbon dioxide will bring about an increase in the level of carbonic acid which in turn will increase the concentration of hydrogen ions. |
|
|
how do most hydrogen ions appear in the body? |
as a result of aerobic respiration |
|
|
What would you expect to happen to the free hydrogen ion concentration in the plasma if bicarbonate ions are removed and excreted in the urine? |
Removal of bicarbonate ions would have the effect of ‘pulling’ the reaction shown above to the right, thus raising the levels of free hydrogen ions in the circulation. |
|
|
How is pH maintained in kidney? |
Bicarbonate is filtered through glomerular, therefore in filtrate. Endothelium cells produce H+ and Bicarbonate ions and are secreted to lumen. These then convert to CO2 and H2O and are subsequently reabsorbed into epithelial cells. Once all bicarb has been converted and re-absorbed, technicially there is no net loss of bicarb in circulation. H+ ions will bind to other non-bicarb buffers, resulting in net loss of H+ ions and net gain in HCO3- ions. |
|
|
How does urine travel to bladder? |
From the kidney via the ureters, which are comprised of smooth muscles lined with epithelial cells. Peristalsis forces urine through. |
|
|
What two structures are present in bladder to retain fluid? And what are they composed of |
Internal and external urethral sphincter which are composed of smooth and skeletal muscle respectively |
|
|
How is the urge to urinate manifested? |
Stretch receptors present in muscle surround bladder. When bladder is full, these stimulate the muscle around the bladder and to contract and the internal urethral sphincter to open. The external urethral muscle remains under voluntary control |
|
|
How does the prostate affect the bladder? |
When the prostate enlarges it can clamp on the urethra, impeding urine flow. Overtime the bladder wall will become thicker and irritable - and will begin to contract even with small amounts of urine, eventually losing ability to empty itself |
|
|
What hormone is produced and released from the kidney itself? And what does it do? |
Erythropoietin stimulates the proliferation of undifferentiated precursor cells present in the bone marrow. These precursors give rise to red blood cells. |
|
|
What stimulates erythropoietin release? |
by a decrease in oxygen concentration in the blood supply to the kidneys. |
|
|
Explain the interaction of Ca and the kidney? |
Approx 50% of calcium is filtered via glomerulus and is mostly absorbed back into the tubules. The rest of the Ca is bound to proteins so is too large to be filtered. |
|
|
What 2 hormones play a crucial role in the regulation of the plasma calcium levels? |
parathyroid hormone, and the active form of vitamin D. |
|
|
How is the parathyroid hormone secreted? And how does it work? |
Stimulated when plasma calcium levels are low. It increases the reabsorption of calcium by the tubular epithelial cells and it increases calcium release from bone and activates vitamin D (which results in increased absorption of calcium from the gut). |
|
|
Can you explain how inhibition of sodium reabsorption results in an increase in the volume of urine excreted? |
Water is reabsorbed passively, by osmosis, largely as a result of sodium reabsorption, which raises the osmolarity of the extracellular fluid. Inhibition of this process results in more urine being excreted. |
|
|
How does CCF result in kidney failure, and therefore oedema which requires treatment from diuretics? |
the contractility of the heart is reduced, resulting in a reduction of blood pressure, which, in turn, causes a reduction in GFR, reduced flow in the tubules and hence, via the renin–angiotensin system, increased aldosterone production and sodium reabsorption |
|
|
How do diuretics reduce BP? |
Treatment results in lowering of the content of water and sodium in the body, and reduction in arteriolar dilation. |
|
|
Explain haemodialysis |
Blood diverted from artery to semi-permeable tubing, allows passage of water and small molecules (urea), but not large molecules (proteins). Tubing is immersed in dialysing fluid which contains molecules that isn't typically excreted via kidney and as a result these build up in plasma with kidney failure. Therefore, these substances diffuse out. The fluid contains bicarb and glucose which diffuse in. |
|
|
Explain peritoneal dialysis. |
instead of using artificial membrane, use peritoneal membrane, a thin vascular tissue layer which covers the abdomen. |
|
|
Name 4 constituents of blood |
Plasma Red cells (erythrocytes) White cells (leukocytes) Platelets |
|
|
What is the name of the process which renews erythrocytes? And how is it initiated? |
Haematopoiesis, initiated via hormone erythropoetin |
|
|
Where are the undifferentiated stem cells found in haematopoeitc tissue of marrow found |
found mainly in the pelvis, sternum, vertebrae and skull |
|
|
What is the haematocrit ratio? And what is the normal value? |
Blood is centrifuged, separating all erythrocytes to a stack. The height of the compacted stack is measured against the height of thecolumn of blood, the volume percentage occupied by erythrocytes can be determined. Normal ratio is 45% |
|
|
Outline the 4 main types of anaemia |
nutritional anaemia - Fe deficiency. Low Hgb content therefore reduced O2 carrying capacity Pernicious anaemia - reduced B12 absorbed in gut, therefore lack of production and maturation of erythrocytes Haemorrhagic anaemia - excess blood loss Haemolytic anaemia - erythrocytes ruputre, releasing contents to plasma. E.g. Sickle Cell |
|
|
What is β-thalassaemia anaemia? |
An inherited disorder caused by defect in the synthesis of β globin chains on HGb, reducing O2 carrying capacity |
|
|
What is leukaemia? |
Ca of bone marrow, uncontrolled proliferation of abnormal immature white cells - causes reduced ability to combat infection |
|
|
What defines the blood groups? I.e. A, B, AB and O |
Presence of surface anitgens, i.e. blood type A have A antigens, AB have both and O have none. |
|
|
Explain the Rh factor |
A type of antigen which are either present or absent on erythrocytes, denoting whether-or-not they have positive or negative blood types. 85% of blood types are positive. No natural antibodies develop against Rh factor, however, if negative blood type, antibodies will develop after first exposure to Rh antigen, and can react to secondary transfusions. Rh positive can have either positive or negative transfusion. Negative only have negative. |
|
|
Why do you think the separation of oxygenated from deoxygenated blood is important? |
It is essential not to mix deoxygenated and oxygenated blood, in order to maintain an adequate supply of O2 to the tissues. If they were allowed to mix, then the blood O2 content would be reduced. |
|
|
The circulatory system consists of 2 separate circuits and is therefore a "double circulation system". What are these circuits? |
Pulmonary circulation heart > lungs > heart Systemic circulation heart > body > heart |
|
|
AS blood passes through the pulmonary artery, what gases are released via the lungs? |
CO2 and H2O vapour (keeps lung membrane mosit, increasing efficiency of gaseous exchange - gases must be dissolved in solution before entering the body) |
|
|
Describe the pericardium |
Double-walled sac, filled with lubricating fluid. Encloses heart with outer pericardial membrane attached to connective tissue which separates the two lungs |
|
|
What is the pulse wave? |
The distension and constriction of the elastic tissue in the arteries when the heart beats, forcing blood along the vessels. |
|
|
What are the walls of arterioles primarily composed of? And for what purpose? |
Mainly smooth muscle - contract and relax when innervated. This is by noradrenergic nerves (sympathetic nerves use noradrenaline as neurotransmitter) causing contraction, or cholinergic nerves (parasympathetic nerves using acetylcholine as neurotransmitter) causing dilation |
|
|
Explain how arterioles are key in relation to blood pressure? |
They are an extensive network, and are very narrow with the ability to constrict or dilate and as a result provide the main resistance to blood flow through body Consequently, blood vessels of the arteriolar system are sometimes referred to as the arteriolar resistance vessels. |
|
|
What does peripheral resistance mean? |
Refers to the resistance of the systemic circulation to blood flow |
|
|
What are capillary pores? |
The spaces between the endothelial cells in capillary walls. When damaged, or infected bypathogens, they become large enough for blood and plasma plasma proteins to pass from capillaries to affected tissue as part of the defence or repair mechanism. |
|
|
Describe the properties of veins |
The walls of the venules and veins are much thinner and contain less smooth muscle and elastic tissue than the corresponding arterial walls. However, they have a larger internal diameter and are very distensible and are referred to as venous capacitance vessels, as the can act as a peripheral reservoir. |
|
|
How much smooth muscle is in the venous system? And the revelance of this? |
Not as much as arterioles, but they can still be stimulated by noradrenaline from sympathetic nerves causing vasoconstriction. This can allow the venous system to adjust to accommodate the amount of blood flowing through the system back to the heart, influencing how much work the myocardium has to perform |
|
|
What junctions do cardiac cells connect to each other via, and for what purpose? |
Gap junctions - this permits the spread of electricity from one cell to the next and ensures it is rapid and uniform |
|
|
Where is the SA node located? |
in right atrium, where vena cava enters |
|
|
What will happen to the SA node and surrounding cardiac tissue (atria and ventricles) if it is excised? |
SA node tissue will beat up to ~85 bpm, atrial tissue slightly slower and ventricular rhythm at approximately 1/3 of this rate. |
|
|
What happens to the speed of electrical impulse once it reaches the AV node? |
AV delay - slows down. Allows atria to complete their contraction before Ventricles |
|
|
Explain pathways of electricity for one heart beat |
SA Node > AV node > atrioventricular (AV) bundle (HIS) > Left and right branches of AV bundle > Purkinje fibres |
|
|
What is a complete heartbeat consist of, and what is it known as? And how long does it take? |
Known as a cardiac cycle - consists of period of systole and diastole, lasts approx 0.85 seconds |
|
|
Significance of cardiac monitoring in lead II? |
Lead II is chosen because it shows the heart’s electrical activity along the interventricular septum, the major axis of the heart |
|
|
What does the QRS complex represent? |
Ventricular depolarisation and atrial repolarisation |
|
|
What does the seldom seen U wave represent? |
slow repolarization of the papillary muscles |
|
|
How is cardiac output measured? |
Stroke volume x heart rate CO = SV x HR |
|
|
70 BPM Cardiac output: 5 lpm What is stroke volume? |
Cardiac Output = Stroke Volume x Heart Rate Stroke volume = Cardiac output / Heart rate Stroke volume = 5 L/per min - 5000 ml/per min / 70 bpm 5000 / 70 = 71.4 ml per beat |
|
|
What is Starling’s law? |
That the stroke volume of the heart increases in response to an increase in the volume of blood filling the heart |
|
|
What do sympathetic nerves use to stimulate the heart? And where do these nerves originate? |
Noradrenaline, nevers originate in vasomotor centre in medulla |
|
|
Where do the parasympathetic nerves originate? And how do they descend? And what neurotransmitter do they use? |
cardio-inhibitory centre in medulla, extending via the 10th cranial nerve (vagus nerve) They use acetylcholine |
|
|
How is the SA node kept in check? What is it known as? |
Under tonic inhibition of parasympathetic vagus nerve - vagal restraint |
|
|
Where are Baroreceptors found? |
in carotid sinus and walls of aorta |
|
|
Explain what happens if blood pressure is increased? |
Baroreceptors detect this, relay information to cardio-inhibitory centre in medulla, where the vagus nerve will be stimulated to produce acetylcholine and induce bradycardia, lowering cardiac output and BP |
|
|
What 3 factors contribute to peripheral resistance? |
the thickness (viscosity) of the blood the length of blood vessels through which the blood flows friction between the blood and the vessel walls - i.e. decrease in diameter in lumen increases friction and therefore bp |
|
|
name of sounds heard when taking BP? |
Korotkoff sounds |
|
|
What is the pulse pressure? |
Difference between systolic and diastolic values. |
|
|
What neurotransmitter stimulates: A) Vasoconstriction B) Vasodilation And what happens to the subsequent BP? |
A) Noradrenaline (Sympathetic NS) increases BP B) Acetylcholine (Parasympathetic NS) decreases BP |
|
|
What other substances affects blood vessels |
Adrenaline & Noradrenaline (adrenal glands) Angiotensin II causes vasoconstriction, particular in efferent renal arteriole, increasing GFR ADH (increases H2O retention, but moderate amounts cause vasoconstriction) |
|
|
What is it called when BP is affected by circulating substances? Give examples and the effects they have |
Humoral control Examples are Bradykinin and histamine released by damage cells and in response to allergies - causes local vasodilation |
|
|
What is metabolic autoregulation? |
Metabolically active organs require more O2 and nutrients. The initial decrease in O2 and increase in CO2 (from respiration) trigger local vasodilation, increasing blood flow meeting metabolic deman |
|
|
Explain the coronary circulation |
Blood leaves aorta to reach 2 coronary arteries which branch within the walls of heart forming capillary beds, where gaseous exchange occurs. The capillaries drain to coronary veins and ultimately into coronary sinus, a small valve regulated opening which drains blood into right atrium. |
|
|
What 2 sets of arteries supply blood to the brain? |
L and R internal carotid arteries & L and R vertebral arteries |
|
|
Difference between L and R internal and external carotid arteries? |
Internal carotids enter the brain, external are on both side of neck only |
|
|
What happens to the L and R internal carotid arteries? |
Side branch off to form ophthalmic arteries, and ultimately give rise to anterior and middle cerebral arteries |
|
|
Describe the origin and pathways of vertebral arteries and what they branch off to form? |
vertabral arteries branch off from sub-clavian arteries, and ascend either side of vertabral column, and ultimately form the basilar arteries on approach to brainstem |
|
|
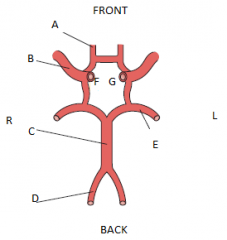
A - anterior cerebral arteries B - middle cerebral arteries C - basilar arteries D - vertebral arteries E - posterior cerebral artery F - right internal carotid G - left internal carotid |
|
|
What are the junctions of endothelial cells in blood brain barrier? For what purpose? |
Tight junctions - Restricts entry of potentially harmful particles put allows passage of o2 and nutrients |
|
|
What advantage does the ‘circle of Willis’ give cerebral blood supply? |
If one of the arteries serving the brain becomes blocked, flow of blood around the ‘circle of Willis’ could ensure that this blockage is compensated for by blood from another artery. In this way, the ‘circle of Willis’ acts as an ‘arterial shunt’ and provides a system of blood vessels that can deliver blood to all the brain cells |
|
|
What substances can passively enter blood-brain barrier? |
ipid-soluble ones, such as O2 and CO2, as well as nicotine, caffeine, alcohol and heroin. |
|
|
As blood brain barrier is effective at blocking potentially harmful substances, how do most of the required molecules, such as glucose and amino acids, pass through to enter the brain? |
via active transport |
|
|
Describe circulations in fingers, toes, palms and earlobes? |
Have shunts which connect arterioles to venules. bypassing capillaries. |
|
|
Describe the shunts in the extremities and how they react with different temps |
Rich nerve supply and thick muscular walls and close to the skin so they lose heat easily. When temp is hot, sympathetic activity decreases, therefore vasodilation, causing decrease in peripheral resistance, therefore increased cardiac output (note starlings law) and then increased blood flow to skin and heat loss is induced |
|
|
How is an increase in blood flow to the skeletal muscle brought about? |
Vasodilation in the skeletal muscle capillary beds and a decrease in peripheral resistance and an increase in venous return from exercising muscles will in turn increase cardiac output. |
|
|
What is special about the arteriole arrangement of the glomerular capillary bed? |
Unlike any other capillary bed found in the body, the glomerular capillary bed drains into an arteriole and not a venule. Afferent to efferent arterioles - the high BP is the force behind the filtration |
|
|
What are the structural differences between afferent and efferent arterioles in kidneys? And what is the reason behind this? |
The afferent arterioles have a larger diameter than the efferent arterioles and it is this arrangement that allows a high pressure to be maintained across the glomerular capillaries. Also, afferent arteriole protects the glomerulus from large fluctuations in arterial bp |
|
|
What is the "second capillary bed" of the kidney and how do they arise? What is it used for? And how does it differ? |
Peritubular bed - arise from the efferent arterioles draining the glomerulus, and is lower pressure. Used fir absorbing solutes and water from tubular cells and returning blood to renale venules. |
|
|
What values constitute as HTN? |
>160 mmHg systolic >95 mmHg diastolic |
|
|
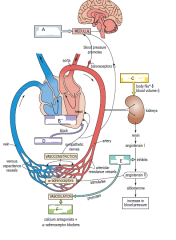
A - centrally acting drugs B - mainly B1 adrenoreceptors C - Thiazide & loop diuretics D - Beta blocks E - ACE inhibitors F - Vasodilators |
|
|
What do beta blockers block specificially? |
adrenoceptors which are activated with noradrenaline. Both β1-and β2-adrenoceptors are present in heart muscle, but the β1 subtype greatly outnumbers the β2 subtype in a ratio of about 3 : 1 so beta blocks block typically B1 subtypes. |
|
|
Can you foresee any side-effects of drugs aimed at β2-adrenoceptors in bronchial, vascular, intestinal and uterine smooth muscle? |
Yes. They may also influence heart function by affecting cardiac β2-adrenoceptors. Note- salbutamol is a B2 agonist and makes you tachy |
|
|
Side effects of beta blockers? |
Can affect B2 adrenoreceptors, causing vasodilation in extremities causing cold extremities.
Also, can cause fatigue, particular in exercise due to reduced cardiac output |
|
|
Name the 2 types of diuretic drugs, and what they do? |
Thiazide and loop diuretics act on distal tubules and thick ascending limb of loop of Henle respectively. They work to reduce circulating volume. |
|
|
How do 2 types of vasodilator reduce BP? |
Decrease vasoconstriction by acting as Ca antagonists, thus blocking the action of Ca2+ ions which, when bond to Ca channels, cause vasoconstriction. Also blocking α1 adrenoreceptors which are involved in noradrenaline mediated vasoconstriction |
|
|
How do ACE inhibitors work in relation to an over stimulation of the renin–angiotensin–aldosterone system? |
ACE (angiotensin converting enzyme) inhibitors prevent angiotensin II production which is a potent vasoconstrictor and stimulator of aldosterone secretion (promotes H2O and Na uptake). Use of these drugs causes markedly reduced peripheral resistance and blood volume (more Na and H2O excreton) |
|
|
Problems / side effects of ACE inhibitors? And solutions? |
Dual effects of decreased peripheral resistance and increase in Sodium and H2O excretion can cause hypotentsion and renal failure. Solution is to take aldosterone antagonist (spirinolactone) or angiotensin II receptor antagonists (losartan) |
|
|
Which patients shouldn't take ACE inhibitors? |
Patients with reduced renal function as further kidney damage may be cuased |
|
|
Explain actions of central acting drugs |
These affect cardioregulatory regions of the medulla in the brain to produce a reduction in the activity of sympathetic nerves innervating the heart - decreasing force of contraction, therefore cardiac output and BP. |
|
|
Problems / side effects with use of central acting drugs? What happens if stopped taking? |
Associated with reduce O2 uptake and transport, physical exertion is limited. Side effects include headaches, nausea and sedation. If stopped suddenly, can induce rebound hypertension |
|
|
What are arthersclerosis / plaques composed of, and what do they do? |
Deposits of lipid, cellular debris and calcium salts on the inside of arterial walls causing a reduced lumen and elasticity |
|
|
What causes athersclerosis? |
Although the underlying cause is not known, the condition appears to begin with damage to the endothelial cells lining the arteries. Once the damage has begun, the endothelial cells proliferate and lipids (e.g. cholesterol), cell debris and calcium salts are deposited to form the basis of the blockage |
|
|
How do statins reduce cholesterol? |
They lower LDL, cholesterol and triacylglycerol levels by blocking production of the specific liver enzymes that synthesize cholesterol and lipids.
|
|
|
What is the first line of tx for angina? How do they work? |
nitrovasodilators - these work by circulating in the blood and react with compounds in vascular smooth muscle cells to produce nitric oxide (NO), a rapid potent vasodilator thus causing a retention of blood in the peripheral circulation. This reduces venous return, resulting in a decrease in ventricular end-diastolic volume and a reduction in the active distension of the heart wall. The oxygen demand of the heart is thereby decreased, relieving the chest pain |
|
|
What does an infarct consist of? |
a central area of dead cells surrounded by tissue that is ischaemic |
|
|
2 ways atherclerosis causes MI? |
Plaques may cause complete occlusion - many years to occur Thromboembolism |
|
|
Cause and symptoms of CCF? |
Progressive hypertension and CHD. Symptoms include oedema, breathlessness and fatigue |
|
|
Results on CCF? |
Reduced cardiac output causes build up of fluid, thus increasing venous blood to heart ('pre-load') Also reduced flow in renal system activated renin-angiotensin-aldosterone system resulting in peripheral vasoconstriction. This causes an increase in arteriolar resistance which the heart must fight against ('after-load') |
|
|
Aim of Tx for CCF? |
Reduce load and decrease force heart must use when it contracts |
|
|
First line of Tx for CCF? |
Diuretics - excrete Na+ ions and H2O, reducing circulatory volume, pre-load and oedema. ACE inhibitors used for venous and arteriolar dilation by prevention of angiontensin II and subsequent secretion of aldosterone* *n.b. this increases Na channel. No aldosterone = lack of channels and there more H2O and Na excreted |
|
|
If diuretics and ACE inhibitors fail, what else can be used to treat CCF? |
inotropic drugs - increase force of cardiac contractions by indirectly increasing the intracellular concentration of Ca2+ ions in heart cells This increases cardiac output and blood pressure, which improves the flow of blood through the tissues and greatly reduces the ‘load’ on the heart. |
|
|
Tx for AF? Purpose of Tx? |
cardioversion - either drug or electric shock. When shocking, it is to uniformly interrupt the chaotic electrical activity of myocardial cells by simultaneously depolarising them, allowing NSR to resume The aim is for control ventricular rate by re-establishing normal sinus rhythm |
|
|
Explain process, pros and cons of cardioversion via electric shock |
When shocked, it uniformly interrupts the chaotic electrical activity of myocardial cells by simultaneously depolarising them, allowing NSR to resume. The aim is for control ventricular rate by re-establishing normal sinus rhythm. Most people with chronic AF are successfully treated with this method, but will revert back to AF within 1 year |
|
|
Explain how AF is treated with drugs |
Drugs act by increasing the refractory period of the AVN, bundle of His and Purkinje fibres and achieve a prolongation of AVN delay. This reduces AV coupling so that the frequency of impulse transmission from the atria to the ventricles is significantly reduced. |
|
|
Verapamil acts by inhibiting the entry of Ca2+ ions into cardiac cells. If a patient who is already using beta-blockers for severe hypertension starts to get atrial fibrillation, would you prescribe verapamil? |
No. The use of beta-blockers contra-indicates the use of verapamil. A person using beta-blockers will already have a slow heart rate and lowered force of cardiac muscle contraction. Taking verapamil in addition to beta-blockers would further reduce heart rate and the force of muscle contraction, leading to possible ‘cardiovascular collapse’ and death. |
|
|
Explain second degree AV block |
In second-degree AV block (called Mobitz Type II) only a proportion of the atrial impulses get through to the ventricles. For example, only every second atrial impulse might be transferred to the ventricle (called ‘2 : 1 AV block’). |
|
|
How are clots formed within a blood vessel? |
atherosclerotic plaques can break through the weakened endothelial lining, exposing the passing blood to the collagen in the underlying connective tissue. When blood platelets come into contact with collagen, a clot, called a thrombus can form by coagulation. |
|
|
What is the name of the process that stops bleeding? |
haemostasis |
|
|
What happens to a blood vessel following any damage? And how are the platelets activated? |
Immediately constricts as a result of sympathetically induced vasoconstriction - this is known as vascular spasm.
Platelets do not normally adhere to the endothelial surface of vessels. However, following injury, platelets are activated by the underlying collagen to aggregate into a platelet plug, sealing vessel |
|
|
Haemostasis involves other specific blood-borne factors that are involved in a complex chain of biochemical reactions. Explain this "clotting cascade" |
This pathway causes fibrinogen to convert to fiberin mesh, entangling erythrocytes and platelets. This mesh promotes formation of fibrous scar at vessel defect, and is also involved in repair of vessel wall. Clot is not needed, and dissolved by fibrinolytic enzyme called plasmin, remnants of clot phagocytized. |
|
|
Explain the action of A) antiplatelet drugs B) anticoagulants C) thrombolytics |
A) inhibit platelet aggregation
B) inhibit the conversion of prothrombin to thrombin and so prevent the conversion of fibrinogen to fibrin C) dissolve clots by activating the conversion of plasminogen to plasmin. |
|
|
How do varicose veins occur? |
valves in the vein which prevent backflow become ineffective, resulting in a partial backflow of blood, which can lead to a weakening of the vein walls. Superficial veins, predominantly in the legs, may become so elongated and dilated |
|
|
2 types of vasogenic shock and there cause if shock? |
anaphylactic and septic - widespread vasodilation substances in blood |
|
|
What causes postural hypotension? |
Low blood pressure occurs due to insufficient compensatory responses to the gravitational shifts in blood distribution When an individual moves from a horizontal to a vertical position, gravity causes blood to pool in the venous capacitance vessels of the legs. There is a subsequent decreased venous return (pre-load), a decreased stroke volume, a lowered cardiac output (after-load) and a lowered blood pressure |
|
|
What is the full equation for the creation of ATP? |
6O2 + C6H12O6 = 6CO2 + 6H2O + ATP
|
|
|
What 3 things does the respiratory system consist of? |
The lungs (the gas-exchange organ) A system of airways which deliver the air to the blood vessels of the lungs The musculo-skeletal system which ventilates the lungs. |
|
|
What is the 'nasal cycle'? |
Nostril sizes alternate throughout the day |
|
|
From the trachea, what path does the airway take? |
Trachea > Bronchus (pl. bronchi) - each one divides to 2 smaller tubes, which divide into 2 smaller tubes (repeat 14 times) > bronchiole > Terminal brionchioles |
|
|
What is the conducting zone? |
The bronchi, primary bronchioles and terminal bronchioles conduct gas to and from the exterior and thus form the conducting zone |
|
|
How are the terminal bronchioles further divided? |
The terminal bronchioles each divide a further seven times into respiratory bronchioles, > alveolar ducts > alveolar sacs |
|
|
What is the respiratory zone? How is this zone kept clean? |
Gas exchange occurs in the respiratory bronchioles, alveolar ducts and the alveoli, which thus form the respiratory zones. Note: there are no cilia or mucous producing cells. Any shizzle not filtered will be deposited here. May be phagocytosed and transported to lymph nodes, accumulating as black deposits. Any remaining particles can cause chronic disease |
|
|
What is the name of the capillaries that surround the alveoli? |
Pulmonary capillaries |
|
|
How does CO2 and O2 diffuse during gaseous exchange? |
Oxygen from within the alveoli diffuses into the pulmonary capillaries, while CO2 diffuses from the blood into the alveoli. Since the walls of an alveolus and a pulmonary capillary are each only one cell thick, the gases have only to diffuse through a two-cell-thick layer. |
|
|
What is surface tension, and why is it an issue in gaseous exchange? |
It is far more efficient for gaseous exchange to occur by the thin liquid film which lines each alveolus, however, the surface tension causes the properties of the liquid to want to be attracted to neighbouring water molecules (think drop of water) |
|
|
How is surface tension overcome? |
Epithelial cells which line the alveolus secrete surface active agent (surfactant), a detergent-like fluid that reduces surface tension of the film of liquid and helps prevent the alveolus from collapsing |
|
|
When do babies suffer from respiratory distress syndrome (RDS)? Or in adultS? |
If they are premature, the surfactant producing cells are not fully developed, so surface tension is high, resulting in difficulty in expanding alveolus. Smokers experience reduced surfactant |
|
|
What separates the thoracic and abdominal cavities? |
Diaphragm |
|
|
How do lungs remain inflated in the chest cavity? |
Both the lungs and chest wall are covered pleuratic membranes, which are lubricated. The space between the lubricated membranes is known as pleuritic cavity, and the fluid layer allow the lung to move frictionless within the thoracic cavity, and prevents the collapse of the lung by maintaining the surface tension that holds it to the chest wall |
|
|
How does the diaphragm and external intercostals muscles move during inspiration? And how does this cause inspiration? |
The diaphragm flattens, and intercostals move out and downwards. This causes the lungs to expand as they are stuck to the chest wall via surface tension between the 2 pleuratic membranes, and the air pressure of the lungs reduces, causing air to flow into the airway |
|
|
Describe process of expiration. |
Expiration is generally a passive event brought about by relaxation of the diaphragm and external intercostal muscles. The ribcage and diaphragm return, by natural recoil, to their original pre-inspiratory positions, forcing the air out of the lungs |
|
|
What is the definition of tidal volume - and what is an average volume |
The volume of air breathed in and out with every breath, approx 0.5 L |
|
|
What is the inspiratory and expiratory reserve volume? |
Deepest breath possible in & out |
|
|
What is residual volume? |
The small amount of air left in lung post expiratory reserve volume |
|
|
What 2 parameters are measured in peak flow? |
1) the muscular ability to expel air 2) how well air is able to pass out of conducting air passages |
|
|
What does partial pressure of gas mean? |
The concentration of a particular gas in a mixture of gases |
|
|
So what is the PO2 in atmospheric air, it the air is ~760 mmHg? |
21% O2 in Earth's atmosphere. Therefore PO2 is 21 / 100 x 760 = 159.6 mmHg |
|
|
What is the PO2 in alveoli? And how does that compare to atmospheric O2? What does that mean? |
approx 100 mmHg and so is lower partial pressure than 160 mmHg of atmospheric O2 This means that there is a lower percentage of O2 in the alveolar air. |
|
|
Can you suggest why the PO2 in the alveoli is less than the PO2 of the inspired air?
|
Not all of the air that is inspired reaches the alveoli due to the residual volume. This residual volume mixes with the inspired air, and reduces the PO2 of the air in the alveoli, which ensures the PO2 in the alveoli is always less than that of the air entering the lungs. |
|
|
explain PO2 in alveolar and deoxygenated blood, and the significance of this |
Deoxygenated blood is approx 40 mmHg, therefore partial pressure difference allows O2 to diffuse from alveoli (100 mmHg) to blood, giving it a new PO2 of approx 95 mmHg. |
|
|
Explain PCO2 in alveoli and dexoygenated blood, and the significance of this |
PCO2 in alveoli is approx 40 mmHg and 46 mmHg in deoxygenated blood. When blood leaves the lungs, the PCO2 is 40 mmHg signifying it has reached an equilibrium.
|
|
|
Why when O2 diffuses from alveoli to deoxygenated blood there is a 5% discrepancy (from 100 mmHg to 95 mmHg) but there is no discrepancy in CO2 |
Suggests O2 is not as soluble in blood |
|
|
Describe structure of haemoglobin |
Is a protein, made up of 4 polypeptide chains called globins. There are 2 alpha and 2 beta chains. Each globin has an Fe2+ ion in centre which picks up one O2 molecule, therefore each haemoglobin will carry 4 O2 molecules. |
|
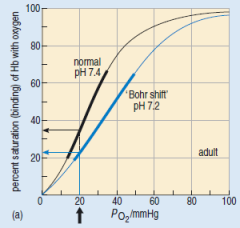
Elaborate (A normal adult dissociation curve (at 37 °C, pH 7.4) and the effect on the position and shape of the curve of increasing the acidity of the blood (pH 7.2) |
The black line represent the disassociation curve, so at approx 40 mmHg PO2, 75% of Hb will bind with O2 become oxyhaemoglobin. The blue line is a more acidotic patient, note the lateral "Bohr" shift, and therefore less efficient and there is a decreased affinity The steepest part (thickened) represents the most efficient regions of O2 and Hb binding. |
|
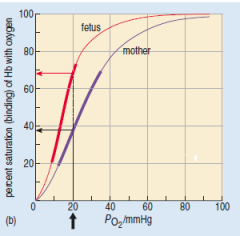
Elaborate (Dissociation curves for a mother and fetus (at 37 °C, pH 7.4).) |
Fetal haemoglobin has two gamma chains in place of the beta chains of adult haemoglobin, endowing it with a higher affinity for O2 than the adult form. Consequently, the oxygen–haemoglobin dissociation curve for fetal haemoglobin is shifted to the left.
At PO2 of 20 mmHg the mother is approx 39% saturated, and fetus is 69% saturated. |
|
|
Outline 3 forms in which CO2 is carried in blood |
1) 10% dissolved in plasma, dependign on on PCO2 differences between plasma & tissue 2) 30% bound to hb - carbaminohaemoglobin. Note this is bound to globin, not the haem! 3) 60% as Bicarb ions (HCO3-) or carbonic acid (H2CO3) dissolved in plasma |
|
|
What is carbonic anhydrase? Where is it found? What does it do? |
Carbonic anhydrase an enzyme found in in erythrocytes and speads up the reaction between CO2 and H2O to form carbonic acid |
|
|
What happens when CO2 enters the erythrocyte? And why? |
Immediately reacts with H2O and the presence of the carbonic anyhydrase enzyme to produce carbonic acid. This conversion keeps the CO2 level in the cell low, keeping a constant PCO2 gradient difference between surrounding tissue and cell. This allows the majority of CO2 in circulation to enter eythrocytes. |
|
|
Why is it important to consider speed in relation transferring tissue CO2 to erythrocye? i.e. why use carbonic anhydrase? |
Blood spends on average 0.75 seconds in the capillary and so the time available to pick up a full load of CO2 from the tissues is very short. The presence of carbonic anhydrase allows the rapid uptake of CO2 into the blood. |
|
|
Within the erythrocytes, carbonic acid disassociates to form bicarbonate ions and H ions - thus causing a reduction in pH. How does the erythrocyte counter this? And as a result, what happens to the oxygen? |
The H ions are biochemically buffered by haemoglobin, thus keeps there levels in safe amounts. Furthermore the presence of H+ ions displaces O2 via haldene effect - causing the O2 to detach from oxyhaemoglobin, out of the erythrocyte and diffuse into tissue. This is more evident in tissues that are metabolically active as there will be a higher amount of CO2. |
|
|
Explain the chloride shift |
As HCO3- ions are produced in the erythrocyte when CO2 enters, these ions diffuse out of the permeable membrane. As these negative ions leave the cell, the cells has an excess of positive charge ions, however, the cell's membrane is not permeable to these. To balance this, Cl- ions diffuse in. |
|
|
What are the respiratory centres in brain for involuntary (automatic) respiration? And which branch of nervous system controls this? |
Pons and medulla Operated by autonomic nervous system |
|
|
Where is the respiratory centre for the voluntary control of respiration? And which branch of nervous system controls this |
cerebral cortex Operated by somatic nervous system |
|
|
How do the respiratory centres receive information about the respiratory status of the body? |
from muscles and tissues via nerves, and from the blood by chemical stimuli – and sends out impulses to the respiratory muscles to increase or decrease the rate of breathing as appropriate |
|
|
Which nerve innervates the diaphragm? And where does it originate from? Which nerve innervates the intercostal muscle? |
Phrenic nerve, originating in respiratory centre of medulla Intercostal muscles innervated by thoracic nerves |
|
|
How do the neurons regulate rate of ventilation? |
There are two types of neuron in the respiratory centres which both send impulses to the phrenic and thoracic nerves. The first set are fire during inspiration (the "inspiratory neurons") and the second set of neurons fire during expiration (the "expiratory neurons"). The inspiratory neurons inhibit the firing of the expiratory neurons and vice versa. |
|
|
Which 2 factors cause inspiration to terminate? |
1) activity in respiratory centre which inhibits breathing 2) Stretch receptors in lungs tell brain when lungs have hit full capacity. The inspiratory neurons stop firing and relieve the block on the expiratory neurons, which leads to relaxation of the inspiratory muscles |
|
|
How are central chemoreceptors used in relation to the control of respiration? |
Central chemoreceptors in medulla respond to H+ concentration in CSF. If concentration increases, these cells become more active, increasing the activity of respiratory centre - increase rate of ventilation. |
|
|
How are peripheral chemoreceptors used in relation to the control of respiration? |
Found in carotid arteries and aorta, and respond to the decrease in O2 in blood. |
|
|
Name 4 non-respiratory functions of respiratory system |
1) To talk 2) To smell 3) Water loss and heat elimination (especially dog) 4) Provides defence mechanisms against inhaled particulate matter |
|
|
What is pneumonia? |
Inflammation and fluid filling of alveoli |
|
|
What is asthma, and how is it treated? |
Swelling of airway linings & over-production of mucus. Treated with bronchodilators with B2 adrenoreceptor agonists and iprotropium bromide, that block the bronchoconstrictive action of parasympathetic acetylcholine are also administered |
|
|
How is asthma managed long term? |
Corticosteroid drugs are prophylactic agents - reducing bronchial muscosal inflammatory reactions and modify cellular reactions to potential allergens |
|
|
Explain the tonic inhibition of SAN |
SAN is under "vagal restraint" with average heart rate of 60-70bpm. This parasympathetic vagus nerve is initiated in the cardio-inhibitory centre in medulla. Without it, the intrinsic heart rate of SAN is approx 90bpm |
|
|
What causes sinus arrhythmia? |
During inspiration, stretch receptors relay info via sensory axons in the vagus nerve to medulla in order to inhibit inspiratory nerves and to allow expiration. This inhibition is also relayed to cardiac centre and the vagal restraint is also relieved, causing increase in heart rate. This process is in reverse during expiration. |
|
|
what will happen if the baroreceptors detect a decrease in blood pressure. |
A reflex increase in blood pressure would occur. This would result from a reduction in the firing rate of the nerves from the baroreceptors to the cardiac and respiratory centres, causing a decrease in parasympathetic activity of the vagus nerve to the heart, and hence an increase in heart rate. Stroke volume would be increased and vasoconstriction would occur due to an increase in the firing rate of sympathetic nerves. Cardiac output and total peripheral resistance would increase, thus increasing arterial blood pressure. |
|
|
How do periods of apnoea occur? And what condition is this linked to. |
When we are asleep, control of respiration is not as vigorous, and there is a decrease in the sensitivity of the chemoreceptors when relaying info regarding PCO2 levels. Believed to be initiated when tongue blocks the airway due to loss of tone, and resulting CO2 build up is not detected and the reflex mechanism (i.e. to breath and get more O2) is not initiated. This is linked to SIDS |
|
|
What are the physiological and psychological benefits linked to laughter? |
blood pressure, to stimulate the immune system, favourably alter mood and reduce stress – indicating that humour can be good for your health |
|
|
What are the first anticipatory mechanisms which are implemented prior to exercise? |
Activation of sympathetic nervous system and release of adrenaline, increasing strength of ventricular ejection fraction |
|
|
Briefly outline changes in body that occur during times of increased metabolic demand - i.e. during exercise. |
-vasoconstriction of arterioles increase bp -vasoconstriction of venous system for increased venous return, increasing stroke volume and cardiac output -vasodilation of muscle blood vessels -High CO2 levels act as local vasodilator -Increased temp and increased concentration of H+ ions causes Bohr shift - so O2 is released from Hb at higher partial pressure, so is transferred to tissue cells more readily |
|
|
By what mechanism is the increased demand for O2 in the body detected? |
The decrease in PO2 and the increase in PCO2 in the blood, following the increased use of O2 by exercising muscles, is detected by both central and peripheral chemoreceptors. |
|
|
How does a build-up of lactate lead to an increase in O2 delivery? |
An increase in acid concentrations in the muscles will shift the oxygen– haemoglobin dissociation curve to the right and this will increase the release of O2 from oxyhaemoglobin |
|
|
Explain why post-exercise oxygen consumption (EPOC) occurs. |
Lactate is produced during anaerobic exercise, and is either subsequently converted to glycogen stores in liver or used by muscle tissue to create ATP. Both of these processes require O2 to complete, so the demand for O2 is still high even after completing exercise. |
|
|
In exercise, how does the "second wind" occur? |
During sustained exercise, the demand for O2 can be partially met. This provides this "steady state". |
|
|
What are the major physiological variables that affect maximal O2 consumption (or max. VO2)? |
- cardiac output - functional capacity of lungs - efficiency of gaseous exchange in lungs - efficiency of delivering oxygenated blood to working muscle - the efficient operation aerobicactivity in muscle cells. |
|
|
What happens to PO2 with increased altitude? And what happens if you go up too quick? |
PO2 Decreases - symptoms of hypoxia. E.g. mountain/altitude sickness |
|
|
What are the 5 compensatory mechanisms to overcome increased altitude? |
- increased breathing (low PO2 and high PCO2 detected by chemoreceptors) - increased erythrocyte and Hb production -increased blood volume (therefore increased output and amount flowing through lungs) -increased vascularisation of tissue -adaptive resome for tissue to utilise O2 at higher PCO2 |
|
|
Why do deep sea divers need to breathe compressed air? What is the drawback from this? |
The air needs to be a higher pressure than the sea or their lungs would collapse. The nitrogen is also under pressure and is forced into alveoli and forced into (primarily) lipid rich tissues. If the diver comes out of the environment of high pressure too quickly, the nitrogen comes out of gas and forms bubbles - THE BENDS! |
|
|
What is the diving response? |
An innate physiological response when submerged in water |
|
|
What happens during anoxia? |
Ventilation stopped immediately and after about 30 seconds vagus nerve stimulates bradycardia, arterioles cosntrict but flow remains to heart and brain |
|
|
What are 2 types of immune system response to pathogens? |
Innate immune system (non-specific defence mechanism) Adaptive immune system (specific defence mechanism) |
|
|
what are lymph glands? |
specialized organs that contain a high density of cells involved in conferring immunity |
|
|
What is an antigen? give examples |
Any macromolecule, cell or organism that triggers an immune response against itself, if it gets into the body of a host animal. Bacteria, toxins from bacteria and other macromolecules |
|
|
What seems to be the only thing that antigens have in common? What does this give them? |
Antigens all seem to be of a certain size beyond a certain threshold. If they are too small, they must first bind with a protein to make them larger. antigenicity (the ability to act as an antigen) |
|
|
Explain antigen specificity, and subsequently, what is the importance of this? |
The immune system is able to recognise EVERY unique antigen with extreme precision. This allows the immune system to ignore cells that aren't considered antigens, giving the property of immunological tolerance. |
|
|
Name the 3 main lineages of leukocytes. Where do these originate from? |
Lymphoid cells Granulocytes Monocytes These cells derive from the same set of undifferentiated stem cells found in the marrow that produce erythrocytes. Haematopoietic stem cells |
|

|
A - Small lymphocytes (A1 = T Cell, A2 = B Cell) B - Large granular lymphocytes C - Neutrophils D - Basophils & mast cells E - Eosinophils F - Marcophages G - Innate immunity H - Adaptive immunity |
|
|
Outline the 5 methods of innate immunity |
· Defence at body surfaces · Constituent antimicrobial chemicals · Phagocytosis · Cytotoxicity · Inflammation |
|
|
Examples of defence at body surface |
Skin - barrier Sweat - acid Respiratory tracts - cilia and mucous Tears & saliva - lysozome Stomach - acid |
|
|
What is an example of a chemical barrier? How does it work? |
Lysozome, attacks specific sugars only present on bacterial cell walls, damaging the integrity of cell |
|
|
What is a complement |
a collection of approx 20 proteins which rely on cascade reaction. Initially are inactive, but activated by specific trigger. This first series activates second series etc until last member is activated, scaling up each time. Final component is a cylindical protein called membrane attack complex, punching holes in pathogen membrane causing fluid to enter (osmosis) and bursting cell |
|
|
What are Interferons |
Primarily used to tackle viruses. Interferons damage viral mRNA and inhibit protein translation, not only in the infected cell, but also in neighbouring uninfected cells. |
|
|
In relation to biological dye, how do the following cells stain? A) Neutophrils B) Eosinophils C) Mast cells & basophils |
A) Doesn't stain B) Acid dyes C) Alkali dyes |
|
|
Explain role of granulocytes |
"granular" appearance = chemicals that either damage cells directly or attract or activate other components of immune system |
|
|
The immune responses mediated by leukocytes can be thought of as having what three kinds of defensive activity |
1) phagocytosis, 2) cytotoxicity, i.e. killing infectious organisms by damaging the cell membrane of a pathogen or an infected host cell; 3) generating inflammation around the site of an infection. |
|
|
What do monocytes do? |
Differentiate to macrophages - "big eater" =phagocytes |
|
|
What do NK cells target? |
NK cells are particularly effective against virus-infected cells. |
|
|
What are opsonins? What do they enable? |
certain antibodies, components of the complement cascade and other specialized proteins in the bloodstream bind to many types of pathogen and label them as targets for phagocytosis. |
|
|
Explain structure of binding sites of opsinons |
Opsonins have two different kinds of binding site in their structure one site binds to the pathogen and the other binds to specialized receptors on the surface of the phagocytic cell |
|
|
Explain the process of "opsonization" |
The labelling of pathogens or other targets with proteins that promote phagocytosis is known as opsonization |
|
|
How do NK cells locate and destroy targets? |
NK cells have receptors in their surface membrane that bind to viral glycoproteins; these appear on the surface of infected body cells as new virus particles are constructed inside them. The NK cell releases perforin, a cylindrical molecule to perforate cell membrane, allowing fluid to enter, bursting the cell |
|
|
What causes inflammation? |
the inflammatory response can be initiated by the unique sugar units and glycoproteins found in many bacterial cell walls. These bacterial molecules cause activation of the components of complement, which are pre-formed in many body fluids and are powerful promoters of inflammation |
|
|
How do complement cause inflammation? |
they attract leukocytes to the area (a process called chemotaxis) and trigger them into degranulating, releasing the contents of their granules which contain some chemicals with a wide range of effects on blood vessels and tissues including inflammation. |
|
|
What happens during an allergic reaction? |
Antibody IgE simultaneously binds to allergen and to mast cells, triggering granulation which also releases histamine. |
|
|
What is suppuration? |
An infected and inflamed wound often forms pus; supparation is the process behind it |
|
|
What is in pus? (6) |
dead phagocytes dead cells, cell debris, fibrin (a protein involved in blood clotting), plasma living and dead microbes |
|
|
What causes pyrexia? |
Chemicals called pyrogens - e.g. interleukin-1 from damaged tissue and the cells involved in the inflammatory response and act on the hypothalamus |
|
|
The function of an increased body temperature? |
Increases the metabolic rate of the cells in the inflamed area and, consequently, there is an increased need for oxygen and nutrients. The increased temperature promotes the activity of phagocytes. |
|
|
Deep-seated abscesses on the other hand have a variety of outcomes (5). |
-rupture completely on skin and heal -rupture partially, chronically infected with open channel (sinus) -Rupture, discharging in to adjacent organ or cavity forming an infected channel (fistula) -Pus removed by phagoctyes and heals -Pus enclosed by fibrous tissue and calcifies. Can be potentially survive and source for future infection |
|
|
What happens to tissue during chronic inflammation |
Can become damaged/destroyed. Furthermore, fibroblasts are activated which lay down collagen and fibrosis occurs leading to formation of scar tissue. |
|
|
If the body's defence are unable to clear infection, how else might it try and cope? |
may try to wall it off instead, forming nodules called granulomas, within which are collections of defensive cells. Tuberculosis is an example of an infection that frequently becomes chronic, leading to granuloma formation and is difficult to treat. |
|
|
What happens when a certain kind of pathogen enters the body for the first time? How about a second time? How do these events differ? |
A primary adaptive response occurs initially. Then Secondary adaptive response.
The primary response takes up to 7-10 days to manifest and peaks within 3 weeks. Patient is likely to feel symptoms. Secondary response develops sooner, lasts longer and the extent of the response is greater, symptoms are less to none-existantq |
|
|
What aspect of the pathogen is remembered in relation to immunological memory? |
The eptiope |
|
|
In the adaptive immunity, what cells bind to antigen? |
Small lymphocytes cell surface receptors |
|
|
How do the innate and adaptive immunity differ in relation to epitope recognition |
Innate immunity - leukocytes only recognise the few tens of receptors (sugars on cell surface) Adaptive immunity - small lymphocytes recognise millions of types, although each small lymphocyte can make just one of these |
|
|
What are epitopes? |
The immune system being able to identify and attack all of the non-self clusters that occur only in the structures of pathogens or their harmful products (toxins), and which therefore act as unique signatures for these threats to life. Epitopes are indicators that the whole of the cell or macromolecule on which they occur is both non-self and a legitimate target for an immune response. |
|
|
How do lymphocytes initially detect these epitopes? |
Each lymphocyte can manufacture one specific receptor which can bind to their complementary epitope. So if an antigen is present, there must be a few lymphocytes already in body which can bind to one of the epitopes. These lymphocytes are said to be members of the same clone. With a population of billions of lymphocytes, these consist of approx 100 mn clones - between all of these they have sufficient antigen receptor diversity to bind to all epitopes which will be encountered in a lifetime. Basically, our immune system is pre-programmed to be able to react to every potential antigenic epitope. |
|
|
3 important functions of lymphatic system |
1) To defend the body against invading organisms by means of the immune system. 2) To collect and return interstitial fluid (the fluid between the cells) to the blood. 3) To absorb lipids from the digestive tract. |
|
|
What happens at lymph nodes? |
Lymph from lymph vessels pass through them and filters any pathogens. Here they are inactivated by cells of the immune system |
|
|
What is a colloidal osmostic pressure? |
When proteins are too large to pass through capillary to interstitial fluid, they form colloidal osmotic pressure, drawing interstitial fluid back to capillaries |
|
|
What causes the formation of interstitial fluid? |
Formed as a result of a net loss of fluid from the capillaries as blood passes through the capillary network via passive diffusion. In addition to passive diffusion, the blood pressure within the capillaries forces fluid out through the wall |
|
|
Why are B and T lymphocytes called B & T? |
B = mature in bone marrow T = mature in thymus |
|
|
What role do B cells do in regards to immune response? |
Create antibodies, proteins which bind to, and destroy, antigens.
|
|
|
What hormone is released to promote the formation of fully differentiated and functional T lympocytes? |
Thymosin |
|
|
What roles do T cells do in regards to immune response? |
-Regulatory roles affecting both adaptive and innate response -Sustaining prolonged inflammation -Kill hosts own infected body cells |
|
|
What is the name of the process which is undertaken to proliferate the correct B & T cells when the epitope has been initiailly identified? |
Clonal expansion |
|
|
What happens when some of the defensive cells have destroyed the antigen? |
Most die, so levels in circulation reduce as amount of pathogen reduces, but some differentiate to memory cells which circulate for long periods of time. |
|
|
What do memory cells do? |
They carry the same antigen receptors as the original clone, so they permanently enlarge the clone of small lymphocytes capable of recognizing the initial epitope . This enlarged clone is able to respond much more rapidly by clonal expansion if the same epitope is encountered again - providing the basis for secondary response & immunological memory |
|
|
What are the 2 subsets T cells are split into? |
Cytoxic Helper |
|
|
What do cytoxic T cells do? |
use toxic and perforating chemicals to kill the body’s own cells when they have become infected with intracellular pathogens |
|
|
What are cytokines in relation to T helper cells |
Cytokines are produced by T cells and act as a signalling molecule and act in a paracrine fashion with a short life before breaking down to their constituent amino acids. They activate other luekocytes of innate immune response |
|
|
How does the T-cell antigen receptor differ, and how does it bind with epitopes? |
The antigen receptor consists of 2 poylpeptide chains that for a binding site for a specific epitope. However, close to this site are other polypeptides which restrict bind of epitope unless it is is being presented to the T cell by one of the hosts own cells!! |
|
|
So if helper T cells can only bind to epitopes that are presented by the hosts own cells, what types of cells can do this? And what are the collectively referred to as? |
Other luekocytes, including B cells and all phagocytic cell (macrophages). These are called antigen-presenting cells or APC's. |
|
|
What function do the APC's do? |
The bind to epitope and therefore antigen, phagocytose them and break them down in the cell using lysozomes. However, antigen fragments, including epitopes, are transported to cell surface where they are displayed in a molecule called MHC molecule. |
|
|
How do cytoxic T cells process their antigens? |
Epitopes of pathogen reach surface of the infected cell when pathogens die, and some fragments end up in clefts of MHC molecules on infected cells surface. The cytoxic T cells bind to these to trigger antigen |
|
|
How do T cells recognised "self" molecules, and due to this mechanism, what are T cells referred to as? |
The arrangement of MHC molecules are unique to each host so they only kill INFECTED SELF CELLS - a double lock mechanism as an analogy. They are subsequently referred to as self-MHC restricted |
|
|
What advantage can you see in the evolution of helper T cells which are restricted to recognizing self-MHC plus epitope?
|
Self-MHC restriction limits each helper T cell to interacting only with those leukocytes in the immune system that have already bound to the epitope for which the T cell also has antigen receptors.
|
|
|
What advantage can you see in the evolution of cytotoxic T cells which are restricted to recognizing self-MHC plus epitope |
Self-MHC restriction ensures that cytotoxic T cells can only kill self cells that are harbouring intracellular pathogens. |
|
|
What are MHC cells? |
Major hisocompatabilty complex are self markers, i.e. these are the properties that can either accept or reject a transplanted organ. |
|
|
Where are B lymphocytes found? |
Fixed in lymphatic tissue, spleen and lymph nodes |
|
|
Difference between epitope recognition with B and T cells? |
B Cells don't need to have them presented on the hosts cell via MHC molecule. These are referred to as native antigens as opposed to processed antigens. |
|
|
What happens to B cells after contact with epitope? |
After contact with antigen they undergo clonal expansion and differentiate either into memory B cells, or into a type of defensive cell called plasma cells which secrete antibodies |
|
|
What are the antigen receptors on all B cells are known as? |
surface immunoglobulins |
|
|
What does the B cell do when they bind with these surface immunoglobulins? |
**causes the original B cell to divide and differentiate into an expanded clone of memory B cells and plasma cells. Produces antibodies that are almost identical to surface immunoglobulin molecules that bound to epitope ** note, other activating signals also stimulate B cell to do this, such as helper T cell |
|
|
What are the 5 classifications of antibodies, and how are they referred to as? |
G - IgG A - IgA M - IgM D - IgD E - IgE Ig = immunolgobulin |
|
|
Significance of ordering of the types of antibodies? |
G, A, M, D & E in order of abundance in bloodstream with G being most abundant. |
|
|
Elaborate on IgG anitbodies |
The most abundant antibody class found in the bloodstream, but not produced in significant quantities until secondary adaptive immune response Also trigger complement cascade when 2 or more inactive complement components |
|
|
Significance of IgG in pregnancy |
IgG antibodies are the only class which can pass through the blood vessels of the placenta and so transfer passive immunity from mother to unborn baby. |
|
|
What does IgM do? |
Form pentamers, increasing effectiveness of the the few available antibodies during primary response. They clump together - easier targets for innate immune system. Also powerful activators of complement cascade (more than IgG) |
|
|
What does IgA do? |
Can reach the inner surfaces of the respiratory system (including the nose and mouth), the gut and the urinary and genital tracts. Most pathogens get into the body in the air we breathe, in the food and water we consume, and during sexual intercourse Also plays a key role in the transfer of passive immunity from mother to new-born baby |
|
|
What does IgE do? |
They have binding sites for epitopes found on common pathogens, including the larger multicellular parasites such as worms. The tail section of these attached to mast cells which result in inflammation. |
|
|
What happens if people who synthesise excess IgE antibodies in response to harmless particles, such as pollen? |
Mass degranulation - anaphylaxis! Especially if inhaled (such as pollen) causes airway compromise |
|
|
How are we "self tolerant"? |
Early in fetal life, when millions of different antigen-receptor shapes are being randomly generated as new lymphocyte clones are formed from the multipotent stem cells, a rigorous process of selection occurs in which self-reactive clones are weeded out and destroyed. This process is called clonal deletion. |
|
|
Elaborate on Clonal deletion |
Specialized cells within the thymus present self epitopes on their surface membranes and, as the juvenile T cells pass through, any with antigen receptors that bind to the self epitopes are given a chemical signal which causes them to undergo apoptosis.. So only T cells that do not bind to self epitopes proliferate! |
|
|
The mechanisms of self-tolerance inolve the deletion of self-reactive T cells. Clonal deletion is thought to have a relatively minor role in maintaining self-tolerance among the B cells; So why don't B cells react to self tissue? |
The helper T cells don't provide the response (cytokines) to mount an immune response against the self epitopes |
|
|
What happens if self-reacting B cells become active in later life? What diseases is this? |
new clones of self-reactive helper T cells are generated randomly and a few may slip through the net and survive the deletion process - so may trigger B cells. Also self-reactive cytoxic T cells may also occur - causing autoimmune disease |
|
|
What is active immunity? (2 points) |
Immune through previous infection or immunisation |
|
|
What is passive immunity? (2 points) |
The fetus passively acquires some of the antibodies actively produced by the mother in response to infections she has encountered via the placenta The new-born baby who is breast-fed also passively acquires some maternal antibodies in the colostrum |