![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
87 Cards in this Set
- Front
- Back
|
Right upper quadrant |
Ascending & transverse colon Duodenum Gallbladder Hepatic flexure of colon Liver Pancreas (head) Pylorus (the small bowel—or ileum— traverses all quadrants Right adrenal gland Right kidney (upper pole) Right ureter |
|
|
Right lower quadrant |
Appendix Ascending colon Cecum Right kidney (lower pole) Right ovary and tube Right ureter Right spermatic cord |
|
|
Left upper quadrant |
Left adrenal gland Left kidney (upper pole) Left ureter Pancreas (body and tail) Spleen Splenic flexure of colon Stomach Transverse descending colon |
|
|
Left lower quadrant |
Left kidney (lower pole) Left ovary and tube Left ureter Left spermatic cord Descending and sigmoid colon Bladder Uterus Prostate gland |
|
|
Peritonium |
thin, shiny, serous membrane called |
|
|
Solid viscera |
Liver, pancreas, spleen, kidney, ovaries |
|
|
Hollow viscera |
Stomach, small and large intestines, gallbladder |
|
|
Pyrosis |
Heartburn |
|
|
Eructation |
Belching or burping |
|
|
Flatulence |
Passing rectal gas |
|
|
Emesis |
Nausea or vomitting |
|
|
Anorexia |
Loss of appetite |
|
|
Dysphagia |
Difficulty in swallowing |
|
|
Constipation |
Difficulty in defecation |
|
|
Visceral pain |
occurs when hollow abdominal organs such as the intestines become distended or contract forcefully |
|
|
Visceral pain |
Poorly defined or localized and intermittently timed, this type of pain is often characterized as dull, aching, burning, cramping, or colicky. |
|
|
Parietal pain |
occurs when the parietal peritoneum becomes inflamed, as in appendicitis or peritonitis. This type of pain tends to localize more to the source and is characterized as a more severe and steady pain. |
|
|
Reffered pain |
occurs at distant sites that are innervated at approximately the same levels as the disrupted abdominal organ. This type of pain travels, or refers, from the primary site and becomes highly localized at the distant site. |
|
|
Striae |
Stretchmarks |
|
|
periumbilical ecchymosis |
Hemorrhagic discoloration |
|
|
flank ecchymosis |
Discoloration of the left flank |
|
|
Caput medusae |
Outward flow pattern from umbilicus in all directions. Cardinal sign of portal hypertension. |
|
|
Ascites |
is the build up of fluid in the space between the lining of the abdomen and abdominal organs, often due to severe liver disease. |
|
|
Umbilical hernia |
an abnormal bulge into the abdominal wall that can be seen or felt near the umbilicus (belly button). |
|
|
Borborygmus |
loud, prolonged gurgles characteristic of one’s “stomach growling |
|
|
Aneurysm |
Loud bruits detected over the aorta may indicate presence of |
|
|
Peritoneal friction rub |
rough grating sound like sound of two pieces of leather being rubbed together |
|
|
Rebound tenderness |
palpating deeply at 90 degrees into the abdomen away from the painful or tender area. |
|
|
Psoas sign |
lie on the left side. Hyperextend the right leg of the client. |
|
|
Obturator sign |
Support the client’s right knee and ankle. Flex the hip and knee, and rotate the leg internally and externally. |
|
|
Hepatomegaly |
is enlargement of the liver beyond its normal size. |
|
|
Splenomegaly |
is defined as enlargement of the spleen measured by size or weight. |
|
|
Appendicitis |
is an inflammation of the appendix, a finger-shaped pouch that projects from your colon on the lower right side of your abdomen. A positive result in Psoas and Obturator sign. |
|
|
Murphy sign |
pain elicited when pressure is applied under the liver border at the right costal margin and client inhales deeply Cause – inflammation of the gallbladder |
|
|
Rovsing sign |
pain in the RLQ during pressure in the LLQ Cause – acute appendicitis |
|
|
Blumberg sign |
abdominal pain or tenderness experienced when examiner test for rebound tenderness byu palpating deeply at 90 degrees into the abdomen one-halfway between the umbilicus and the anterior iliac crest cause – peritoneal irritation |
|
|
Periosteum |
covers the bones |
|
|
Tendons |
Skeletal muscles attach to bones by way of strong, fibrous cords called |
|
|
Joint |
The junction of two or more bones is called |
|
|
Non synovial joint |
the bones are connected by fibrous tissue, or cartilage. The bones may be immovable, like the sutures of the skull, or slightly movable, like the vertebrae. |
|
|
Synovial joint |
move freely; the bones are separate from each other and meet in a cavity filled with synovial fluid, a lubricant. These joints are surrounded by a fibrous capsule that stabilizes the joint structure and surrounds the joint’s ligaments- the tough, fibrous bands that join one bone to another. |
|
|
Bursae |
are small sacs filled with synovial fluid that serve to cushion the joint |
|
|
Ball and socket joint |
located in the shoulder and hips allow flexion, extension, adduction and abduction rotates in their sockets are assessed by their degree of internal and external rotation |
|
|
Hinge joint |
include the knee elbow move in flexion and extension |
|
|
Carpal Tunnel Syndrome |
What is CTS |
|
|
Tinel's sign |
Lightly percuss the transverse carpal ligament over the median nerve where the patient’s palm and wrist meet. |
|
|
Phalen's maneuver |
Have the client put the back of his hands together and flex his wrists downward at a 90 degree angle |
|
|
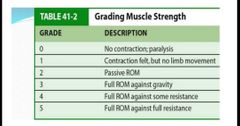
Grade 2 in grading muscle strength |
|
|
Quadriceps strength |
lower legs and raise then again while you press down on his anterior thigh |
|
|
Ankle strength |
patient push his foot down against your resistance and then pull his foot up as you try to hold it down |
|
|
Foot drop |
result from weakness or paralysis of the dorsiflexor muscle of the foot and ankle, may also stem from prolonged immobility |
|
|
Crepitus |
abnormal crunching or grating when a joint with roughened articular surfaces move. Ex. Rheumatoid arthritis |
|
|
Muscle spasm |
cramps, strong, painful contraction, common in calf and foot |
|
|
Muscle atrophy |
muscle wasting, results from prolonged muscle disuse |
|
|
Traumatic injury |
fractures, dislocations, amputations, crush injuries, serious lacerations |
|
|
Pain Paresthesia Paralysis Pallor Pulse |
5 P’s of Musculoskeletal Injury |
|
|
Paresthesia |
assess for loss of sensation by touching the injured area with the tip of an open safety pin. Abnormal sensation or loss may indicate neurologic vascular involvement |
|
|
Aorta Left and right renal artery Left and right iliac artery Left and right femoral artery |
If arterial insufficiency is found in legs, auscultate over the following areas: |
|
|
Venous |

|
|
|
Arterial |

|
|
|
Arterial |
Location of sores: toes and feet |
|
|
Venous |
Location of sores: ankles |
|
|
Manual compression test |
To check for competency of valves |
|
|
Arterial circulation |
Bilateral/unilateral pulses weak, asymmetrical, or absent may indicate |
|
|
Doralis pedis pulse |
Have client dorsiflex or extend foot. |
|
|
Posterior tibial pulse |
located on medial malleolus of ankle |
|
|
Superficial vein thrombophlebitis |
is characterized by redness, thickening, and tenderness along the vein. |
|
|
Occluded artery |
Bilateral/unilateral pulses weak, asymmetrical, or absent may indicate |
|
|
Arterial insufficiency |
Pallor, cyanosis, rubor; pallor on elevation and rubor on dependency suggest |
|
|
Venous insufficiency |
rusty or brownish pigmentation around ankles indicates |
|
|
Arterial insufficiency |
Cold; coolness in one leg suggest |
|
|
Thrombophlebitis |
increased warmth in leg may be due to |
|
|
Raynaud's disease |
Disorder caused by vasoconstriction or vasospasm of the fingers and toes |
|
|
Hyperkinesis |
Increase radial pulse may indicate |
|
|
Pulse inequality |
may indicate arterial constriction or occlusion in one carotid |
|
|
Weak pulses |
occur with hypovolemia, shock, or deceased cardiac output. |
|
|
Arteriosclerosis |
Loss of elasticity may indicate |
|
|
Allen's test |
used to detect arterial insufficiency of the hand. |
|
|
Arterial peripheral vascular disease |
tobacco smoking, age over 50 years, family history of peripheral vascular disease, hypertension, coronary or peripheral vascular disease, or male sex. |
|
|
Venous peripheral vascular disease |
pregnancy, job with prolonged standing, limited physical activity/poor physical fitness, congenital or acquired vein wall weakness, female sex, increasing age, genetics (eg. Non-African American), obesity, lack of dietary fiber, use of constricting corsets/clothes. |
|
|
Epitrochlear nodes and superficial inguinal nodes |
superficial lymph nodes of the arms and legs |
|
|
Epitrochlear nodes |
located approximately 3 cm above the elbow on the inner (medial) aspect of the arm which drain the lower arm and hand |
|
|
Superficial inguinal nodes |
consist of two groups: a horizontal and a vertical chain of nodes. The horizontal chain is located on the anterior thigh just under the inguinal ligament, and the vertical chain is located close to the great saphenous vein. These nodes drain the legs, external genitalia, and lower abdomen and buttocks |
|
|
Capillary bed |
is very important in maintaining the equilibrium of interstitial fluid and preventing edema |
|
|
Venous stasis |
long periods of standing still, sitting or lying down. Lack of muscular activity causes blood to pool the legs which in turn increases pressure in the vein. |
|
|
Femoral vein and popliteal vein |
2 deep veins |
|
|
Jansjs |
Baba |