Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
132 Cards in this Set
- Front
- Back
|
|
|
|

|
|
|
|
|

|

|
|
|

|
|
|
|
|
|
|
|

|
|
|

|
|
|

|
|
|

|

|
|

|

|
|
|
|
|
|

|
|

|

|
|

|
|
|

|

|
|

|

|
|

|

|
|
|
|
|

|

|
|

|

|
|

|

|
|

|
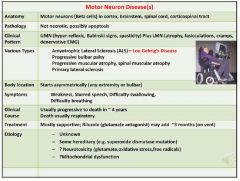
Motor neuron disease causes a combination of upper and lower motor neuron findings.
|
|

|

|
|

Steroids DO work for the chronic type.
|

|
|

|
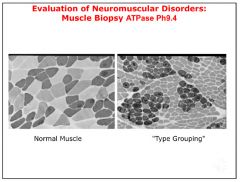
Fiber type grouping is indicative of axonal loss.
|
|

|

|
|

|

|
|

|
|
|

|

The top graph represents MG.
|
|

In LE syndrome, the response gets bigger with repeated stimulations.
|

|
|

|

|
|

|
|
|

|
|
|

|

|
|

|

|
|
|

|
|

|

|
|
|

|
|

|

|
|

|

|
|
|
|
|

|

|
|

|

|
|
|

|
|
|
|
|

|

|
|
|

|
|
|

|
|

|

|
|

|

|
|

|

|
|

|
|
|
|

|
|

|

|
|

|
|
|

|

|
|

|

|
|
|

|
|

|

|
|

|

|
|
|

|
|

|
|
|

|

|
|

|

|
|

|

|
|

|
|
|

|

|
|

|

|
|

|

|
|

|

|
|
|
Epidural cord compression:
|

|
|

|

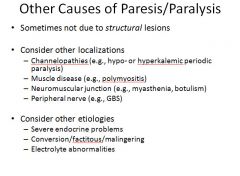
This diagram shows all the possible sites that would cause a problem with weakness.
|
|

|

3 things affect the NMJ: Botulism, Lambert-Eaton and Myasthenia Gravis.
|
|

|

|
|

|

|
|

Motor areas are mainly supplied by the middle cerebral artery.
|

The small portion of the fibers that do not cross after the decussation are responsible for motor control of the trunk.
|
|
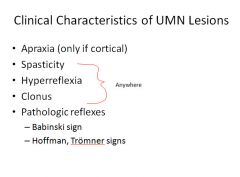
Babinski sign can be a normal finding up till 12 months of age.
Hoffman sign: flicking downward of the middle digit of the fingers; normal is no response, abnormal is twitching of the other fingers Tromner: flicking upward of the middle digit of the fingers; same as for Hoffman |

|
|

|

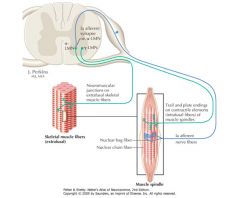
Gamma-motor neurons are responsible for “tightening” up the intrafusal muscle fiber to keep the spindle stretched; this allows for continued feedback and determination of load. All of these reactions are controlled by the cortex and basal ganglia. When the “higher” input is removed, this causes the gamma-motor neurons to go crazy and this leads to spasticity. This is why an UMN lesion leads to spastic reflexes.
|
|
|

0: No movement at all
1: flicker of movement only 2: movement with gravity eliminated 3: strength against gravity only 4: some strength against resistance 5: full strength against resistance |
|
|

Cerebral palsy: the patient has some kind of muscle problem…caused by an UMN problem and not congenital.
|
|

|

A subthalamic nucleus infarct = hemiballismus
|
|

|

|
|

|

|
|

Bromocriptine is a dopamine agonist; not an antagonist!!!
|

|
|

* The thought is that the abnormal cytoskeletal proteins responsible for RBC acanthocytosis are shared in some of the neurons, leading to abnormal neuron morphology/function.
|

|
|

Bradykinesia = slowed movement
|
|
|

|

|
|
|

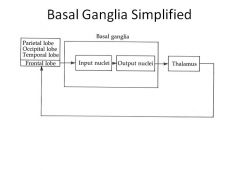
The sensory receptors are golgi tendon organs, intrafusal fibers and other primary sensory apparatus. Reflexes mediated by the spinal cord can result in non-conscious motor responses.
|
|
|

There is both unconscious and conscious monitoring of the executed movement.
|
|

THE RELATIONSHIP BETWEEN ACh and DA is especially important. Dopamine and Ach are in balance in the normal brain.
|

|
|

|

Since the indirect pathway is inhibitory, if you release the inhibition, you get excess movement.
|
|

|

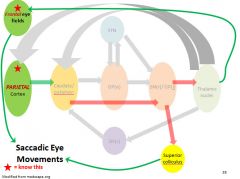
Saccadic eye movements originate in the frontal eye fields.
The parietal lobe is responsible for smooth tracking eye movements. |
|
|

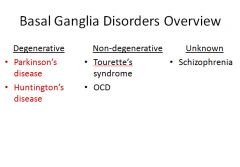
Classic example is Tourette’s syndrome.
|
|

|
|
|

|

|
|
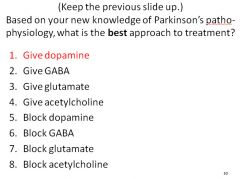
Give dopamine; but you can’t, so instead you have to correct the imbalance between Ach and Dopamine by blocking Ach instead by giving an anti-cholinergic drug. (Benadryl)
|

Treatment 1: combination of Carbidopa and Levodopa
Treatment 2: administration of a dopamine agonist; Ropinirole or Pramipexole Treatment 3: inhibition of the enzyme (COMT) that cleaves dopamine off the receptor Treatment 4: inhibition of dopamine reuptake and further metabolism; a monoamine oxidase inhibitor-B (MAOBI) (this actually doesn’t work well) Treatment 5: administration of an anti-cholinergic drug. * Carbadopa binds to the enzymes that metabolize dopamine to other products that cause undesirable side effects. |
|

|

|
|

|
|
|

|
|
|

|

|
|

|

|
|
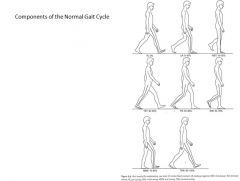
From the point where the leading heel first strikes the surface to the next time it strikes the surface is one gait cycle.
There are 5 points in the gait cycle where the body is balanced on one leg. |

|
|

|

These patients have problems with the sensory inputs.
|
|
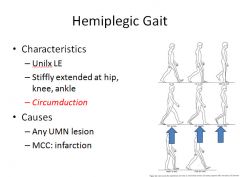
Circumduction: walking with stiff leg, has to “throw” the bad leg out in front with the hip muscles to continue walking.
|

|
|

Patients with Parkinson’s are off balance; to prevent from falling backwards they lean forward a bit, lower their center of gravity and take small steps.
|

Usually unilateral and caused by foot drop (can’t dorsiflex the foot); have to lift the leg up further to allow the foot to clear the ground.
|
|

In muscle disease, proximal weakness is greater than distal weakness.
Excessive movement of hips from side to side. |

So this type of gait is not abnormal….it is always caused by a psychiatric disorder of some type.
|
|

|

|
|

|

|
|

|
|
|

|

|
|
|

|
|
|

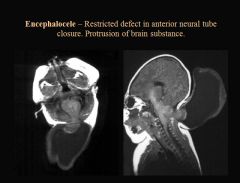
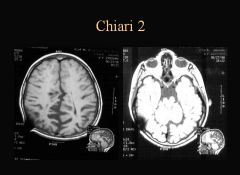
High alpha-fetoprotein levels correlate to congenital brain and spine malformation.
The higher the lesion is, the less likely the child is to walk. In utero closure of the lesion provides a better outcome; but carries a higher chance of miscarriage. |
|

Patient may be symptomatic or not; it depends on whether there is compression of the brain stem and flow of CSF
|

|
|
|

|
|

|

|
|

|

Bifid Cord; two spinal cords
|
|

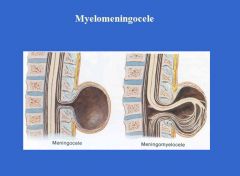
The spinal cord is stretched all the way down.
Walking and gait may be affected as the child grows. May develop urinary and bowel incontinence. |

|
|

|

|
|

|

|
|

|

|
|

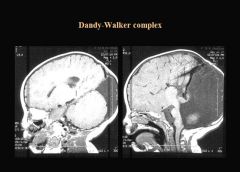
A normal finding in a pre-term child.
|

|
|

Children with small Dandy-Walker malformations may have problems with hydrocephalus later on in life.
|
|
|

|

Some kids with microencephaly are not mentally retarded.
|
|

|
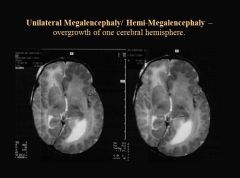
Kids with this problem have hard to control seizures. They often have a hemispherectomy to correct this.
|
|

Patients may have mild cerebral palsy and some seizures; but most will also have normal cognitive function.
|
More common in boys
|
|

|

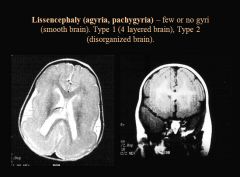
Fewer gyri than normal
|
|
|

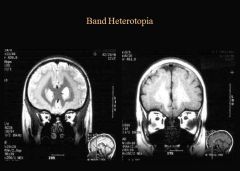
Double cortex; more common in girls
|
|

|

Hemangiomatosis of the brain and port wine stain
|
|

|

Ash leaf spots and seizures.
|
|
|
Tuberous Sclerosis:
|

|