Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
40 Cards in this Set
- Front
- Back
|
What is the Respiratory Circulatory Model?
|
A model that looks at the influence of myofascial and articular distortions on the respiratory and circulatory health of the patient. Originated by Dr. Gordan Zink in 1973.
|
|
|
What is the treatment emphasis of the respiratory circulatory model?
|
It is to reduce the work of breathing (increase the efficiency with each breath) and enhance the pumping action of the musculoskeletal system to bring venous and lymphatic flow back to the heart.
|
|
|
What does passive congestion of the venous and lymphatic systems lead to?
|
A build-up of waste products of cellular respiration, which leads to a compromise of the normal cellular environment and therefore suboptimal self-healing capacity.
|
|
|
Why is it important to have transitional areas and diaphragms in optimum condition?
|
They are required for optimal low pressure fluid movement (venous and lymph) via pressure changes generated in the mechanical process of breathing.
|
|
|
List the "transitional areas" and their "diaphragmatic areas" involved in generating pressure differentials.
|
Occipitoatlantal-Tentorium cerebelli
Cervicothoracic-Thoracic inlet Thoracolumbar-Thoracoabdominal diaphragm Lumbosacral-Urogenital pelvic diaphragm |
|
|
What happens when the thoracoabdominal "cylinder" or any of the diaphragms is distorted?
|
The diaphragmatic amplitude is decreased and therefore pressure gradients are decreased. This reduces gas and fluid movement throughout the body, not just the core.
|
|
|
List different pumps of the body involved in maintaining the respiratory and circulatory systems.
|
The heart is a force pump.
The thoracoabdominal cage with the action of the thoracoabdominal diaphragm operates as a suction pump for secondary respiration and drives venous and lymphatic return to the heart. The brain along with the reciprocal tension membrane system operates as a cerebrospinal fluid pump. The digestive system operates as an extraction pump. The urogenital/pelvic diaphragm maintains the lower end of the intraabdominal pressure differential and assists in the movement of fluids from the lower extremities. The musculoskeletal contraction system augments fluid return to the body core in addition to providing body movement. |
|
|
Points on posture and function.
|
- Ideal posture is a more energy efficient orientation.
- Proper muscle length and tension are necessary for maintenance of body functions for ambulation, respiration, digestion, and other functions. - Blood flow is inextricably linked with neural function and metabolic activities. - Proper joint surface apposition is necessary to maintain the Proper relationship to all myofascial structures. - muscle inhibition may also occur when there is misalignment of joint surface position, inflammation or if joint fluid pressures are elevated. |
|
|
What are benefits for a supine evaluation?
|
Patient should be able to relax entire body toward physiologic ideal.
The supine position reveals patterns that are associated with compromise to the respiratory and circulatory systems. |
|
|
What may be seen from a supine evaluation?
|
Fascial twist patterns, altered breathing patterns, tissue edema and bogginess and postural compromise can be more easily recognized.
|
|
|
What does venous drainage of the central nervous system depend on?
|
Venous drainage of the CNS (cranial) is valve less; emptying is passive and depends on the proper respiratory effort and negative intrathoracic pressure to serve as a "suction" pump for this flow.
|
|
|
Describe tentorium cerebelli and falx cerebri and their significance.
|
This diaphragm is contained in the cranium. It is also linked to the sacrum via the dura and influenced throughout the vertebral and pelvic system.
Restrictions in the dural and arachnoid membranes via strains to the reciprocal tension membrane affect the circulation of the cerebrospinal fluid and the transit of nerves and blood vessels as they course through these membranes. |
|
|
What will happen to the cerebrospinal fluid if the jugular veins are restricted?
|
Cerebrospinal fluid pressure will increase.
|
|
|
List the tennets of the Primary Respiratory Mechanism.
|
- Inherent motility of the central nervous system
- Mobility of the intracranial and intraspinal membranes (Reciprocal Tension Membrane) - Fluctuation of the cerebrospinal fluid (CSF) - Mobility of the cranial bones - Involuntary mobility of the sacrum between the ilia |
|
|
What is the Secondary Respiratory Mechanism?
|
Body core and the thoracoabdominal diaphragm.
|
|
|
What is the anatomical and functional thoracic inlet?
|
Anatomical Inlet: manubrium, 1st ribs bilaterally and T1
Functional Inlet: manubrium, first 2 ribs bilaterally and T1-4 |
|
|
What is the thoracic outlet?
|
Thoracic Outlet: clavicle, 1st ribs and scapula
|
|
|
What might edema at the supraclavicular region indicate?
|
Obstruction of terminal lymphatic drainage; the majority of lymphatic drainage terminates at the region fo the throacic inlet.
|
|
|
How will venous flow be affected when the thoracic inlet is obstructed?
|
Venous flow can be diverted through the azygous system and enter via the inferior vena cava but will place more back pressue on lower venous system.
|
|
|
List the attachments and openings of the thoracoabdominal diaphragm.
|
Attachments: Right crus to L1,2,3,(4); Left crus to L1,2,(3); Arcuate ligaments; Xyphoid process; Ribs 6-12.
Openings/penetrations: Esophageal hiatus; Vena caval foramen; Azygous/hemiazygous v.; Aortic foramen. |
|
|
What results from thoracoabdominal diaphragm dysfunction as a result of a hypertonic crura.
|
Contraction of the crura of the diaphragm places the thoracoabdominal diaphragm in a more caudal and flattened oriented (inhalation direction). With reduced excursion of the diaphram, the result will be increased venous congestion and reduced lymphatic drainage from the entire body.
|
|
|
How will someone be breathing who has a diaphram that will not relax fully?
|
The breathing pattern is more costal and less abdominal resulting in a higher rate and lower depth of respiratory effort.
|
|
|
Describe motion of the diaphragms and ribs during inhalation and exhalation.
|
During inhalation, all the diaphragms descend and flatten and the rib cage increases bucket-handle, pump-handle, and caliper rib motions.
During exhalation, all the diaphragms ascend, the abdominal diaphragm redomes, and the bucket handle, pump handle and caliper rib motions decrease. |
|
|
What are cisterna chyli?
|
Dilated sac at the lower end of the thoracic duct into which lymph from the intestinal trunk and two lumbar lymphatic trunks flow. They are at the level of L1-L2.
|
|
|
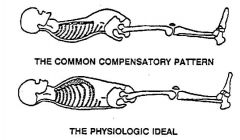
What are possible causes of fascial compensation patterns?
|
May be due to: The body’s response to postural stresses and gravity, in-utero torsions, Coriolis effect, handedness, viscerosomatic reflexes.
|
|
|
What is significant about uncompensated patterns?
|

They are a greater challenge to the physiologic state and are commonly the result of trauma.
|
|
|
Why does the body take on a compensatory pattern?
|
It is an adaptive response to attempt to maintain function but is not an ideal state of posture. It provides less than ideal metabolic function by reduing optimum respiratory and circulatory activities.
|
|
|
List the transitional areas of the body. Why are they significant.
|
Occipitoatlantal, cervicothoracic, thoracolumbar, and lumbosacral regions. Are regions with transitional changes in anatomical characteristics. Have the greatest motion and receive the greatest stress and strain among the other vertebral segments. Have venous plexuses in these regions. Are sites of crossover points for compensatory curves.
|
|
|
What are the steps in the respiratory/circulatory screen?
|
Respiratory movement (level and time phase ratio)
Lumbar spine curve (flat or #finger spaces) Leg length Iliac crest heights (LS sidebending) Pelvic rotation (LS rotation) ASIS position (pelvic position) Innominate rotation (SIJ restriction) Thoracolumbar rotation and translation Cervicothoracic rotation and translation Occipitoatlantal rotation and translation Shoulder position Arm length |
|
|
Describe respiratory movement step.
|
a) Respiratory movement along the anterior body core. How far down do you observe this movement: at the neck, rib cage, xyphoid, above or below the umbilicus or above or at the pubic symphysis. The best is abdominal all the way to the pubic symphysis. Worst is upper costal with excessive use of the accessory muscles of respiration at the neck.
b) Rate, ratio and depth of breathing. The inhalation to exhalation time phase ratio should be one inhalation to two or three exhalation. |
|
|
Describe lumbar spine curvature step.
|
Patient’s back should be flat to the table. If the patient maintains a space between the lumbar spine and the table, how many finger spaces is this measurement?
|
|
|
Describe leg length step.
|

Place the thumbs under the medial malleolus and compare the quality and length of the legs. Note the quality and quantity of this movement. Are both legs equal in length or is one longer than the other? In CCP, the left leg is longer than the right.
|
|
|
Describe lumbosacral transitional region step.
|
a) Place the hands over the cephalad part of the iliac crests bilaterally and note if one hand is more cephalad compared with the other. In CCP, left iliac crest is cephalad and represents left lumbosacral sidebending.
b) Place hands around lateral aspect of the hips. Rotate the pelvis to the right and left and compare rotation motion of each side. In CCP, the pelvis rotates easier to the right and therefore the lumbar is rotated right at the lumbosacral region. |
|
|
Describe pelvic girdle step.
|
a) Place the thumbs under the ASIS and compare the heights (cephalad/caudad). In CCP, the right ASIS is posterior and inferior.
b) With the palms over the ASIS and fingers around the lateral aspect of the ilia, press in a superior/lateral direction with one hand and pull in an inferior/medial direction with the other. In CCP, the left innominate moves easier with superior/lateral movement and the right innominate with inferior/medial movement. |
|
|
Describe thoracolumbar transitional region step.
|

Place hands around lateral aspect of the lower rib cage bilaterally. Rotate this region to the right and left. Next, translate (sidebend) this region. In CCP, the thoracolumbar region is rotated and sidebent to the left.
|
|
|
Describe cervicothoracic transitional region step.
|

Place hands over the top of the thoracic cage with the pads of the fingers over the clavicle in contact with the anterior 1st ribs and the thumbs in contact with the transverse processes of T1 and the remaining part of the hand in contact with the tissues between. Test rotation and sidebending (translation) motion. In CCP, this region is rotated and sidebent right.
|
|
|
Describe occipitocervical transitional region step.
|

Place hands gently around the base of the cranium at the occiput. Slightly flex the head and neck and test rotation and sidebending (translation) motion. In CCP, this region is rotated left and side-slipped the the left (resulting in sidebending to the right).
|
|
|
Describe shoulder position step.
|
Are the shoulders flat to the table or are they forward? How does this compare to your standing postural screen? Gently press the shoulder toward the table and see if you can detect resistance to posterior movement from overly tight anterior chest and shoulder muscles. Is one side more anterior and restricted compared with the other side?
|
|
|
Describe arm length step.
|

Gently abduct/flex each arm to compare the quality and length of the arms. Note the quality and quantity of this movement. In CCP, the right arm is longer than the left.
|
|
|
What areas are checked for passive congestion (edema or bogginess)?
|
i) Suboccipital area
ii) Supraclavicular area iii) Axillary fold iv) Epitrochlear area v) Inguinal region vi) Lateral thighs vii) Popliteal fossa viii) Achilles tendons |