Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
10 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
tardive dyskinesia
|
due to antipsychotics
is a variety of DYSTONIA (involuntary, repetitive movements) manifesting as a side effect of long-term or high-dose use of dopamine antagonists. tardive: the dyskinesia sometimes continues or appears even after the drugs are no longer taken |
|
|
|
chorea v. dystonia
|
dystonia are non-choreic rapid, patterned movements that repeat themselves in a set distribution of the body and do not have the changing, flowing nature of choreic movements that travel around the body.
|
|
|
|
Athetosis
|
continuous succession of slow, sinuous, writhing, involuntary movements especially of the fingers and is characteristic of basal ganglia lesions.
|
|
|
|
Decerebrate posturing
|
damage to lower midbrain or upper pons
both the upper and lower limbs are extended |
|
|
|
Decorticate posturing
|
damage to reticular formation in the upper midbrain. Upper limbs are flexed at the joints and lower limbs are in extension
|
|
|
|
Spinal Cord Syndromes:
Commissural Syndrome |
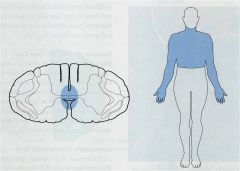
Lesion in the central region of SC.
segmental loss of p & temp sensation due to interruption of 2nd order axons as they decussate to form the spinothalamic tracts. Sensory loss is bilateral, and loss is only in those segments. |
|
|
|
Spinal Cord Syndrome
Intramedullary Lesion |
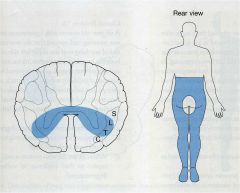
Sensory loss with sacral sparing due to the intramedullary lesion shown on the left, involving lateral spinothalamic tracts bilaterally.
loss of pain and temperature sensation at all levels below the lesion except in the sacral level |
|
|
|
Brown-Sequard Syndrome
|
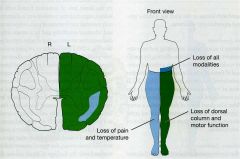
lateral hemisection of the spinal cord.
Severs the pyramidal tract (which has already crossed in the medulla),the uncrossed dorsal columns, and the crossed spinothalamic tract. The only time you will see this is due to trauma, i.e., knife or bullet |
ipsilateral and below the level of the lesion demonstrates UMN weakness (paralysis), loss of tactile discrimination, loss of position sense, and loss of vibratory sense. The ipsilateral DTRs become hyperactive with subsequent spasticity and a positive Babinski response develops.
Contralateral to the lesion there is a loss of pain and temperature sensation below the lesion |
|
|
Posterior Fossa
|
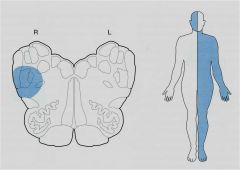
contralateral loss of sensory function in the trunk and limbs because of interruption of the major ascending pathways.
Sensory function (primarily pain and temperature) is also lost over the ipsilateral face because of segmental involvement of the trigeminal nerve or its descending tract and nucleus |
any lesion involved in the brainstem affects the ipsilateral cranial nerve and the fibers that travel to and from the contralateral body.
|
|
|
HMSN I = Charcot-Marie-Tooth (CMT type I)
|
Most common inherited neuropathy.
group of neuropathies which are characterized by their impact upon both afferent and efferent neural communication. |
|