Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
30 Cards in this Set
- Front
- Back
|
What is the broad category of disease that scleroderma falls under?
What two components must it fulfill? |
Collagen Vascular Disease
1. Collagen (excess/abnormal CT production) 2. Vascular anomalies |
|
|
What is the incidence of scleroderma? What demographic is typically affected?
|
Uncommon (2-12/ million/ year)
F>M (4:1). Mostly appears in middle age. |
|
|
What is localized scleroderma (comes in two forms)?
|
Localized Scleroderma= just a disease of skin, almost never becomes systemic.
1. morphea 2. linear scleroderma |
|

What type of systemic sclerosis does this individual have? What antibody is associated with this condition?
|
Diffuse Cutaneous systemic sclerosis (dc-SSc)-
Systemic disease: IPF, renal failure, mycoardial disease, diffuse GI. TRUNCAL and acral skin affected. Scl-70 positive (antibody to topoisomerase I). Rapidly progressive onset and sick patients :( |
|
|
How does limited cutaneous systemic sclerosis (Lc-SSc) differ from diffuse systemic sclerosis (dc-SSc)?
|
Limited- RP involvement for years, limited skin involvement, anti-CENTROMERE antibody. Insidious onset of PHTN (pulmonary hypertension).
Also, much better survival than dc-SSc |
|
|
What are some presenting symptoms in scleroderma?
|
- Raynaud's
- swelling of hand/feet and stiffness (can look arthritic) - tightening of skin (rapid onset, within few months) - consistutioal sxs or things related to organ involvement (GI, renal, etc.) |
|

What is the "Vascular Paradox" associated with SSc (Systemic Sclerosis, i.e. Scleroderma)?
|
Patients can have BOTH Vasoconstriction and Vasodilatation.
Vasoconstriction: Raynaud's, Digital ulcer Vasodilation: Telangiectasia, Nailfold capillary dilation |
|

Just by looking at this person, what diagnosis would you give them? What is the formal criteria for diagnosing this?
|
Raynaud's Phenomenon (red, white, and blue- erythema, pallor, cyanosis) in response to cold/stress. Episodic.
Formally- need to have episodic vasospastic color change, bilaterality, absence of gangrene, normal pulsations of arteries and symptoms LONGER THAN 2 YEARS! |
|
|
What is the prevalence of raynauds? Why is it different in men and women?
|
Women ~5%, men ~4%
Women have higher density of α-adrenergic receptor (increase under influence of E2). Vasoconstrict under sympathetic control. |
|
|
What two things regulate acral cutaneous blood flow?
|
1) AV shunts (controlled by CNS and ANS- including sympathetic and parasympathetic)
2) Nutritive Capillaries (secrete local endothelin, neuropeptides to control vasculature in skin) |
|
|
Why does RP treatment focus more on blocking alpha adrenergic Receptors and relaxing vascular smooth muscle than activating B-adrenergic receptors?
|
There are more alpha adrenergic receptors in the peripheral vessels (B-adrenergics drop out in the periphery). Thus stimulating the B-adrenergics won't have as much of an effect.
|
|
|
The pathogenesis of systemic sclerosis involves what three main things?
|
1) fibrosis
2) vascular abnormalities 3) immune dysregulation |
|
What immune abnormalities are seen in Scleroderma?
|
Ag driven process (but the Ag is unknown). Lymphocytes are seen early on.
Th2 cells --> produce IL-4 --> activates macrophage --> release TGFB and PDGF --> induce fibroblast collagen production |
|
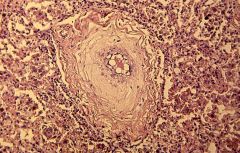
What is shown in this biopsy? Do you see inflammation?
|
Scleroderma vascular changes --- Don't see inflammatory cell! (this is not a vasculitis)
- intimal proliferation - intense medial hypertrophy - adventitial fibrosis |
|
What potent vasoconstrictor is responsible for the vascular changes seen in Scleroderma? What are some factors that balance out its effect?
|
Vasoconstrictor- ET-1
Vasodilator- NO, and EDHF *note the hypertrophied artery seen in this condition |
|
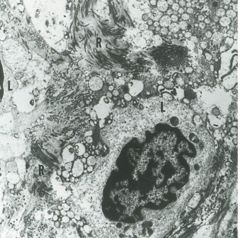
What is shown here? What condition is this seen in (note: it is a condition associated with systemic sclerosis)?
|
Plexiform lesion (from active vasoconstriction)
- seen in PHT (pulmonary HTN) |
|
|
Primary anti-fibrotic cytokines in SSc? What type of cell secretes them?
Primary pro-fibrotic cytokines in SSc? What type of cell secretes them? |
Anti-fibrotic (Th1). TNFα and INFg
Pro-fibrotic (Th2). TGFβ and PDGF |
|
|
How does TGFβ cause fibrosis in SSc? What about PDGF?
|
TGFβ bind to receptor --> causes Smad signaling cascade --> Smad translocates to nucleus causes gene expression of collagen.
Platelet derived growth factor binds to receptor --> via ERK-ROS signaling causes increased gene expression of collagen, inflammatory genes, and antiapoptotic genes. *note: TGFB upregulates PDGF (work synergistically) |
|

What is seen in this picture?
|
Sclerosis of the skin, can be disfiguring. There are distal contractures of the skin and retraction of soft tissue at finger tip --> causing digital ulcers.
|
|
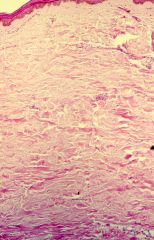
What is seen on this histologic image?
|

Infiltration of collagen. Initially patients have vascular engorgement and edema (increased swelling and stiffness of skin) which is later replaced by collagen.
Deposition begins on lower dermis and there is LOSS of hair follicles, sweat glands, etc. *trichrome stain shows extensive collagen |
|

What is this condition called?
|

Subcutaneous calcinosis in the finger and elbows. Can be seen on xray.
very characteristic of Scleroderma. |
|

What is the problem with the barium swallow of a patient with Scleroderma?
|
There is no esophageal peristalsis. In addition, the lower esophageal sphincter is wide open and patients can get reflux.
Fibrosis in the GI smooth muscle results in hypomotility throughout tract (in addition to dilatation, malabsorption, etc.) |
|
|
What unique GI systems are spared in patients with Scleroderma?
|
Liver and Pancreas!
|
|
|
What are the two main pulmonary findings in patients with SSc?
|
1) Pulm vascular disease- obliterative arteriopathy (small pulmonary arteries affected, develop HTN --> cor pulmonale)
2) Interstitial fibrosis |
|

Would you expect this chest x-ray to come from a patient with lc-SSc or dc-SSc?
|
dc-SSc (you tend to see more interstitial fibrosis in these patients). In lc-SSc you see more pulm HTN.
Note the honeycombing and parenchymal infiltrates. Patient likely has impaired gas exchange, dyspnea and cough. |
|
|
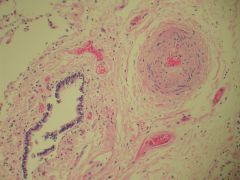
What cardiac problems can a person with Scleroderma present with?
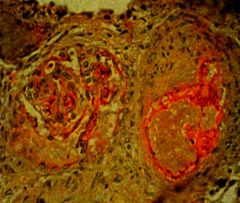
What do you notice in this histologic image of a kidney? |
Cardiac- mostly Right side heart failure (Cor pulmonale, HTN)
Renal- note onion skinning of artery --> patients can develop malignant HTN, renal crisis (azotemia --> increased SCr). They can also get necrosis of capillaries in the glomerulus. |
|
|
In a person with scleroderma, what lab values would you predict for the following:
- Hb - ESR - RF - ANA |
- low Hb (mild anemia)
- ↑ ESR (inflammatory marker- seen early on) - RF + - ANA + (in 90-95% of patients) |
|
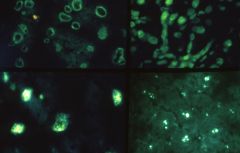
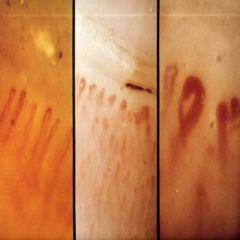
What is shown here?
If someone with Raynaud's syndrome came in and had this pattern, what would you tell them? |
Different patterns of ANA (periphral, diffuse, speckled, nucleolar). Many people have ANA and they also can have Raynaud's. Want to be cautious and do other tests, specifically look for Ab's to centromere or topoisomerase.
Diagnosis of scleroderma will come over time if skin changes, arthritis, etc. are seen |
|
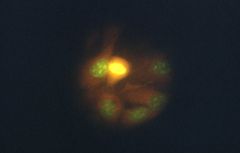
What is shown here? What type of systemic sclerosis does this individual likely have?
|
Anti-centromere antibodies (this is seen in lc-SSc or limited cutaneous scleroderma)
|
|
|
How do you treat scleroderma?
|
- symptomatic therapy
- physiotherapy (so they don't get contractures early on) *difficult to treat. Lack of response to steroids. |