![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
118 Cards in this Set
- Front
- Back
|
Characteristics of CRVO |
- usually UNILATERAL, but up to 7% may develop CRVO in fellow eye within 5yrs - men = women - elderly |
|
|
3 major Risk Factors for CRVO |
1) HTN (#1 RF) 2) Diabetes 3) POAG |
|
|
Pathogenesis of CRVO |
- physical blockage - lumina of the CRA & CRV are narrower at the lamina cribosa - vessels are bound by a common sheath - lamina limits expansion of ON & vessels - results in an obstruction to blood flow - thrombotic/atherosclerotic phenomenon - laminal constriction site for occlusion: nidis |
|
|
CRVO Symptoms |
- blurred vision - scotoma - sudden, painless loss of vision |
|
|
CRVO Appearance |
BLOOD & THUNDER! |
|
|
CRVO Signs |
- dilated, tortuous veins - deep & superficial hemorrhages - disc edema - CWS (NOT exudates) - collateral vessels - macular edema (main cause for vision reduc.) - anter/posterior segment neovascularization |
|
|
Describe the retinochoroidal collaterals that develop with CRVO: |
- "protective" effect - develop 3-14 months after occlusion - bypasses vascular bed occlusion - do not leak - in 5% CRVO w/ iris/angle NV - in 58% CRVO w/o iris/angle NV (PROTECTIVE!) |
|
|
Classification of CRVO |
1) Perfused (non-ischemic) 2) Non-perfused (ischemic) |
|
|
Perfused (non-ischemic) CRVO |
- less than 50% capillary non-perfusion - 70-80% of all CVO's - acuity better than 20/200 - deep hemorrhage (dot/blot) - should be treated as the TIP of the STYSTEMIC iceburg! - 83% of "interdeterminate" CRVO converts to ischemic - CWS are RARE! - NO APD |
|
|
Non-perfused (ischemic) CRVO |
- greater than 50% non-perfusion - 19-30% of all CVO's - will have +APD - poor VA - CWS present - 16% of all CRVO's develop NVI/NVA (CVOS) (very high risk of NVI/NVA via VEGF) |
|
|
What's the major complication (most serious) that can arise from CRVO? What is it correlated with? |
Neovascularization; correlated with the degree of capillary non-perfusion |
|
|
How is the amt of perfusion detemined with CRVO? |
- FA! - less than 10 DD of non-perfusion = perfused - more than 10 DD of non-perfusion = non-perfused |
|
|
What factors/signs differentiate Perfused (Non-ischemic) vs Non-perfusion (Ischemic)? |
- VA (worse with ischemic) - pupils (+APD with ischemic) - DFE (orange appearance & CWS w/ ischemic) - VF examination - FA (>10 DD ischemia with ischemic) - elctroretinogram |
|
|
What's the #1 reason for vision loss with CRVO? |
macular edema (other causes include: RPE atrphy, macular ishemia, retinal hemorrhage, NVG) |
|
|
What assessments should we do if we suspect CRVO? |
- FA - pupil testing - retinal photo - gonio (r/o NVA) - measure IOP - NVG evaluation |
|
|
How do we manage/treat CRVO? |
- systemic condition needs to be treated - refer for PRP if NVD, NVI, NVG or macular edema develops - f/u every 1-2 months for 6-8 months |
|
|
CVOS study |
- PRP only after NV is observed - macular laser did NOT have a significant effect on VA, thus is NOT indicated - SLE with gonio is mandatory
|
|
|
What is Papillophlebitis?
|
- CRVO in a young patient w/o systemic dz
- inflammatory etiology (unlike true CRVO) - prognosis is great; majority non-ischemic - disc swelling & disc edema - symptoms: GOLD & PURPLE flashing lights - do these tests: CVC w/ diff, lipid panel, BP, & tested for antiphospholipid AB syndrome - same neo complications as true CRVO - monitor 1 q mos until resolution |
|

Young, healthy patient with complaints of gold & purple flashing lights. What is the diagnosis? |
Papillophlebitis |
|
|
Characteristics of BRVO |
- elderly - males = females - more common than CRVO - less visually disabling than CRVO - involves one of the branch retinal veins - small, localized area of the retina or as much as a quadrant - most involve veins located temporal & superior to the disc |
|
|
BRVO Pathogenesis |
- venous compression at A/V crossing (75% of all BVO) - arteriolosclerotic etiology - sclerotic arteriole compreses on underlying venule leadint to leakage from capillary beds - VEINS/VENULES DO NOT LEAK - ALL leakage is from the CAPILLARIES |
|
|
BRVO Symptoms |
- reduced VA &/or VF may be present - often is ASYMPTOMATIC |
|
|
BRVO Classification |
1) Ischemic vs Non-ischemic 2) based on LOCATION |
|
|
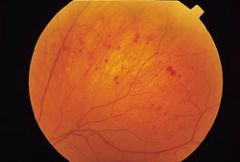
BRVO appearance |

|
|
|
3 location classifications for BRVO: |
1) Hemispheric: before 1st bifurcation (aka: HRVO) 2) Intermediate: after 1st bifurcation, typical BRVO appearance (MAJORITY OF BRVO CASES) 3) Twig: macular area only |
|
|
RFs for BRVO |
#1: HTN (70% of cases)
- systemic associations - DM - atherosclerosis - hyperlipidemia ETC |
|
|
Non-ischemic BRVO |
- 70-80% of cases - VA >20/200 - blot, flame shaped hemes - RARE to see CWS - mild macular edema - collateral vessel formation |
|
|
Ischemic BRVO
|
- defined as 5 DD of retinal capillary NON-perfusion on FA
- CWS - macular edema (most common cause of vision loss) - NVD/NVE/vitreous hemorrhage, tractional RD COMMON - NVI/NVG are RARE |
|
|
What's the most common cause of (irreversible) vision loss with BRVO?
|
macular edema
others: vitreous hemorrhage, tractional RD |
|
|
BRVO management
|
- refer for directed W/U
- monitor q1mo until resolution of hemorrhages - monitor every 4 months for next 3 yrs - possible FA at 3 mos - retinal pics at every visit - retinologist ONLY if complications develop |
|
|
HRVO |
- "hemi-retinal vein occlusion" - major branch occlusion at or near OD - occlusion of one of the trunks of central retinal vein - involves superior OR inferior drainage only - develops like CRVO, behaves like BRVO
|
|
|
RFs for HRVO |
1) HTN 2) Diabetes 3) Glaucoma |
|
|
What is OIS? |
Ocular Ischemic Syndrome is hypoperfusion of the anterior & posterior segments of the eye due to carotid obstructive disease. |
|
|
OIS Etiology |
- usually unilateral - internal carotid artery atheromatous ulceration & stenosis at bifurcation of common carotid artery - only occurs if stenosis >90% = NO BF in eye - males > females - 50-80 y/o
|
|
|
What's the 70-70 Rule with OIS? |
- 70% of BF to brain is thru internal carotid artery - don't start to get in trouble until you have at least 70% occlusion - with 90% stenosis, you only drop down to 50% perfusion in CRA |
|
|
Chronic signs of OIS |
- diminished vision in bright light - PAIN - progressive vision loss |
|
|
Systemic correlations with OIS |
- systemic mobidity (arterial HTN, DM, ischemic heart dz, stroke, peripheral vasc. dz, etc) - less common causes include: GCA
|
|
|
What is the #1 cause of mortality in OIS pts? |
- CARDIAC DEATH is #1 cause of mortality |
|
|
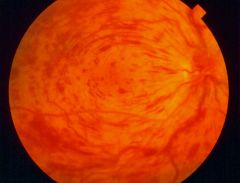
OIS posterior findings |
- dilated, NOT tortuous veins - dot/blot hemes in MIDPERIPHERY - hemorrhages are usually more scattered (unlike with CRVO, more confluent) - macular edema - CWS - spontaneous arterial pulsation (IOP exceeds pressure w/in CRA) |
|
|
OIS anterior segment findings |
- diffuse episcleral injection & corneal edema - aq. flare with few cells (ischemic pseudo-iritis); where the pain comes from! **may appear like uveitis (dilate your pts!) - iris atrophy & a mid-dilated/poorly reacting pupil - RUBEOSIS IRIDIS is common & often progresses to NVG - cataract in very advanced cases (prolonged ischemia) |
|
|
What should you expect on FA with OIS patient? |
1) early phase shows delayed choroidal filling & prolonged arteriovenous transit time 2) late phase shows disc & perivascular hyper-fluorescence & leakage at post. pole |
|
|
OIS management |
- r/o HTN, DM, cardiac dz, etc - carotid ultrasound or doppler ( >70% w/o symp or >50% w/ symp --> carotid endartectomy or stenting) - anterior segment treat with topical steroid & mydriatis - NVG treated medically & surgically - proliferation requires PRP |
|
|
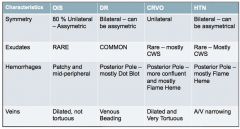
What are some differences between CRVO, DR, HTN, and OIS? |
|
|
Mid-peripheral hemes, dilated (not tortuous) vessels - what is most probably diagnosis? |
OIS |
|
|
What should you do if your CRVO pt has signs of NVD, NVE, NVI? |
refer to retinal specialist for PRP! |
|
|
What's the hallmark of CRVO? |
sudden, painless loss of vision |
|
|
According to the BVOS study, can photocoagulation (grid laser) improve VA in eyes with macular edema? |
YES! Grid laser is STD of care for macular edema in BRVO! 65% incr. VA by 2 lines! |
|
|
According to the BVOS study, can PRP prevent VH in eyes with NV? |
32% absolute risk reduction |
|
|
Describe the classifications of MACULAR EDEMA in BRVO (perfused & ischemic). |
Perfused: most common, leakage (FA), 1/3 spontaneously resolve, frequently has persistent decr. in VA |
|
|
What does the BVOS study have to say about treating macular edema? |
1) 3-18 mo window of opportunity to tx |
|
|
How should you manage a BRVO patient? |
1) refer to internist for w/u |
|
|
Is macular grid laser tx effective in improving the vision in eyes with CRVO & VA 20/50 or worse due to macular edema? |
NO! |
|
|
T or F: NVD/NVE, VH, Tracitonal RD may cause permanent severe vision loss in BRVO? |
True. |
|
|
What is common in CRVO, but rare in BRVO? |
NVI/NVG |
|
|
What's the "50% Rule"? (Hint: BRVO) |
1) If the BRVO involves at least 1 quadrant, there's a 50% chance of developing 5DD+ of retinal non-perfusion. |
|
|
Name at least 2 ways that BRVO differs from CRVO. |
1) ischemic classification (>10DD for CRVO; 5DD for BRVO) |
|
|
HRVO develops like _____(CRVO, BRVO), but behaves most like _____ (CRVO, BRVO). |
CRVO; BRVO |
|
|
Conclusion of SCORE study regarding BRVO. |
NO significant differences among the 3 tx groups. |
|
|
HRVO involves what kind of drainage? |
superior or inferior ONLY |
|
|
This study focused on Triamcinolone for CRVO. |
SCORE (std care vs corticosteroids for retinal vein occlusion) = std of care for CRVO is NO longer just "watching it until neo"; now it is INJECTIONS if CRVO pt has macular edema (no grid laser, but yes to injectables) |
|
|
What's the most common cause of vision reduction in BRVO? |
Macular edema |
|
|
What conclusion was made about SLE in the CVOS study? |
SLE with GONIO is MANDATORY! (need to rule out NVI/NVA!) |
|
|
What's the most significant RF for predicting NVI/NVA? |
amount of non-perfused retina (remember that with ischemic CRVO, you have >10DD of non-perfusion; high risk of NVI/NVA with ischemic CRVO) |
|
|
When should you follow up with your CRVO pt?
|
20/40 or better: q1-2 mos x6mo |
|
|
T or F: Of "inteterminate" CRVO cases, roughly 80% will progress to ischemic CRVO. |
True. |
|
|
What did the CVOS declare about doing macular laser? (Hint: CRVO study) |
Macular laser did NOT have a significant effect on VA, thus is NOT indicated. In CRVO, just WATCH macular edema until NEO develops. |
|
|
T or F: Papillophlebitis' etiology is different than that of CRVO. |
True. |
|
|
What's a unique symptom of Papillophlebitis? |
Gold & Purple flashing lights |
|
|
T or F: Sclerotic arteries leads to compression on underlying venule, which causes the venue to leak. (Hint: BRVO) |
FALSE. |
|
|
T or F: BRVO is often asymptomatic. |
True. (Often, but not always..may present with loss of VA or VF.) |
|
|
"Define" Ischemic BRVO. |
5DD of retinal capillary NON-perfusion on FA |
|
|
CRVO or BRVO: Which one is more visually disabling? Which is more common? |
CRVO; BRVO (3x's more common) |
|
|
Characteristics of Macular Holes |
- usually 6th or 7th decade of life - more common in females (2:1) - usually uniliateral (10-20% bilateral)
|
|
|
Macular Hole symptoms |
- painless, central vision loss - early: central metamorphopia or blue, micropsia - late: severe decr. in central vision - symptoms noticed with other eye closed |
|
|
Macular Hole Pathophysiology |
- shrinkage of the perifoveal vitreous cortex (perifoveal vitreous "shrinks up") - incomplete perifoveal PVD - foveal adherance of posterior hyaloid --> vitreous traction on the fovea |
|
|
How many stages of macular holes are there? |
4 |
|
|
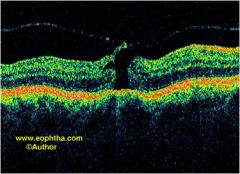
Describe Stage 1a (impending) of macular holes: |
- split in inner retina - cystic space (pseduocyst) - vitreous pulls at the fovea - photoreceptor layer intact - loss of foveal light reflex - yellow spot - 50% resolve spontaneously |
|
|
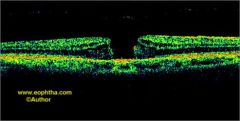
Describe Stage 1b of macular holes: |
- pseudocyst enlargement - extension to the outer retina, disrupting photoreceptor layer - small central yellow ring - loss of foveal depression |
|
|
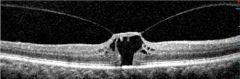
Describe Stage 2 of macular holes: |
- roof of cyst opens ("can opener") - full thickness defect less than 400um in diamter - small retinal defect (hole) seen within yellow ring |
|
|
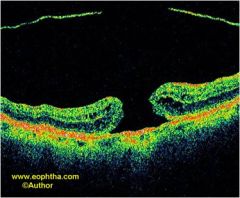
Describe Stage 3 of macular holes: |
- full thickness defect more than 400um in diameter - thickened edges due to intraretinal cystoid spaces - central, RED round full thickness retinal defect - surrounding, subretinal fluid cuff |
|
|
Describe Stage 4 of macular holes: |
- Stage 3 + PVD (possible Weiss ring) |
|
|
Describe VA of each stage of macular holes: |
Stage 1a/b --> 20/20-20/50 Stage 2 --> 20/50-20/200 Stage 3 --> 20/200-20/800 Stage 4 --> 20/200-20/800 |
|
|
What are some diagnostic tests to run for macular holes? |
- OCT (useful for staging) - Watzke-Allen Test |
|
|
What is the Watzke-Allen test? |
- put narrow beam over center of hole - w/ macular hole, pt reports beam broken or thinned - w/ pseudohole or cyst, pt reports beam distorted |
|
Determine the stage of this macular hole: |
Stage 1a (impending) |
|
Determine the stage of this macular hole: |
Stage 1b |
|
Determine the stage of this macular hole: |
Stage 2 |
|
Determine the stage of this macular hole: |
Stage 3 |
|
Determine the stage of this macular hole: |
Stage 4 |
|
|
How you do manage each stage of macular hole? |
Stage 1: monitor; 50% spontaneously resolve
Stages 2-4 (full thickness): treatment required IF 20/40 or worse for VA |
|
|
What's the treatment for Stages 2-4 Macular Holes? |
Surgical Tx: 1) Vitrectomy (PPV) 2) Peeling of ILM 3) Fluid-gas exchange 4) Post-op face-down positioning |
|
|
Describe the post-op of macular hole repair: |
- after surgery to repair the macular hole, the pt should be positioned face down for 24 hrs for 5-10 days |
|
|
What's the #1 complication of macular hole surgery? |
CATARACT! (75%) |
|
|
What does ERM stand for? |
Epi-retinal membrane |
|
|
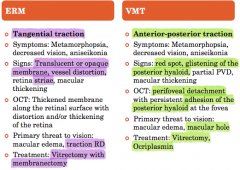
Characteristics of ERM |
- aka: mucular pucker, cellophane maculopathy - fairly common in pts over 40 y/o - bilateral involvement in 20-30% of cases |
|
|
What are the causes of an ERM? |
- idiopathic (most common!) - following intraocular sx - retinal vasc. dz - intraocular inflamm. - trauma |
|
|
What are symptoms of an ERM? |
- blurred vison - metamorphopsia - macropsia due to crowding of the photoreceptors
(mild, transparent ERM are often asymptomatic) |
|
|
What are the clinical signs of an ERM? |
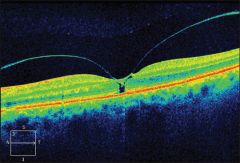
- presents as a translucent, shimmering or whitish gray membrane along inner retina - retinal traction can cause: distortion/tortuosity of BVs, retinal striae, & CME - OCT is great test to view ERM |
|
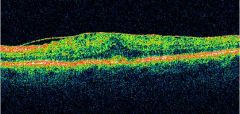
What is the shimmering membrane in this OCT photo? |
ERM |
|
|
Complications of ERM |
- contraction of ERM can cause distortion/folds of inner retina - in some cases, there may be edema visible as black spaces (OCT) in the outer retina |
|
|
ERM Pathophysiology |
- ERM are due to proliferation of retinal GLIAL cells (as well as other cells) at the vitreoretinal interface - the cells gain access to the retinal surface through breaks in the ILM - PVD is believed to play a role in development of ERM |
|
|
How do you manage ERMs? |
- surgery is typically recommended in pts with BCVA of 20/40 or worse (or severe metamophopsia) |
|
|
What's the treatment for ERMs that need it? |
1) Vitrectomy (remove vitreous) 2) Membranectomy (ERM peeled off) |
|
|
What's the expected outcome after ERM tx? |
- VA usually improves 50% - most pts have decr. in metamorphopsia |
|
|
What's the #1 complication of ERM tx? |
CATARACTS! (just like macular hole tx!) |
|
|
What does VMT stand for? |
Vitreomacular Traction |
|
|
What is VMT? |
- condition in which the vitreous gel has an abnormally strong adhesion to the retina - complication of incomplete PVD - exerts anterior-posterior traction on the fovea |
|
|
Clinical signs of VMT |
- early stages may be hard to see - may see glistening of the posterior hyaloid - partial PVD usually present - center of fovea may show reddish or yellowish spot - macula may appear thickecned due to edema |
|
|
What does VMT look like on an OCT? |
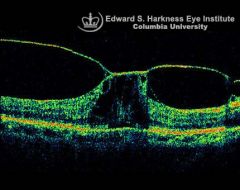
- bright posterior hyaloid tenting up the fovea & surrounding area - perifoveal vitreous detachment |
|
|
What are the threats to vison from VMT?
|
- CME or macular hole formation
- the narrower the VM attachment, the greater the force exterted upon the macula in that area, the greater the risk of macular hole formation - VMT & EMR can occur simutaneously |
|
|
How do we manage/tx VMT? |
- early, asymptomatic VMT observed for progression w/o tx - previously, vitrectomy was the only tx - intravitreal injections of an enzymatic agent is a new treatment approach that was FDA approved |
|
|
What's the name of the intravitreal injection used to treat VMT? |
Ocriplasmin (Jetrea)
- side effects: floaters (NOT cataracts!) |
|
|
What are the differences between an ERM & VMT? |
|
|
|
What is a Pseudohole? |
- have intact photoreceptor layer - commonly retain near normal VA - caused by ERM contraction - ERM that have a central opening in the foveal area - normal central foveal thickness - incr. parafoveal thickness |
|
|
How do we manage/tx Pseudoholes? |
- surgical peeling of the ERM is indicated when vision is reduced (worse than 20/40) |
|
|
What is a Lamellar Hole? |
- result of an abortive process of macular hole formation - VA is usually preseverd - macular shoes a stable, round, well circumscribed REDDISH lesion - irregular foveal contour - split b/w the layers - photorectpor layer intact - bi-lobed or anvil-shaped |
|
|
How do we manage/tx Lamellar Holes? |
- typcally stable condition - tx usually not necessarily (acuity preserved) |
|

What is the finding on the left? On the right? |
Left: pesudohole Right: lamellar hole |