![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
39 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
ETDRS criteria for treatment of DME |
"ME, HE ME, ME X3 in groups of 500 from the foveii " ME within 500 microns of fovea Hard exudate within 500 microns assoc w ME ME 1500microns in size area within 1500 microns of fovea |
|
|
|
Fleck retinas DDX |
"DR FAKES" D dominant drusen R retinitis punctata albicans FA fundus albipunctata Kandoori Fleck retina E S Stargardts disease fundus flavi |
|
|
|
Severe NPDR Criteria |
4 quadrants of aneurysms 2 quadrants of Venous beading 1 quadrant of IRMA |
"4 neuysms, 2✌(V) enous beading, (1)👆 1RMA |
|
|
CME DDX |
D diabetes E E 2 prostaglandin analog P pars planitis R RP I Irving Gas V venous obstruction E epi N nicotinic acid |
"Deprive'n'" |
|
|
DDX for CNV |
" escapes the Net Streaks across the "Stars" TH BEST RHINO STREAKS across stars sending SOS VKH
Trauma Bests RP Histo Idiopathic Neoplasms Optic pits drusen Angioid streaks (Pepsi) Myopia
VKH Choroidal nevus SO Serpiginous SARCOIDOSIS |

|
|
|
Central Retinal artery supplies? |
NFL Ganglion cells Inner plexiform layer Inner nuclear layer TO MLM (OPL) |
|
|
|
Choroidal blood supplies? |
Up to MLM (OPL) ONL (PR Cell bodies) Rod cones RPE |
|
|
|
Macular star what layer? |
Henle layer or OPL in macula (radial orientation in macula) |
|
|
|
ELM and ILM what cell? |
ILM Meullers footplate (true BM) (Gunns dots, visible at Ora) ELM Tight junction between PR Cell bodies and mullers (not a true BM), demarcates beginning of rods and cone elements |
|
|
|
11 cis retinol -> all Trans retinol happens where? |
Rods and cones outer segment |
|
|
|
All Trans retinol -> 11 cis retinol? |
RPE |
|
|
|
How many Rods? Where most dense? |
100M most dense in 20° ring around fovea |
|
|
|
How many cones? Where? Which color pigment most? |
5M vs (100 M rods) 50% in macula 45% green, 45% red 10% blue |
|
|
|
Which rod or cone discs are attached to cell membrane which are free floating? |
Rods "discrete" Cones "connected" |
|
|
|
Definition of peripheral retina |
Any retina that is a single ganglion cell thick. |
|
|
|
ERG What retinal cells are stimulated? |
Mueller PR Bipolar Ganglion cells are not! |
|
|
|
Why is ERG not helpful in glaucoma? |
Ganglion cells are not measured |
|
|
|
What does a flicker ERG evaluate and how? |
Isolates cone response by flashing so rapidly rods do not have time to recycle rhodopsin |
|
|
|
What ERG isolates rods? |
Dim light, dark-adapted ERG |
|
|
|
Normal ERG w abnormal EOG (only 5 conditions) |
"If you're gonna Dominate the Best Eggs contest hold them very stationery , and pattern dye them with Chlorox "
Autosomal Dominant Best- abnl EOG Stay put- stationary night blindness. (CSNB) Pattern dystrophy ChlOROquine X- x linked retinoschsis |
"If you want the Best Damn Pattern for your Easter Eogs, hold them still (stationary) and Pat dry them with Chlorox" |
|
|
"LISN" Lebers Idiopathic Neuroretinitis Age? M or F? Unilateral or bilateral? + or - APD? VF? How does it contrast from MS? (2) FA? vitreous? Disc? |
"Think optic neuritis that isn't MS" 20s, M=F, unilateral APD Central or cecocentral scotoma Vitritis Disc edema Macular Star "hot disc " on FA Prognosis excellent!! |
|
|
|
DDX for angioid streaks |
PEPSI PXE Ehrlers danlos Paget dz of bone SCA Sickle cell Idiopathic |
|
|
|
Salt and pepper retinopathy |
"MRS CL COOKS " w salt and pepper Medications mellaril, thorazine clofazamine R rubella RP in x-linked recessive carriers Syphilis Lebers congenital amaurosis Carrier's of CHOROIDEREMIA and albinism Cystinosis O O Kearn- Sayre syndrome |
|
|
|
RRD RULE of 7s |
0.07% will have RRD if live to 70 7/100,000 will dev RD 0.7% pop retinal breaks 7% pop has lattice but not the cause In 70% of RRD. Lattice has 0.5% (7x) risk of RD |
|
|
|
Bullseye Maculopathy |
CARCASS C one Dys A R ARMD C A Chloroquine antimalarials, central Areolar dystrophy benign S Stargardts S spiel meter-Batten--mayeau |
|
|
|
PVR classification |
ABC CAP A grade better than B, better than C C contraction A anterior extent P posterior extent |
|
|
|
Stickler Syndrome |
Syndrome Sticks to retina Risk of retinal detachment Syndrome: arthropathy, Pierre Robin sequence |
|
|
|
Wagoners Disease |
wag tail cuz they're happy they don't have RD Low risk of RRD WaG n ER s. Abnormal ERG |
|
|
|
Cholesterolosis vs Asteroid |
Scinchisis scintillans (cholesterolosis) Cholesterolosis Collects Caudilly Sinks to the bottom of vit Cholesterol scintillates like a hollenhorst plaque |
|
|
|
Peripheral NV |
USUAL SICK "PEROPHFEREALS" USUAL usual suspects DM and BRVO Sick sickle cell P PArs Planitis E emboli hyperviscosity synd ROP H Hyperviscosity FEVR EALES A autoimmune like Lupus S Sarcoid |
|
|
|
Retinoschisis vs RD |
"Hypergun skis are absolutely smooth. They bite no dust and leave no marks " Hyperopia Gunns dots muller cells Absolute scotoma Smooth dome BITE Bilateral inferiotemporal No tobacco dust No demarcation lines |

|
|
|
Nyctylopia |

GlaUCOmAZ: 1st COMes Meds (miotics), then Laser, CAR, RP, make it hard at night to see. " GlaUCOmAZ: 1st COMes Meds (miotics), then Laser, CAR, RP, make it hard at night to see. CSNB Oguchi's (a form of CSNB) Myopia CSNB Oguchi's (a form of CSNB) Myopia
G gyrate atrophy Laser PRP A laser PRP U Unreal ( hysteria) C CSNB, choroideremia O optic atrophy Oguchi's dz (form of CSNB) M myopia miotic meds (phenothiazine, chloroquine, quinine A vit a Z zinc def
|
1st COMES GLAUCOMAZ, then meds, CAR, RP, make it hard at night to see |
|
|
Internal reflectivity melanoma vs choroidal hemangioma |
MeLanoma has Low internal |
|
|
|
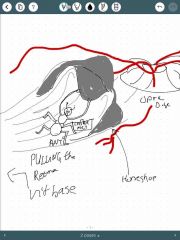
Horseshoe retinal tear |
Horseshoe tear always has its base, open end, anteriorly toward the vit base. Horse always walks toward the disc LASER ANTERIOR BASE! inadequate laser to base is number 1 reason laser tx fails after treating RD tear |
|
|
|
Hearing loss and Retinal degeneration |
"RUB your thinking cap and USHER them to the Cockeyed HARD OF hearing ward"
Rub rubella Usher syndromes Cockeyed cockayne syndrome H Hollegrens syndrome, hurlers syndrome A Alports syndrome, Allstroms s R Refsums syndrome D dysplasia spondyloepiphisia congenita O osteopetrosis F Freidreichs ataxia Flynn aerd syndrome Wardenburgs syndrome |
|
|
|
Choriodal melanoma vs choroidal nevus |
Breaks in BRUCHS membrane B breaks in Bruchs R retinal detachment serous U up elevated >3mm C color orange flecks suggest melanoma H hyperfluorescent pinpoints S Size change growth = melanoma |
|
|
|
Choriodal melanoma vs choroidal nevus |
Breaks in BRUCHS membrane B breaks in Bruchs R retinal detachment serous U up elevated >3mm C color orange flecks suggest melanoma H hyperfluorescent pinpoints S Size change growth = melanoma |
|
|
|
Radiation retinopathy |
15/30 rhymes "15 months and 30 gray before retinopathey " |
|
|
|
Choroidal folds |
"THIN RPE" Undulating RPE over contracted choroid or Bruch Yellow elevated crests alternate w darker bands FA- light bands hyperfluoresce at Crest (due to stretched out RPE) same as fundus appearance
T Tumors H hypotony I inflammation /idio N NV R retrobulbar mass P Papilledema E extra ocular hardware |
|