![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
111 Cards in this Set
- Front
- Back
|
Name 3 quantities measured with a spirometer commonly reported in a pulmonary function test. |
Forced vital capacity (FVC) Forced expiratory volume in 1sec (FEV1) FEV1/FVC |
|
|
Normal FEV1/FVC |
80% |
|
|
Name two broad types of respiratory diseases and explain how you could easily distinguish them with a spirometer. |
Obstructive disease FVC ➘ and FEV ➘➘ ⇒ FEV/FVC < 60% Restrictive disease FVC ➘ and FEV ➙ ⇒ FEV/FVC > 80% |
|
|
For a constant lung volume, how would be the intrapleural pressure compared to normal in the following diseases:
Asthma Interstitial fibrosis Emphysema Rheumatic valve disease |
Defined by the compliance Interstitial fibrosis: much more negative (smaller compliance) Rheumatic valve disease: more negative (smaller compliance) Asthma: less negative (higher compliance) Emphysema: much less negative (higher compliance) |
|
|
How is the total lung capacity (TLC) and residual volume (RV) in obstructive and restrictive disease? |
Obstructive: higher TLC, higher RV Restrictive: lower TLC, lower RV |
|
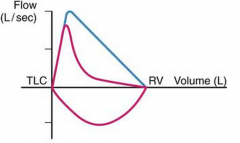
Diagnosis? |
Emphysema/COPD |
|
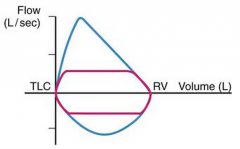
Diagnosis? |
Upper airway obstruction |
|
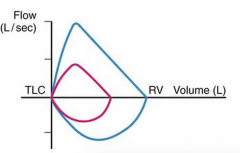
Diagnosis? |
Restrictive disease |
|
|
Name two conditions that may lead to upper airway obstruction. |
Foreign body Neoplasia |
|
|
How would you diagnose asthma? |
1. Low peak expiratory flow rate that responds to beta2-agonists 2. Atopic status (eosinophilia or IgE) 3. Bronchial hyper-responsiveness to methacholine (muscarinic agonist) or exercise |
|
|
Name one method you could use to measure residual volume |
Body box Helium concentration |
|
|
Name three mechanisms that may lead to obstructive lung disease and name one example of a disease in which each mechanism occurs. |
Material within airways Retained secretion (chronic bronchitis) Mucous plugs (asthma) Oedema fluid (pulmonary oedema) Inhaled foreign body Increased thickness of airways Inflammation (chronic bronchitis or asthma) Hypertrophy of mucous glands (chronic bronchitis) Hypertrophy of bronchiole smooth muscles (asthma) Destruction of alveolar wall Emphysema |
|
|
Name 3 microstructural abnormalities that you would expect in asthma |

Mucous plugs Mucous oedema Increased mucous glands Inflammation Hypertrophy of smooth muscles |
|
|
Name 3 microstructural abnormalities that you would expect in chronic bronchitis |
Retained secretions Inflammation Hypertrophy of bronchiole mucous glands Oedema of the airway walls |
|
|
Name four examples of a condition leading to obstructive disease |
Emphysema (COPD) Chronic bronchitis Asthma Pulmonary oedema Inhaled foreign body |
|
|
What two pathologies define COPD |
Emphysema Chronic bronchitis |
|
|
Briefly describe what emphysema means |
Enlargement of air spaces distal to terminal bronchioles with destruction of their walls |
|
|
Where is emphysema more likely to occur? Why? |
At the apex because intrapleural pressure (and hence also alveolar size) is large at the apex so that stress is higher at the apex.
|
|
|
Define chronic bronchitis |
Defined clinically: Excessive production of mucous in the bronchial tree sufficient to cause excessive expectoration of sputum. |
|
|
Typical pathogenesis leading to chronic bronchitis |
Hypertrophy of mucous glands producing enormous amount of mucous that overwhelm the mucociliary escalator. |
|
|
How can COPD present?
|
In two types: Type A (Emphysema) "Pink puffer" Type B (Chronic bronchitis) "Blue bloater" |
|
|
Why can COPD present in two different types? What makes a patient switch between presentations? |
The Type B has, in the stages of coping with hypoxaemia, traded-off the distress associated with hyperventilation with a lower pH and a poorer control of blood gas in general |
|
|
Name 5 clinical features present in Type A (emphysema) COPD |
Thin person Desperately SOB Enlarged lungs Almost normal PO2 Normal PCO2 |
|
|
Name 5 clinical features present in Type B (chronic bronchitis) COPD |
Coughing up mucous (Sputum pot next to bed) Lying in bed Cyanotic Low PO2 High PCO2 Right heart failure |
|
|
One of your patient is suspected to have COPD with emphysema and a CXR is acquired. Name 3 features that you expect to see. |
Over-inflated chest (ribs are more horizontal) Low diaphragm Narrow mediastinum Over-penetrated lung fields |
|
|
Name 2 features that you expect from a pulmonary function test in a patient with COPD |
Low FEV/FVC Scooped descent of flow-volume curve |
|
|
If you were to measure TLC, FRC and RV in a patient with COPD, how would they be? |
All increased |
|
|
How is physiological dead space in COPD? |
Increased |
|
|
How is physiological shunt in COPD? |
Increased |
|
|
How is alveolar-arterial PO2 difference in COPD? |
Increased |
|
|
How is the pulmonary blood pressure in COPD? Why (4 reasons)? |
Pulmonary hypertension due to: Destruction of capillary bed Hypoxic vasoconstriction Polycythaemia increasing blood viscosity Thickening of the walls of small arteries |
|
|
How would the heart function in COPD? Name three consequences of this condition. |
Right-sided heart failure (because of pulmonary hypertension), possibly causing: Right ventricular dilation Pulmonary oedema Fluid retention |
|
|
How is the work of breathing in COPD? |
Enormous |
|
|
Name five elements of management of patients with COPD |
Bronchodilators (beta2-agonists) Promotion of smoking cessation Vaccination against pneumococcus and influenza Antibiotics (for bronchitis) and prevention of exacerbation Continuous oxygen therapy Rehabilitation programs |
|
|
What drives respiration in COPD? Why? |
Hypoxaemia is the biggest drive to ventilation because: 1. pH of the CSF (responsible for activation of central chemoreceptors) is normal due to increased HCO3 in the CSF 2. pH of the blood (responsible for activation of peripheral chemoreceptors) is normal due to renal compensation |
|
|
Define asthma |
Increased responsiveness of airways to various stimuli, manifested by inflammation and widespread narrowing of airways. |
|
|
Name one other allergic reaction present in asthmatic patients |
Eczema |
|
|
Name four sources of hyperreactivity of airways in asthmatic patients |
Allergen Smoke Cold air Exercise |
|
|
Pathogenesis of asthma |
1. IgE bind to mast cells 2. Mast cells release histamine, PG, leukotrienes, bradykinin, interleukin, ... leading to inflammation 3. Inflammation causes (i) dilation of capillaries and increased permeability and (ii) contraction of airway smooth muscles (by decreasing cAMP). |
|
|
What drug would you give in acute asthma that does not settle with beta2-agonists? |
Muscarinic antagonists (Ipratropium bromide) |
|
|
What drug would you give in chronic asthma that does not settle with beta2-agonists? |
Corticosteroids (oral tablets or inhaler) |
|
|
Name an add-on therapy that may be tried in asthmatic patient that do not respond well to salbutamol. |
Leukotrienes antagonists |
|
|
Name 2 classes of drugs for acute bronchodilation and for each, name two examples. |
β2 agonists (salbutamol, salmeterol) Methylxanthines (theophylline, aminophylline) |
|
|
Name one drug that prevents histamine release by mast cells |
Sodium cromoglycate |
|
|
Name two broad effects of corticosteroids |
Inhibits cytokine transcription Potentiates beta2 receptors |
|
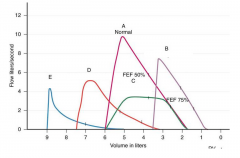
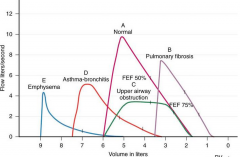
Label the various curves with a causative condition. |
|
|
|
Name 2 features that you expect from a pulmonary function test in a patient with asthma |
FEV/FVC ➘ (responsive to bronchodilators) Not scooped expiratory flow-volume curve |
|
|
If you were to measure TLC, FRC and RV in a patient with acute attack of asthma, how would they be? |
All increased |
|
|
Name two conditions in which airway resistance is expected to increase? |
Asthma and COPD |
|
|
How is alveolar-arterial PO2 difference in asthma? |
Increased
|
|
|
How is PO2 and PCO2 in asthma? |
Region with low V/Q => Low PO2 and normal PCO2 due to hyperventilation |
|
|
How is physiological shunt in asthma? |
No shunt |
|
|
Name three clinical features of upper airway obstruction |
Inspiratory and expiratory wheezes (because the obstruction is always there) Hypoxaemia CO2 retention No response to bronchodilators Flattening of flow-volume curves |
|
|
Name 3 causes of tracheal obstruction |
Inhaled foreign body Enlarged lymph nodes Enlarged thyroid gland Stenosis after tracheostomy |
|
|
Name 3 causes of bronchial obstruction |
Inhaled foreign body Aspiration following surgery Retained secretions Neoplasm in bronchus Enlarged lymph nodes Misplaced endotracheal tube |
|
|
On which sides are bronchial obstructions more likely? Why? |
Right because the left bronchus makes a sharper angle |
|
|
After giving oxygen therapy to your patient, you notice that he now presents with lung collapse. Why did that occur? |
Partial pressure of O2 in O2 therapy is much larger than that in the blood so that most of it is absorbed by the blood thus considerably decreasing the pressure in the alveoli which may eventually collapse. This does not occur with normal air since it mostly contains N2 at a partial pressure that is about equal to that of the blood. |
|
|
Define restrictive disease
|
Expansion of the lung is restricted because of alterations in the parenchyma or because of diseases of the lung pleura, chest wall or neuromusculature. |
|
|
Name 3 conditions in which rapid shallow breathing may be observed |
Pulmonary oedema Pulmonary fibrosis Asthma Pneumonia Anxiety |
|
|
Name three characteristics of the respiratory mechanics that are altered in pulmonary fibrosis. |
Low FEV and FVC but normal or increased FEV/FVC ratio All lung volumes decreased Reduced lung compliance |
|
|
Name one condition in which airway resistance is decreased |
Pulmonary fibrosis |
|
|
Name two disease processes in which gas exchange is impaired. |
Pulmonary oedema Pulmonary fibrosis |
|
|
Name 3 conditions that may lead to pulmonary hypertension |
Pulmonary fibrosis Pulmonary embolism Emphysema Mitral stenosis Exercise Hypoxia (leading to hypoxic vasoconstriction) Primary pulmonary hypertension |
|
|
Name three disease processes of restrictive lung disease |
Pulmonary fibrosis Pneumothorax Pleural effusion Pleural thickening Chest wall disease (Scoliosis, Ankylosing Spondylitis) Neuromuscular diseases (Polio, Guillain-Barré, myasthenia gravis, muscular dystrophy) |
|
|
Describe the permeability of the epithelium and endothelium of the blood gas barrier. |
Endothelium: very permeable to water, ions and even some proteins Epithelium: mostly impermeable with active transport |
|
|
Describe alveolar oedema |
Last stage of pulmonary oedema where the capillary pressure is so high that the interstitial pressure rises as well and fluid spills into alveoli. RBC can be found in alveoli as well due to damage to epithelium |
|
|
Name 4 common mechanisms through which pulmonary oedema may occur and for each name one example. |
Starling's forces: 1. Increased capillary hydrostatic pressure (e.g. fluid overload, PE, MI, LHF) 2. Increased capillary permeability as in inflammation (e.g. inhaled or circulating toxins) 3. Decreased interstitial hydrostatic pressure (e.g. rapid removal of pleural effusion or pneumothorax) 4. Decreased osmotic pressure of capillary (e.g. saline overtransfusion, hypoproteinaeima) |
|
|
Is the fluid in pulmonary oedema an exudate or a transudate? |
It depends: Early oedema due to increased capillary pressure ⇒ Low protein content ⇒ Transudate Late oedema due to increased capillary pressure ⇒ High protein content (due to damage to walls)⇒ Exudate Oedema due to increased capillary permeability ⇒ High protein content ⇒ Exudate |
|
|
Name 3 symptoms of pulmonary oedema |
Dyspnoea Orthopnoea Sudden nocturnal dyspnoea Cough (maybe with pink sputum due to RBC) |
|
|
What can you expect on auscultation of pulmonary oedema? |
Crackles |
|
|
What do you expect to see on CXR of pulmonary oedema? |
Shadowing (in alveolar oedema) or septal lines (in interstitial oedema) |
|
|
How would be the lung compliance in alveolar oedema? |
Lung compliance ➘ |
|
|
How would be the airway resistance in alveolar oedema? |
Airway resistance ➚ |
|
|
Do you expect V/Q mismatch and shunt in alveolar oedema? |
Yes, both. |
|
|
How PCO2 be in alveolar oedema? |
Normal |
|
|
Name three mechanisms through which PE can occur and name a few examples for each. |
Virchow's triad Blood stasis Immobilisation, venous obstruction, heart failure or dehydration, sickle cell Hypercoagulability Polycythaemia, contraceptive pills, malignancy, liver disease Abnormality of vessel wall Trauma, sepsis, inflammation |
|
|
Name 3 features observed in medium-size PE |
Pleuritic pain Dyspnoea Coughing with blood-stained sputum Mild fever Pleural friction rub Pleural effusion |
|
|
Name 3 features observed in massive-size PE |
Sudden collapse Shock Pallor Central chest pain Loss of consciousness Systemic hypotension Pulmonary hypertension Pulse rapid and weak (RHF) Raised JVP (RHF) |
|
|
How is the dead space in PE? |
Increased |
|
|
Why can we observe collapse secondary to PE? |
Because in PE, surfactants are depleted |
|
|
Define cor pulmonale |
Right heart disease secondary to lung disease |
|
|
Name 3 mechanisms through which cor pulmonale may occur |
All lead to pulmonary hypertension: Destruction of the capillary bed (emphysema, COPD) Hypoxic vasoconstriction Polycythaemia |
|
|
What is the relative proportion of small cell lung cancer in all lung cancers? |
15% |
|
|
Name three differences between small cell and non small cell lung cancers |
Prevalence amongst lung cancer Small cell: 15% Non-small cells: 85% Size of cells Small cell: smaller than normal cells Non-small cells: not smaller than normal cells Malignancy Small cell: shorter doubling time, higher growth fraction Non-small cell: longer doubling time, lower growth Metastases Small cell: early metastasis Non-small cell: late metastasis Treatment Small cell: more responsive to chemotherapy Non-small cell: less responsive to chemotherapy Ectopic production of hormones Small cell: ADH, ACTH Non-small cell: PTH Location Small cell: more common centrally by the hilum Non-small cell: more common at the apex |
|
|
Most common type of lung cancer |
Adenocarcinoma |
|
|
Name two respiratory complications of bronchial cancer |
SOB (by blocking air entry and possibly by compressing phrenic nerve)
Infections (by blocking blood vessels) |
|
|
Name three non-pulmonary complications of bronchial cancer |
1. Compression of recurrent pharyngeal nerve (left only) => hoarseness of voice 2. Damage to sympathetic trunk => Horner's syndrome 3. SVC obstruction (right only) 4. Metastasis to the brain => Dizziness, seizure 5. Metastasis to the bone => Bone fracture, bone pain 6. Metastasis to the liver => Jaundice, liver failure 7. Ectopic production of PTH => Fracture and osteoporosis 8. Ectopic production of ADH => Hypertension 9. Ectopic production of ACTH => Cushing's syndrome |
|
|
Name three common places where lung cancer tend to metastasise |
Lymph nodes Brain Bone Liver Adrenal gland |
|
|
Name four features of Horner's syndrome. What is it indicative of? |
Miosis (a constricted pupil) Ptosis (a weak, droopy eyelid) Apparent enophthalmus (inset eyeball) Anhidrosis (decreased sweating) Indicative of Pancoast tumour |
|
|
Name three hormones that can be ectopically secreted by lung cancers. For each of them state whether they are produced by SCLC or NSCLC |
ADH: SCLC ACTH: SCLC PTH: NSCLC |
|
|
Route of lymph spread of lung cancer |
1. Ipsilateral hilar nodes 2. Ipsilateral mediastinal or subcarinal nodes 3. Contralateral, scalene orsupraclavicular lymph nodes |
|
|
Name the main and two secondary risk factors for lung cancer |
Primary: smoking Secondhand smoking Previous history of cancer Age COPD Exposure to asbestos Exposure to radon Exposure to radiations |
|
|
A retired non-smoker miner present with lung cancer. What is the likely cause of his cancer? |
Exposure to asbestos |
|
|
What two abnormal components can we find in alveoli of a patient with pneumonia? |
Exudate WBC |
|
|
A patient present with symptoms of pneumonia. What is the expected observations on spirometry and blood gas? |
V/Q ➘➘ ⇒ Hypoxaemia PCO2 normal |
|
|
A patient present with symptoms of pneumonia and has restricted respiratory movements. Why? |
Because of the pleural pain or pleural effusion |
|
|
Name 3 risk factors for community-acquired pneumonia |
Age: especially infants, young children and the elderly. Smoking Alcohol Preceding viral infections (e.g. influenza) Asthma COPD Malignancy Bronchiectasis Cystic fibrosis Immunosuppression |
|
|
Incidence of community-acquired pneumonia in UK |
0.5%-1% |
|
|
Name 2 common causes of bacterial pneumonia |
S. pneumoniae S. aureus Haemophilus influenzae Mycoplasma pneumoniae Chlamydophila pneumoniae |
|
|
Five common viruses that may cause pneumonia |
Respiratory viruses (CAPRI) Coronavirus Adenovirus Parainfluenza Rhinovirus Influenza (most likely) |
|
|
Two risk factors for TB |
Resident of southern countryImmunocompromised patients (e.g. AIDS) |
|
|
Define bronchiectasis |
Abnormal widening of the bronchi or their branches, causing a risk of infection. |
|
|
What gender is most likely to have small-cell carcinoma? |
Female smokers |
|
|
Pathophysiology of cystic fibrosis |
Autosomal recessive disorder: mutation of the CFTR gene affecting chloride and sodium transport ⇒ All exocrine glands are affected |
|
|
What organ is most affected by cystic fibrosis |
Pancreas |
|
|
A patient with a family history of pancreatic disorder presents with productive cough. What is happening? |
Cystic fibrosis: Hypertrophied mucous glands in the lungs ⇒ Excessive secretion ⇒ Plugging of airways ⇒ Chronic infections and productive cough
|
|
|
Name three consequences of CO2 retention |
Mechanism: PCO2 ➚ ⇒ Cerebral vasodilation ⇒ Increased cerebral blood flow Consequences: headache, raised CSF pressure, papilloedema, asterixis |
|
|
Outline the mechanism of acute respiratory distress syndrome (ARDS) |
Trauma or sepsis ⇒ Widespread inflammation in the vasculature of the lung ⇒ Destruction of the lung parenchyma, surfactant loss leading to increased surface tension in the lung, fluid accumulation in the lung, and excessive fibrous connective tissue formation |
|
|
Name three consequences of ARDS |
Alveolar oedema with high protein concentrations (reflecting damage) Areas of collapse RR ➚ Arterial PO2 ➘ Lung compliance ➘ (fibrosis) FRC ➘ CXR: opacity |
|
|
Outline the mechanism of infant respiratory distress syndrome (IRDS) |
Absence of surfactants ⇒ Unstable lung, reduced compliance (stiff lung), severe hypoxaemia, pulmonary oedema |
|
|
Relate pulmonary hypertension to heart failure. |
Left heart failure is a possible cause of pulmonary hypertension. Right heart failure is a possible consequence of pulmonary hypertension. |