Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
109 Cards in this Set
- Front
- Back
|
what character bacteria is commonly on the skin?
|
G+
|
|
|
what character bacteria is commonly in the GI?
|
G-
|
|
|
PCNs are bacterial_____
|
cidal
|
|
|
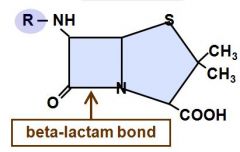
which component of PCN binds to PBP?
|
b-lactam ring
|
|
|
Be able to Identify the structure of a B-lactam and the bond..
|
|
|
|
• The attack point of the beta-lactamases such as penicillinase is the?
|
o B-lactam ring
|
|
|
• Which PCNS are effective with methicillin sensitive staph A (besides methiciliin)
what are they collectively known as? |
o Naf, ox, clox, diclox
Antistaph pens |
|
|
• Which is the drug of choice for MSSA
|
o Nafcillin
|
|
|
• What are the functional Hemoglobins
|
o A and F
|
|
|
• Extended spectrum PCNs that are used for some gram negatives?
|
o Amp and amox
|
|
|
• DOC against listeria
|
o Ampicillin
|
|
|
which of the extended spectrums have better oral availability?
|
amoxicilin
|
|
|
• What are the antipseudomonal PCN
|
o Ticar,piper
|
|
|
• Which gen of ceph has more gram neg cov, 1st or 3rd?
• Better CSF penetration? • More B-lactamase resistance? |
All are 3rd gen
|
|
|
• Name a carbapenem
|
o Imipenem
|
|
|
• Can you use cefipime in a pt who had an anaphylactic rxn to amoxicillin?
|
NO
|
|
|
• Can you use aztreonam in a pt who had an anaphylactic rxn to a penicillin?
|
yes!
|
|
|
What kills almost ALL bacteria?
|
Carbapenem
|
|
|
MOA for carbapenem?
|
similar to cephs
|
|
|
Carbapenems:
Effective against pseudomonas? |
YES
|
|
|
Carbapenems:
o Does it have a significiant post bacterial effect? |
Yes
|
|
|
Carbapenems:
o Is it effective against MRSA? |
NO
|
|
|
Carbapenems:
o Used with this medication to extend duration by blocking action of renal enzymes |
Cilastatin
|
|
|
• Name a monobactam
|
o Aztreonam
|
|
|
• What is a MAGIC bullet for gram negs?
|
o Aztreonam
|
|
|
pt is in ICU for 6 weeks, have a ton of resistance, ton of infections..what do you want to use?
|
this is a resistant G- infection
so Aztreonam |
|
|
Aztreonam:
MOA? |
Only binds PBP in G-
|
|
|
Aztreonam:
o Does it have cross sensitivity with PCN/Cephs? |
NO
|
|
|
• Vancomyicn spectrum limited to?
|
G+
|
|
|
vancomyocin is toxic to what 2 systems?
|
Renal (nephrotoxic)
Auditory (ototoxic) |
|
|
adverse side effect of vancomycin with rapid infusion?
|
Red man syndrome
|
|
|
• What is the drug of choice for methicillin resistant staph A MRSA
|
o Vancomycin
|
|
|
DOC for psuedomembranous colitis?
|
o Metronidozle and Vancomyocin
|
|
|
Bug associated with:
• Southwest Desert |
o Coccidiodes immitis
|
|
|
Bug associated with:
• Cutaneous Lesions |
o Blastomyces dermatites
|
|
|
Bug associated with:
• Neutropenic |
o Aspergillus fumigatus
|
|
|
Bug associated with:
• Ohio River Valley |
o Histoplasma capsulatum
|
|
|
Bug associated with:
• Sporulating Organisms |
o Coccidioides immitis
|
|
|
Bug associated with:
• Filamentous branching hyphae |
o Aspergillus fumigatus
|
|
|
Bug associated with:
• CT “Snowstorm” pattern |
Histoplasma capsulatum
|
|
|
Bug associated with:
Halo Sign |
Aspergillus
|
|
|
Bug associated with:
Slimy black mold? |
o Stachybotrys chartrum
|
|
|
• Evaluation of tumors of specific nerve is best achieved with?
|
MRI- Tissue and nerve
|
|
|
• What makes small cell carcinoma have an increased sensitivity to chemotherapy
|
o Its rapid doubling time
o If something is a slow growing cancer, chemo doesn’t really do much, so this is good for small cell |
|
|
• Why is small cell Ca not amenable to surgery
|
o Metastasizes via blood stream early, 80% disseminated at diagnosis
o So you can’t cut it out before it has already spread like wild |
|
|
• CT suspicious for lung cancer…next step to diagnosis?
|
o Biopsy and bronchoscopy (must do this b4 diagnosing ca)
|
|
|
• What are the associated paraneoplastic syndrome with small cell Ca
|
o SIADH
|
|
|
• Harmatomas are similar to pneumonias or coin lesions on xray?
|
o Single pulmonary nodules (coin lesions)
|
|
|
• Why may an apical lung tumor cause hoarseness
|
o Right recurrent laryngeal nerve
|
|
|
• In TNM classification what does each letter stand for and what must M be to signify stage IV
|
o T- Tumor
o N- Nodes o M- metastitis o M must be at least 1 |
|
|
• Which type of pneumothorax involves a mediastinal shift
|
o Tension
|
|
|
• Trauma, distant heart sounds, in shock describes?
|
o Cardiac tamponade
|
|
|
treatment of cardiac tamponade in order?
|
IV fluids,
O2, pericardiocentesis (drain that fluid) |
|
|
• A pancoast tumor can invade the cervical sympathetic chain and brachial plexus causing what syndrome?
|
Horners
|
|
|
What are the symptoms of Horner's syndrome? what can cause this?
|
Miosis, ptosis, shoulder pain, and motor sensory deficits in the arm
Pancoast tumor |
|
|
what do you suspect if you see a
Milky pleural effusion? Bloody? |
o Milky: Lymphoma
o Bloody: malignancy |
|
|
• 69 y/o male, smoker, with ant chest pain, shocky, and hoarse
|
o Dissecting aortic aneurysm
|
|
|
• Tumors-locations:
o Pleural |
Mesothelioma (fibrous plaques)
|
|
|
• Tumors-locations:
Central |
Sqaumous Cell
Small Cell |
|
|
• Tumors-locations:
Peripheral |
Adenocarcinoma (glands involved)
|
|
|
what type of cancer has ill defined cell boarders?
|
small cell
|
|
|
what type of cancer is Glandular with mucin?
|
o Adenocarcinoma
|
|
|
what type of cancer is Well differentiated, gray-white tissue
|
o Squamous cell
|
|
|
• Which carcinoma is associated with paraneoplastic syndromes (low Na, etc)
|
o Small cell
|
|
|
• Most common syndromes associated with small cell cancer?
|
o SIADH
o Cushings (moon facies, hyper weight gain, hyper cortisol) |
|
|
• Which carcinoma is caused by asbestos
|
o Mesothelioma
|
|
|
• Leading cause of cancer-related deaths
|
o Lung Cancer
|
|
|
Major risk factor of cancer related deaths?
|
Smoking
|
|
|
• Most aggressive cancer?
|
o Small cell
|
|
|
please outline fetal circulation starting with the umbilical vein and finishing at the umbilical arteries
|
Umbilical vein
ductus venosis liver inferior vena cava RA Foramen ovale Latrium Left ventricle Ascending aorta Descending aorta Placenta |
|
|
where does blood go to first in fetal circulation?
|
LIVER
(glucose and AAs for fetus) |
|
|
what part of fetal circulation has the highest concentration of "good stuff"
|
umbilical vein
|
|
|
what causes constriction of the pulmonary arteries?
|
*Acidotic & Hypoxic blood causes Hypoxic Pulmonary Vasoconstriction *
|
|
|
90% of Deoxygenated blood shunts through Prostaglandin induced _____ _____ ______ bypassing pulmonary arteries.
|
Patent Ductus Arteriosus
|
|
|
3 organs with preferred circulation in Fetal Circulation
|
Liver
Heart Brain |
|
|
what gets 1st dibs at O2 rich blood in fetal circulation?
|
coronary arteries
brain gets second dibs |
|
|
o Pathology in meconium aspiration?
|
Chemical irritation
(that is all she said but he asid the fetus gets stressed, hypoxic etc, causing decreased sympathetic tone, leading to pooping the womb. this poo is then inhaled as a chemical irritant, baby comes out looking like shit...hahaha i mean, all blue and having trouble breathing) |
|
|
o When does surfactant production begin?
|
28 weeks
|
|
|
o What initiates surfactant release
|
physical stretch
|
|
|
what stimulates the production of surfactant?
|
cortisol
|
|
|
at what age are lungs matured?
|
34 weeks
|
|
|
• Transient tachypnea of the newborn most common in? why?
|
o C section (no thoracic squeeze)
|
|
|
• Earliest preemie age for longer survival
|
25 weeks
(i remember him saying 23 is when the type I pneumocytes develop, and that is the earliest age...but this is what she said in lecture) |
|
|
o Ground glass X ray in neonate....
|
Hyaline Membrane disease (ugh what is the other name for this respiratory distress syndrome)
|
|
|
o Patchy infiltrate X ray in neonate....
|
Neonatal pneumonia
|
|
|
o Spongy airless area base of left lung on X ray in neonate....?
|
Pulmonary sequestration
|
|
|
• Most common structural lung lesion in neonates?
|
o Congenital lobar emphysema
|
|
|
• Which malacia is mild albeit noisy?
|
o Laryngo
|
|
|
• Conjunctivitis and staccato cough?
tx? |
o Chlamydia (erythromycin/macrolide is Tx)
|
|
|
• Most common neonatal infecting agent?
|
o CMV
|
|
|
• Primary newborn screening for CF?
|
o Immunoreactive trypsinogen
|
|
|
if you screen a kid for CF (using what again?) and it is positive... what do you do next?
|
o Immunoreactive trypsinogen
next step: Refer them to CF center, and get sweat test |
|
|
What is the genetics behind CF?
|
Autosomal recessive
so need to know how to calculate this if they tell you one parent is a carrier etc |
|
|
o Lung transplant parameters?
|
baseline FEV1 < 40% of expected
increasing frequency of severe pulmonary exacerbations requiring hospitalization progressive O2 need emergence of organisms resistant to multiple anti-biotics ok so this was something she said to know...i didn't see it in his handout but this is what i remember from lectuer: it is tough to get a lung transplant, so you want to get on the list early (before you need one) also you can get parts from mom/dad |
|
|
o Most common Bacteria in CF
|
Pseudomonas
|
|
|
Most dangerous bacteria in CF?
|
Burkholderia cepacia
associated with worsening lung function, makes for worse outcome, isolate them from other CF pts because it can rock their shit |
|
|
Kid comes into your office w/ CHRONIC COUGH, APATHETIC, past Hx of SEVERAL INFECTIONS, & is SMALLER than other classmates...what should you do? why
|
o Look at STOOL – check for malabsorption & order SWEAT TEST
they might have CF |
|
|
what is a J receptor? What can be detrimental to its activity? What population is this seen in?
|
J receptor is what senses stretch of the lungs and makes you exhale
RSV can stop this receptor's activity this is seen in kids and can lead to stopping of breathing! |
|
|
Why are neonates more susceptible to O2 toxicity?
|
Premature babies get toxicity from oxygen and inflammation bc they *do not have Free Radical Scavengers* to fight off free radicals
--thus they cannot turn off the inflammatory response |
|
|
what is the most important lung volume?
|
FRC (Functional Residual Volume)
|
|
|
what stops atelectasis besides closely packed alveoli and surfactant?
|
Functional Residual Volume
|
|
|
How do you tx an asthmatic or COPD to get relief? (this had *TQ next to it...which makes me think test question)
|
Restore FRC!
Make it easier for them to breathe. -Giving O₂ doesn’t treat the WOB. Their lungs are already too full (blood, edema,pus, mucus) |
|
|
Please discuss the progression of infant immunity
|
IgG passes from mother to fetus in *3rd Trimester*
-A TERM baby has mom’s immunity for a couple months, it then goes down for a bit while IgG, IgA & IgM are learned |
|
|
Thickened Alveolarmembrane
*Neutrophilic infiltration *Decreases Oxygenation *Increases Work of Breathing describes? |
• Respiratory Distress Syndrome (RDS) or Hyaline Membrane Disease
|
|
|
what is the major problem (cause) of Respiratory Distress Syndrome (RDS) or Hyaline Membrane Disease
|
lack of surfactant leads to alveolar collapse
|
|
|
treatments for RDS? 3
|
1. Perinatal Steroids
2. 4 mL/kg Surfactant injection into Lungs 3. Support (O2, antibiotics….) |
|
|
What is considered a positive sweat test for CF?
|
values of chloride greater than 60 mEq/L
|
|
|
aside from the lungs, what is another major organ that has its function diminished in CF?
|
pancreas
can't secrete as well, and what it does is less effective |
|
|
what can improve digestion and intestinal absorption problems seen in CF?
|
supplemental pancreatic enzyme therapy
|