![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
368 Cards in this Set
- Front
- Back
|
Hypoxia |
Deficiency of Oxygen; inadequate availability of oxygen for cellular function; can result from reduced oxygen content in the air (such as in high altitudes) or from anemia. |
|
|
Hypoxemia |
Deficiency of Oxygen in the blood; diminution of the actual content of oxygen in the blood implies tissue hypoxia |
|
|
the state of matter of a substance depends largely upon... |
its KINETIC ACTIVITY (the motion of the molecules) which in turn depends on the temperature of the molecules = the higher the temperature, the more kinetic energy, the more the molecules are inclined to change states. |
|
|
Absolute Zero |
the temperature at which all molecular activity is ceased = no kinetic energy developed by Kelvin (0K) |
|
|
Melting Point |
temperature at which a solid converts to liquid |
|
|
Freezing Point |
Same as melting point, but the substance if converting from liquid to solid |
|
|
Boiling Point |
temperature at which a liquid turns into a gas at 1ATM (760mmHg) at sea level; temperature at which the Vapor Pressure is equal to Atmospheric Pressure; reducing the pressure above the liquid reduces its boiling point, because the forces opposing the escape of molecules from the liquid are decreased. |
|
|
Sublimation |
temperature at which a solid converts to a gas below the MELTING POINT. = skips melting, skips liquid phase; occurs when the heat content of a substance increases to a point that the molecules in the solid state acquire enough energy to break lose and enter the gas state while remaining below the melting point. |
|
|
Evaporation |
temperature at which a liquid converts to a gas below the boiling point; clinical examples: simple humidifier |
|
|
Vapor Pressure |
A measure of the force that molecules exert as they hit the surface of a liquid and escape into the gaseous phase; The higher the liquid's temperature, the more force is exerted when the molecules hit the surface of the liquid, and the more likely the molecules are to escape. |
|
|
Critical Temperature |
The temperature ABOVE which a gas cannot be converted back to a liquid, no matter how much pressure is exerted upon it. As the temperature of a substance rises above its boiling point towards its critical temperature, the pressure necessary to change it back to a liquid increases proportionately. When the gas surpasses its critical temperature, no amount of pressure will be sufficient to convert it back to a liquid. |
|
|
Critical Pressure |
The pressure required to convert a gas back to a liquid at its critical temperature |
|
|
Characteristics of an Ideal Gas |
1. No energy is lost during molecular collisions (they are completely elastic in nature) 2. The volume of the molecules themselves is negligible (the distance between them is 300 times bigger than the diameter of their molecules) 3. no forces of mutual attraction exist between these molecules; they are always in constant movement. |
|
|
Gas Pressure |
The fore the molecules of a gas exert when they hit a surface/object Can be measured using an Aneroid Barometer or a Mercury Barometer |
|
|
Mercury Barometer |
uses the weight of a column of mercury to equilibrate with the kinetic force of molecules hitting the surface of the mercury reservoir. the pressure of the atmosphere on the mercury reservoir forces the mercury up the vacuum tube a distance equivalent to the force exerted. Height of Hg column represents the downward force of atmospheric pressure. |
|
|
Aneroid Barometer |
measures atmospheric pressure by equilibrating the atmospheric gas pressure with a mechanical force, or the expansion force of an evacuated metal container. when there is an increase in gas pressure, the box is forced to contract; the spring attached to it is pulled down causing the lever to pivot and the indicator moves to a higher value on the pressure scale, A decrease in atmospheric pressure surrounding the box allows it to expand toward its normal shape. |
|

Bourdon Gauge |
easiest to use in the clinical measurement of gas pressure; consists of a semicircular coiled flexible metal tube attached to a gauge that records the degree to which the tube is straightened by the pressure of the gas inside. an increased gas pressure is transmitted up the coiled flattened tube. It tends to rise (straighten) as the surface area on the outer side of the tube is larger than the inner surface. This causes the gearing mechanism to rotate the indicator to a higher point on the pressure gauge. |
|
|
1mmHg = |
1.36 cmH20 |
|
|
Kelvin to Celsius |
C = K - 273 |
|
|
Celsius to Kelvin |
K = C + 273 |
|
|
Fahrenheit to Rankine |
R = F + 460 |
|
|
Rankine to Fahrenheit |
F = R - 460 |
|
|
Boyle's Law |
Absolute Temperature and Mass are constant; Pressure is inversely proportional to Volume; P1V1 = P2V2 |
|
|
Charles' Law |
Pressure and Mass are constant; Volume and Absolute Temperature (K or R) are directly proportional V1/T1=V2/T2 |
|
|
Gay-Lussac's Law |
Volume and Mass are constant; Pressure and Absolute Temperature (K or R) are directly proportional P1/T1=P2/T2 |
|
|
Universal Gas Law |
P1V1/T1=P2V2/T2 |
|
|
Dalton's Law of Partial Pressures |
1. The total pressure of a gaseous mixture is equal to the sum of the partial pressures of each gas that constitutes the mixture 2. The partial pressure of each gas in the mixture is the pressure it would exert if it occupied the entire volume alone 3. The partial pressure exerted by each constituent gas is proportional to its volumetric percentage of the mixture |
|
|
Diffusion |
The net movement of gas molecules, by virtue of their kinetic properties, from an area of high concentration to an area of low concentration; Intermolecular mingling that occurs as a result of molecules randomly bouncing off each other. This produces a homogenous mixture and occurs due to the ideal gas law. |
|
|
Fick's Law |
The rate of diffusion of gases in a gaseous medium is proportional to the gradient of their concentration. The higher the concentration gradient from one area to another, the faster the gas will diffuse. Example: diffusion of carbon dioxide through the croup tent (CO2 tends to flow from the inside of the croup tent, where the patient in breathing, through the tent's micropores towards room air, where the concentration of carbon dioxide is very minimal). |
|
|
Graham's Law |
The rate of diffusion of a gas is inversely proportional to the square root of its density; The lower the density of the gas molecule, the faster it will diffuse. Example: Helium + Oxygen (Helium is lighter than room air - 21% oxygen - so we combine the two gases together to trick the body when the patient's airways are too constricted, to make oxygen reach spaces it could not reach if it were alone). |
|
|
Density |
Mass / Volume Weight / Volume Units: 1. g/cm3 = for solids and liquids 2. g/L = for gases |
|
|
Henry's Law |
The weight of a gas dissolving in a liquid at any given temperature is proportional to the partial pressure of the gas; The higher the partial pressure, the more it will dissolve; Example: when a patient is out of breath and we put him on a mask delivering 100% oxygen, the partial pressure of 100% oxygen will be a lot higher than room air oxygen - 21% - and that will make oxygen be diffused more efficiently through the alveoli). Same with carbon dioxide: carbon dioxide content in room air is very minimal, but in the lungs the partial pressure is way higher, therefore CO2 tends to flow out of the lungs easily. |
|
|
Solubility Coefficient |
measurement of how much of a gas will dissolve per ml/mmHg into a liquid (how much of a gas will dissolve in blood). |
|
|
Solubility Coefficient of Oxygen |
= 0.023 ml/ml of plasma at 37 degrees Celsius, 760mmHg |
|
|
Solubility Coefficient of Carbon Dioxide |
= 0.510 ml/ml of plasma at 37 degrees Celsius, 760mmHg |
|
|
Solubility Coefficient and Density related to Diffusion |
The diffusion of a gas into a liquid medium (like the diffusion of gases into the perfused lung) is DIRECTLY proportional to the solubility coefficient of the gas and INVERSELY proportional to the square root of its density. Whatever the substance, the bigger the solubility coefficient, the easier it will diffuse, The denser the substance, the slower it will diffuse. Because CO2 has such a high solubility coefficient, it is 19 times more diffusible than Oxygen. CO2 can always diffuse into the blood at the alveolar capillary membrane and get out of the lungs. O2 has a much more difficult time leaving the alveoli to get into the capillaries. |
|
|
Flow |
Volume / Time mL/sec L/min Flowmeter = L/min Remember Fick's Law = gas flows from an area of high pressure to an area of low pressure |
|
|
Bernoulli's Principle |
A gas flowing in a tube meets a narrowing/restriction. The molecules speed up with increasing forward velocity so that the same number of molecules can get through in a given amount of time. As a result, the molecules hit the sides of the tube after the restriction less frequently, causing a drop in lateral pressure. This drop in lateral pressure causes a vacuum, or sucking action, that can be used to entrain additional gas or liquid to be delivered to the patient. |
|
|
Jet |
Commonly found in many respiratory care equipment; Simple application of Bernoulli's principle; We can entrain air in for increased flow (used in Venturi masks or ventilators) or we can entrain water (as in nebulizers) |
|
|
Factors that affect the degrees of fluid or air entrainment by a jet |
1. JET ORIFICE SIZE: the smaller the orifice, the higher the forward velocity, the larger the drop in pressure, the more air can be entrained, decreased FiO2 (fractional inspired oxygen) 2. SIZE OF THE ENTRAINMENT PORT: the larger the port size, the more air can be entrained, decreased FiO2. |
|
|
Venturi Principle |
Based on Bernoulli's principle; states that the lateral pressure drop as fluid flows through the restriction can be restored to the pre-constriction pressure if a gradual dilation occurs in the tube distal to the constriction. The gradual dilation of the tube must have an angle of divergence that is less or equal to 15 degrees. The addition of a tube gradually increasing in diameter in the direction of flow from the jet orifice will restore the lateral pressure of the gas toward pre restriction pressure. This is critical in devices such as ventilators. |
|
|
Moles |
All matter is composed of atoms. A molecule is the smallest particle of a substance that retains all of its properties. 1 gram atomic weight = 1 gram molecular weight = 1 gram formula weight (ionic compounds) = 1 mole (any quantity of matter that contains 6.02 x 10 to the 23rd power atoms) |
|
|
Avogadro's Law |
States that equal volumes of gases under the same conditions (T and P) must contain the same number of molecules. At constant temperature and pressure, 1 mole of a gas should occupy the same volume as 1 mole of any other gas. This ideal volume = molar volume. At standard T (O degrees Celsius) and pressure (760mmHg), dry (STPD) the ideal molar volume of any gas is 22.4L. These values are used to calculate gas densities and convert dissolved gas volumes into moles per liter. Remember Density: weight/volume => in order to compare gases we examine their mass at equal volumes (gmw/22.4L) |
|
|
Specific Gravity |
Comparison of gas densities Refers to the ratio of the density of one fluid compared to the density of another reference substance, usually water. The specific gravity of gases can also be measured. In this case, Oxygen or Hydrogen is used as a standard instead of water. Example: comparing the densities of Oxygen and Room air, Oxygen is 1.12 times heavier than room air (21% oxygen). Croup tent: Oxygen being heavier than room air, when we analyze oxygen we should always place the sensor as close to the patient as possible (where 100% oxygen is settling). |
|
|
Viscosity |
The thickness of a gas/fluid; determined by: 1. Density (increased density, increased viscosity) 2. Frictional Resistance (water has decreased frictional resistance compared to blood - full of protein and other cells that increases its viscosity - in the body) 3. Temperature (increased temperature, decreased viscosity) |
|
|
Clinical Example of Viscosity |
CONGESTIVE HEART FAILURE (CHF) AND CARDIOGENIC HYPOXIA: decreased muscular pumping ability of the left ventricle leads to an increased viscosity of the end systolic volume (blood left in the ventricle after systole). This thickened blood is much more difficult to pump out of the left ventricle, resulting in poor perfusion (blood flow) to the extremities. This will lead to tissue hypoxia (Cardiogenic Hypoxia = hypoxia with origin in the heart not being able to function as pump efficiently). |
|
|
Poiseuille's Law |
The resistance or pressure gradient to fluid flow through a tube is directly proportional to the length of the tube, flow and viscosity of the fluid and inversely proportional to the radius to the 4th power. R = V (flow) / R(4th) Assumes the flow is laminar (see patterns of flow) |
|
|
Bronchoconstriction |
Smooth muscle surrounding the airways gets irritated and constricts; Example: Asthma, chemical allergies, obstruction due to foreign body |
|
|
Bronchodilation |
Relaxation of the smooth muscles surrounding the airways causes dilation; needs drugs for it to happen |
|
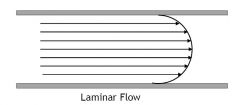
Laminar Flow |
Smooth; fluid flows in streamlines; associated with the movement of fluids through tubes of fixed radii and smooth walls/surfaces Requires far less pressure and resistance than turbulent flow does to move gas through the airways |
|

Turbulent Flow |
Movement of fluid is chaotic; likely to happen when airways bifurcate (branch) Fluid flow becomes turbulent when the velocity at which the liquid/gas molecules are traveling increases sharply. Several other factors can produce turbulent flow such as density and viscosity of the gas or in the radius of a tube. |
|
|
Transitional/Tracheobronchial Flow |
Combination of laminar and turbulent flow. Airways that are making the transition from laminar to turbulent flow are said to have transitional flow. |
|
|
Reynold's Number |
The change in pattern of flow (laminar to turbulent) depends on several factors, including fluid density (d), fluid viscosity (n), linear velocity (v) and tube radius (r). In combination these factors determine Reynold's Number: RN= v X d X (2r/n) If number is less than 2000 = laminar flow If number is more than 2000 = turbulent flow |
|
|
STPD |
Standard Temperature, Pressure Dry; volume of dry gas (water vapor removed) at O degrees Celsius, 1 ATM (760mmHg); used to calibrate equipment |
|
|
BTPS |
Body Temperature, Pressure Saturated; volume of gas with water vapor present, 37 degrees Celsius (body temp), ambient environmental pressure (pressure standard can change according to the weather) |
|
|
Absolute Humidity |
the maximum content or actual weight of water in the air in a given volume at a specific temperature (Mosby: actual content of water present in a given volume of gas - g/m3 or mg/L) |
|
|
Relative Humidity |
CONTENT/CAPACITY; Actual amount of water in the air / the maximal amount of water the air could hold at that temperature If temperature is increased, there is an increased capacity of the gas to hold water due to greater kinetic motion. There is also an increase in partial pressure and greater ability for molecules to escape into the gaseous phase. |
|
|
Body Humidity |
37 degrees Celsius; 44 mg/L (or 43.8 mg/L - absolute humidity) 47 mmHg (water vapor pressure) Mosby, pg 160 example: person breathing room air (22 degrees Celsius, RH = 50%, absolute humidity = 10mg/L). As the inspired gas enters the nose, it is warmed by convection and picks up humidity (water vapor) from the moist mucosal lining by evaporation (cools the mucosal surface). Around the nasopharynx and oropharynx temperature is increased to 30 degrees Celsius, relative humidity of about 95%, Absolute Humidity 30mg/L. By the time air gets to the carina (bifurcation of the bronchi), temperature is 37 degrees Celsius, 100% body humidity, absolute humidity 44 mg/L (Isothermic Saturation Boundary) |
|
|
Regulating Agencies |
Make the laws; Federal, State and local bodies with the right to regulate (pass laws). These agencies often use standards prepared by recommending bodies. An example would be a local county government that adopts standards for the storage of bulk Oxygen established by the National Fire Protection Association (state of PA, for example) |
|
|
Recommending Agencies |
Individuals with technical knowledge that recommend standards for equipment or products. For example, Compressed Gas Association (CGA) made up of equipment, container and valve manufacturers recommends the conditions and ways their products should be used Other examples: AARC, NBRC |
|
|
ICC / DOT |
Regulating Bodies; ICC = Interstate Commerce Commission; regulated the construction, transportation and testing of compressed gas cylinders from 1948 to 1970. DOT = Department of Transportation; took over the ICC job in 1970 and continues to do it. |
|
|
HHS |
Regulating Agency; Department of Health and Human Services; A division of this that affects our practice is the FDA (Food and Drug Administration), which regulates the purity of medical gases. The Bureau of Medical Devices (est. 1976) sets the standards for medical devices so that they can be safely sold in the market. |
|
|
OSHA |
Regulating Agency; Occupational Safety and Health Administration; is a division of the Department of Labor, which regulates safety in the work place. Occupational lung diseases are a major cause of disability in the United States. |
|
|
US PHARMACOPOEIA |
Regulating Agency; A very long series of books containing all the drugs currently available in the US, their strengths, purity and directions for making them (now all online) Revised by Physicians, Pharmacists and other scientists every 5 years. It is the legal standard for drugs in the US In the hospital we use PDR (Physician's Desk Reference) to look up questions about drugs. |
|
|
Compressed Gas Association (CGA) |
Recommending Agency; Recommends the conditions and ways that their products should be used (made up of equipment, container, and valve manufacturers). |
|
|
National Fire Protection Association (NFPA) |
Recommending Agency; sets the standards for the storage of all flammable and oxidizing gases |
|
|
Z-79 of ANSI (American National Standards Institute) |
Recommending Agency; This committee, the Anesthesia and Ventilatory Standards group, reviews and evaluates all anesthesia and respiratory care equipment on the market (we can see the mark on equipments that passed their tests). |
|
|
3 Categories of Medical Gases |
1. Laboratory Gases: have limited therapeutic use; non-flammable; examples: CO2, He, N2 2. Therapeutic Gases: all these gases support combustion (oxidizers - will feed a fire once it is going); examples: room air (N2-O2), Heliox (He-O2), Carbogen (CO2 - O2), and O2. 3. Anesthetic Gases: gases that are used to put the patient to sleep; examples: cyclopropane and ethylene (flammable), N2O (nitrous oxide - oxidizer) |
|
|
Cracking a Cylinder |
We crack a cylinder to get rid of any oil or debris in the valve and to prevent O2 from feeding an ongoing fire (because oxygen is an oxidizer, it will react with oils, debris, grease and other combustible materials if a fire is going on). When in doubt => crack the cylinder: if finding a cylinder that you do not know the history, crack it. |
|
|
Full Cylinder (H or E) |
2200 - 2400 pounds per square inch gauge (psig) |
|
|
Bleeding |
We bleed the regulator to relieve pressure in the spring in the reducing valve to preserve it. 1. Turn off the flowmeter 2. Turn off the tank 3. Turn on the flowmeter, bleed it, turn it off (reduces the pressure on the spring). |
|
|
Function of the Washer in the E Cylinder Regulator (PISS) |

The plastic washer is leveled with the gas outlet, and when securely tightened it prevents leaks. |
|
|
3 Hazards of Compressed Gases |
1. If safety cap isn't on, the valve can be damaged and the tank becomes a missile 2. gases can burst into flames (flammable) 3. gases can feed combustion (oxidizers) |
|
|
Where should cylinders be placed in the office or at home? |
Cylinders should be stored in a cool and dry place, away from any source of heat. |
|
|
What should be done in the event of a severe compressed gas leak? |
We must first make sure the patient is safe (remove patient from the room). After attending to the patient, take the necessary measures to fix the leak. |
|

Cylinder Markings |
1. ICC or DOT (regulating bodies - ICC from 1948 to 1970, DOT from 1970 to present) 2. 3A or 3AA: Type of steel the tank is made of (3A = High Carbon or Medium Manganese steel; 3AA = Chrome-Molybdenum - CrMo; could say spun as well; heat treated steel, superior quality than 3A, more common; 3AL = Aluminum, more recent; Spun/Punch Pressed = the way they are made) 3. Maximum Working Pressure / Service Pressure: the filling pressure that can be exceeded legally by 10% by the manufacturer. It is read in psig (2000 - what the label says - X 10% = 2200 - what the cylinder actually has) 4. Cylinder Size and Serial Number: cylinders are given a letter designation according to their size (A-E are small cylinders most often used as anesthetic gases or portable oxygen supplies, use a yolk regulator - PISS. F-K cylinders are the larger cylinders used as part of the bulk delivery systems of hospitals, use the ASS regulator with threaded outlet. 5. Company that owns and/or manufactures the cylinder, Inspecting Authority: It may be almost impossible to distinguish the manufacturer from the owner or they may be one in the same. Inspectors each have their own brand. 6. Original Safety Test (Hydrostatic) Date and Subsequent Retests: Before 1970, required retest every 5 years, after 1970 retest every 10 years. The DOT requires that each cylinder be tested for leaks, expansion, and wall stress. EE = elastic expansion (cylinder is heated and cooled to certain temperatures and their expansion/contraction is recorded). The oldest test date is the Original Safety Test Date. 7. Label/Color of Cylinders: the label identifying the contents and the concentration of medical gases is more important than the color (tanks can be repainted over the years, so always look at the label first) |
|
|
Green Tank (White internationally) |
Oxygen |
|
|
Gray Tank |
Carbon Dioxide |
|
|
Brown Tank |
Helium |
|
|
Red Tank |
Ethylene |
|
|
Light Blue |
N20 (Nitrous Oxide) |
|
|
Orange Tank |
Cyclopropane |
|
|
Yellow Tank |
Air; but could be Nitrogen |
|
|
Black Tank |
N2, Nitrogen; could be yellow |
|
|
Gray Green Tank |
Carbogen (CO2 + O2) |
|
|
Brown Green Tank |
Helox (He + O2) |
|
|
2 Types of Cylinder Valves |
1. Direct Acting Valve: sophisticated needle valve with two washers and Teflon packing to prevent leaks; capable of withstanding HIGH PRESSURES (more or equal to 1500 psig), therefore cylinders holding gases such as Oxygen or Helium use this type of valve. 2. Diaphragm Valve: stem is separated from the seat by a spring and two diaphragms. As the valve seat does not turn, there is no metal scoring, so no leaks. Used for LOW PRESSURE GASES (less than 1500 psig) with a vapor phase such as a flammable anesthetic or CO2. |
|
|
Pressure in Vapor Gas Cylinder |
At room temperature, 22 degrees Celsius, cylinder pressures for vaporous gases are higher than for liquid gases. The pressure in a vapor gas cylinder represents the force required to squeeze a given volume of gas into the cylinder. In gas cylinders, the volume of gas left in the cylinder is constantly decreasing as is the pressure. |
|
|
Pressure in a Liquid Gas Cylinder |
It is the vapor pressure of the gas over the surface of a given weight of liquid poured into a closed container. In liquid gas cylinders, we see that for a long time the pressure in the cylinder does not change even as gas is used up. This is because the liquid gas is constantly being converted to vapor gas (because of that the regulator shows pressure remaining the same). Only when the liquid gas is gone does the regulator pressure begin to decrease constantly as it did for the vapor gas. |
|
|
Duration of flow |
Duration of Flow (min) = PSIG X Factor / flow going to patient (L/m) Factor: - E Cylinder = 0.28 or 0.3 - H Cylinder = 3.14 or 3 Divide result by 60 to get it in hours. |
|
|
Clinical Importance of Measuring Cylinder Contents and Duration of Flow |
Oxygen X CO2 = Remember that whether a gas is a vapor or a liquid at room temperature is dependent upon its critical temperature and pressure. Beware a fault sense of security with liquid gases. Commercial gas cylinders have calibrations recorder in the English System (PSIG), but once the therapeutic gases leave the regulator, flow is measured in the metric system (L/min) What to tell the nurse: When the gauge reads 500 psig, call me! |
|
|
Bulk Oxygen Systems |
Any system that has 20,000 cubic feet of gas ready for use or 25,000 cubic feet of gas in unconnected reserves; A "central supply" or "piped in" system means there is an Oxygen outlet at each patient bedside. Pressure reduction to 50 psig (working pressure) is accomplished at a central station, and then Oxygen is pumped to each clinical area. This is obviously much easier than changing tanks all the time. |
|
|
Gaseous Bulk Oxygen System |
Standard H cylinders tied together by a manifold which converts individual units into one continuous supply. The manifold mechanism has a pressure reducing valve, a check valve to prevent back flow, a flow control and alarm system to warn of malfunction or depletion. These gaseous bulk systems can be either permanently fixed cylinders or trailer units. |
|
|
Liquid Bulk Oxygen Systems |
The most economical way of transporting and storing Oxygen; 1 cubic feet of liquid oxygen = 860.6 cubic feet of gaseous oxygen at ambient T and P. Remember Oxygen critical temperature = -119 degrees Celsius (-181.1F) and boiling point = -183 degrees Celsius (-297.3F). To prevent liquid from converting to gas both supply trucks and hospital stations are designed like large thermos bottles. There are two layers of steel with a vacuum between them that prevents transfer of heat. Two types of liquid bulk systems: 1. liquid cylinders connected with a manifold 2. a fixed station thermos bottle with 130,000 cubic feet capacity. Liquid is converted to a gas using a heating unit called a Vaporizer. |
|
|
STEPS FOR THE COMMERCIAL FRACTIONAL DiSTILLATION OF OXYGEN |
1. Air is dried and filtered of debris via scrubbers and then cooled near freezing, to remove water vapor (room air is pulled into the fractional distillation plants and large filters that clean up the air) 2. Air is compressed to 200 ATM (increased pressure causes increased temperature - Gay Lussac) 3. The compressed gas is then cooled again, to room temperature this time. The compressed gas is then expanded to 5ATM (decreased pressure, decreased temperature) - also, gas goes through coils that cool it down, like in a refrigerator. 4. When expanding and compressing, we end up with liquid air. Liquid air is obtained (N2+O2); the great drop in pressure (from 200 to 5ATM) puts air below critical temperature and all gases turn to liquid. 5. Liquid air is brought to the distilling column and warmed to boil off the unwanted gases (air is heated to just below the boiling point of Oxygen; Nitrogen is evaporated off the mixture). 6. The distillation process is repeated until 99% pure oxygen is obtained. 7. Pure Oxygen is then placed in liquid storage or as gas in cylinders for delivery to health care facilities. |
|
|
Safety Indexed Connector System |
prevents human error; the purpose of these safety systems is to make only correct connections between the cylinders and the delivery systems. |
|
|
American Standard System (ASS) |

- For H and K systems - 3 parts: Hex nut (with internal/external threads), nipple, outlet - the gas channel through their nipple (on regulator) is aligned with the channel through the threaded outlet (in the valve). The two parts are held together with a wrench tightened HEXAGONAL NUT (hex nut) - 4 divisions of this system: Internal/External Threads; Right/Left Handed Threads - Every medical gas has a distinct combination of this system. |
|
|
PIN INDEX SAFETY SYSTEM (PISS) |

- For small cylinders (aa-E) - Yoke connection - This system was first designed for anesthesia machines, where fixed yokes were attached to the internal gas circuitry. - This design is to prevent the wrong cylinder of medical gas from being attached to the wrong yoke. - There are 6 different positions of pins located in the yoke with the corresponding holes drilled into the valve face of the medical gas. Each gas has 2 pin positions. Oxygen: 2 and 5 - Rubber washer: necessary in this system to prevent leaks - Parts: Yoke, pin position, screw, washer |
|
|
DIAMETER INDEX SAFETY SYSTEM (DISS) |
- Low pressure safety system (designed for use with less than 200 psig, after a reducing valve for example). - Mostly seen used in flowmeters and regulators after the reducing valve - Each medical gas has its own specific threaded connector that cannot be interchanged with other gases. |
|

Quick Connects |
- the connectors for each medical gas have their own specific shapes (circles, squares, diagonals) that will fit only into those shapes on the wall outlet. - This system is used for wall flowmeters and psig of less than 50. - Different companies, different connections. - NCG (squares, circles, diagonals); Shrader (male/female connections); DISS (Hex nut); Ohio (twist and unlock) |
|
|
REDUCING VALVE |
Device that reduces pressure from a high value to a lower one. The reducing valves we work with normally change 2200-2400 psig (oxygen tanks) to 50 psig (working pressure). |
|
|
FLOWMETER |
A device that adjusts the flow of gas in L/m after the pressure has already been reduced (by the reducing valve on the regulator or on the manifold bulk O2 system). |
|
|
REGULATOR |
A device with a reducing valve and a flowmeter; The reducing valve is decreasing pressure in psig (English System) while the flowmeter reads flow (volume/time) in liters per minute (metric system) |
|
|
HOW A REDUCING VALVE WORKS |
FROM NOTES: The two foces that interact are spring tension and gas pressure. As gas pressure at the bottom drops, the spring tension becomes the dominant force. It pushes the diaphragm downward opening the poppet valve (valve stem). When the poppet valve open, gas flows into the bottom chamber of the reducing valve. Gas continues to flow in until the pressure rise equals the spring tension. The diaphragm will then be straightened out and the poppet valve will close. All reducing valves have a popoff valve also, to vent excessive pressure to the atmosphere if debris or other malfunctions cause a pressure buildup. MY VERSION: Gas comes in through the inlet and reaches the cylinder gauge that tells us how much pressure there is in the tank in pounds per square inch gauge. Gas then flows into the central chamber that contains the poppet valve (which is open at this time), the diaphragm and the spring. Gas fills up the upper chamber (high pressure chamber) and forces the diaphragm down, straightening and closing the poppet valve. When the pressure in the upper chamber straightens the diaphragm, pressure in the upper chamber is equal to pressure on the spring (which is pushing upwards from the bottom). Meanwhile, gas is flowing out the outlet into the flowmeter. The pressure in the upper chamber drops, the diaphragm expands back its curve and pushes the poppet valve up to let more gas in. |
|
|
Trace the flow of gas in and out of a reducing valve and what happens inside: |
Gas comes in through the inlet and reaches the pressure gauge, that tells us how much pressure is in the cylinder in pounds per square inch gauge. Gas then flows into the central chamber of the reducing valve, which contains the diaphragm, the poppet valve (which is open at this time) and the spring. Gas fills up the upper chamber (high pressure chamber)and forces the diaphragm, straightening it and closing the poppet valve. When the diaphragm is straightened, pressure on the upper chamber is equal to the pressure on the spring pushing upwards from the bottom. Meanwhile, gas flows out the outlet and into the flowmeter, that reads the flow is liters per minute. The pressure on the upper chamber is reduced as gas flows out, the diaphragm then expands back its curve, opening the poppet valve to allow for more gas to enter the central chamber. |
|
|
Types of Regulators |
1) PRESET: the most common in the hospital practice; preset to 50 psig; the poppet valve opens until 50 psig is achieved and then closes. 2) ADJUSTABLE: These have a key or threaded hand control on the reducing valve face, which allows adjustment of pressure on the diaphragm (up to 100 psig). These regulators permit a wide range of flow and pressure to be achieved. All Bourdon regulators are adjustable. The Bourdon is actually a low-pressure regulator that has one gauge for pressure and another that converts pressure to flow. 3) MULTIPLE STAGE REGULATOR: accomplishes pressure reduction in two or three stages for precision in flow control. Used in industry, not in the hospital. The number of stages is equal to the number of popoff valves present (we cannot always see them). - Which stage has the highest pressure? First stage - thicker spring and diaphragm |
|
|
Reducing Valve in Bulk Oxygen Systems |
a reducing valve is incorporated after the vaporizer to reduce pressure to 50 psig. |
|
|
Pressure Relief Valves |
Located on the valves of the cylinder; Designed to relief pressure in case it builds up inside to an unsafe level; 3 Types: 1. Rupture Disk: a thin metal disk that ruptures or buckles when the pressure inside the cylinder exceeds a certain predetermined limit. 2. Fusible Plug: made of a metal alloy that melts when the temperature of the gas in the tank exceeds a predetermined temperature (pressure increases, temperature increases). After plug melts, excess pressure is release. 3. Spring-Loaded Devices: most common, most dependable (H cylinder); designed to release excessive cylinder pressure and reseal, preventing further release of gas from cylinder after the cause of the excessive pressure is removed. A metal seal is held in place by an adjustable spring. The amount of pressure required to force the seal open depends on the tension on the spring holding the metal seal in place. |
|
|
BACK PRESSURE |
Back Pressure occurs when there is a pressure drop across a restriction. When we hook up an Oxygen device to a regulator via a flowmeter, back pressure can occur, therefore the liter flow going to the patient would drop. Some of the regulators/flowmeters we work with are affected by back pressure and others are not. |
|
|
BOURDON GAUGE AND BACK PRESSURE |

The Bourdon Gauge is calibrated so that its outlet is open to the atmosphere, therefore every time we hook up an oxygen device we cause back pressure. The gauge reads back pressure, and indicates flow in L/m that is HIGHER than what is actually going to the patient. In addition, if we obstruct the outlet the Bourdon Gauge reads to back pressure, even though no flow is going out to the patient. Bourdon Gauge = reads high, delivers low = it is uncompensated for back pressure |
|
|
UNCOMPENSATED FLOWMETERS AND BACK PRESSURE |
These flowmeters are calibrated in L/m AGAINST atmospheric pressure. The gas flow is regulated by a needle valve upstream (proximal) to the ball/float. The ball/float in the Thorpe tube has two forces working against it: P1 = the flow of gas from the wall or cylinder P2 = gravity pulling on the weight of the ball/float and back pressure. P1 > P2 due to Bernoulli's principle When an oxygen device is attached, there is an increase in back pressure that pushes down on the ball/float recording less gas flow than the patient is actually receiving. Uncompensated Flowmeters = Read low, delivers normal |
|

COMPENSATED FLOWMETERS AND BACK PRESSURE |
These flowmeters are calibrated against 50 psig; The gas flow is regulated by a needle valve DOWNSTREAM (distal) to the ball/float. P1 always = P2 No matter what oxygen device is attached, the flowmeter does not respond to back pressure because it is calibrated at 50 psig, therefore flow going to the patient will be accurate. Compensated Flowmeter = reads normal, delivers normal. |
|
|
State one advantage and one disadvantage of the Bourdon Gauge Regulator |
One advantage of the Bourdon Gauge regulator is that it will read accurately at any position that one might tilt it (recommended for patients that are moving around). One disadvantage is that it is calibrated so that its outlet is open to the atmosphere, which means that every time we attach an oxygen device we cause back pressure. The flow gauge reads this back pressure and indicates flow in liters per minute that is higher than the flow being delivered to the patient. Also, if we obstruct the outlet of the Bourdon Gauge it reads the back pressure even though no flow is going to the patient. |
|
|
Tests to see if a flowmeter is back pressure compensated |
1) Read the label: it will say "pressure compensated" or "calibrated at 50 psig". 2) When plugging the flowmeter to the gas source on the wall, the ball/float will respond by jumping quickly if it is compensated. If it isn't compensated, nothing will happen. 3) Take the flowmeter to Biomed to be taken apart so we can see the location of the needle valve. If the needle valve is upstream it is uncompensated, if it is downstream, it is compensated. |
|
|
Expanded Scale Flowmeters |
Clinically we use these for COPD (Chronic Obstructive Pulmonary Disease)or pediatric/neonatal patients. These scales are easy to adjust when a more precise control of low flow rates is required. Regular Flowmeters: 1-15 L/m High Flow Flowmeters: 1-70 L/m Expanded Scale Flowmeters: 0-4, 0-8, 0-15 L/m Babies may need only 1/8 L/m to 4 L/m COPD patients (emphysema + chronic bronchitis) only need 0-4 L/m. These patients only need a very small amount of oxygen, otherwise they will stop breathing. |
|
|
Air Compressors used in Respiratory Care |
Air compressors draw room air to be compressed. Mosby, pg 71: Compressed air is used to power many respiratory care devices. In many cases, air can be compressed at the point of administration by portable air compressors. Larger portable systems can produce compressed air with a standard working pressure of 50 psig (~3.04 ATM); these units can therefore be used to power devices such as pneumatically powered ventilators. Smaller portable compressors, which are unable to reach these high working pressures, are used for bedside applications (like powering small volume nebulizers). Three types of air compressors are available: PISTON, DIAPHRAGM, AND ROTARY UNITS. |
|
|
AIR COMPRESSORS PISTON |
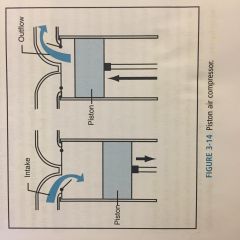
As the piston drops, gas is drawn in through the one intake valve. On the upstroke, the intake valve closes and gas leaves through the outflow valve. Medical air pumping systems use the piston, but its size is limited due to the noise and vibration. Portable examples include the Timemeter. BOYLE'S LAW (less pressure - more volume, more pressure - less volume). If there is a construction going on in the hospital or an old building that has piped-in medical gases (hoses), we may have to shut off oxygen and air outlets and if that is necessary we need to set up air compressors to take over medical air and oxygen cylinders for oxygen. |
|
|
AIR COMPRESSORS DIAPHRAGM |
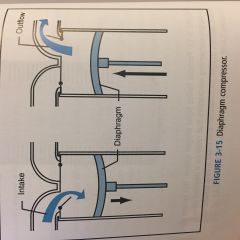
The diaphragm substitutes for the piston. These are used mostly for SMALL PORTABLE MODELS such as the Airshields Diapump or the Devilbiss Nebulizer. Some units combine air compressors and suction. Diaphragm is weaker than the piston, for this reason it is used on smaller devices (O.R., recovery room) Mosby, pg. 71: Diaphragm compressors use a flexible diaphragm attached to a piston to compress gas. As the piston moves down, the diaphragm is bent outward, and gas is drawn through a one-way valve into the cylinder. Upward movement of the piston forces gas out of the cylinder through a separate one-way outflow valve. |
|
|
AIR COMPRESSORS ROTARY |
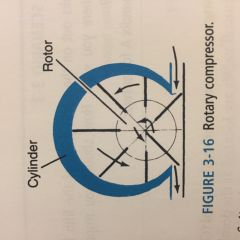
The rotor acts as a fan pushing the air from one area to the other. Examples include ventilators such as the MA 1. It draws air in and spins very quickly, which causes an increased pressure and delivers that to the piece of equipment. |
|
|
OXYGEN CONCENTRATORS |
Mosby pg. 77 Oxygen concentrators are devices that produce enriched oxygen from atmospheric air. They provide an alternative to compressed-air cylinders, particularly in the delivery of respiratory therapy to home care patients. Two types: SEMIPERMEABLE PLASTIC MEMBRANES and MOLECULAR SIEVE. |
|
|
OXYGEN CONCENTRATORS PERMEABLE (SEMIPERMEABLE) PLASTIC MEMBRANES |
These are older models; The membranes are 1um thick, and gases diffuse across them according to their solubility and pressure gradient; A diaphragm compressor provides a constant vacuum across the membrane. Oxygen moves across faster than nitrogen, as a result: 40% oxygen is available at 1-10 L/m; Remember that hospital oxygen is 100%, so a patient going home on this concentrator would have to have their flow increased above hospital level until adequate ABGs (arterial blood gases) are obtained. Increase the flow to deliver closer to 100% oxygen. |
|
|
OXYGEN CONCENTRATORS MOLECULAR SIEVE |
A compressor pumps room air to one of the two sets of sieves. Inorganic Sodium Aluminum Silicate pellets are used to absorb nitrogen from the air while oxygen passes through. The oxygen concentration is flow dependent. At 1-4 L/m the concentrator is able to provide the same ABGs obtained on 100% oxygen at the hospital. Fortunately, 95% of our patients need less or equal to 4 L/m at home. If placed on 10 L/m, the concentrator gives only 50% oxygen. Decrease the flow to provide closer to 100% oxygen. |
|
|
Home Setting Oxygen |
1) Could have a group of cylinders on a cart 2) Liquid oxygen with portable pack 3) Oxygen Concentrator (however, it consumes a lot of energy) |
|
|
Zone Valves and Riser Valves |
We have a liquid gas storage unit, it travels through the hospital floors and every floor has a zone valve (Mosby, 3-19, pg 77) Zone valves are available in order to shut off medical gas in case of an emergency; usually they are located right behind the nurse station. Zone valves must be placed: 1. at the entrance to the hospital 2. at each riser 3. at each branch supplying an area 4. at each operating room In the walls between the floors we have RISER VALVES. Those are used only for maintenance (people who need to take care of them). |
|
|
At hospitals all of our plugs are grounded... |
The principle of the grounding protection method for medical equipment is to provide a low-resistance conductive path that allows most fault current (short-circuit current) to bypass the patient and return to the ground. At hospitals we have normal colored plugs and red colored plugs. Red colored plugs are used for emergencies. If for some reason the electricity in the hospital is out, move all the normal plugs to red plugs (back up emergency generators). In the ICU, we will not have electric beds like other rooms. This is to reduce the amount of electricity around the patient. ICU patients usually have their skin broken multiple times (needle sticks, etc) which increases the amount of exposure to electricity. |
|
|
Physiological effects of electrical current associated with a 1 second external contact with a 110VAC current at 60Hz |
Remember: AMPS KILL, VOLTS DON'T. Amps is what flows through the equipment (and possibly through the patients body), Volts is just the equipment. 500 uA = threshold of perception (when you just start to feel an electrical shock) A little above 10mA = maximum "let go" current - when your reflexes make you withdraw your hand from touching something that shocks you DANGER OF RESPIRATORY PARALYSIS: 1A = danger of ventricular fibrillation 10A = sustained myocardial contraction (followed by normal heart rhythm is current is removed in time) Above 10A = severe burns and physical injury |
|
|
RATIONALE FOR THE USE OF HUMIDIFICATION IN RESPIRATORY CARE |
1. Simples humidifiers are designed to provide enough water vapor to inspired gas to make it comfortable for the patient. 2. Complex humidifiers are designed to provide heated gas at 100% RH at body temperature (37 degrees Celsius); also know as body humidity. This is for critically ill patients, that when intubated have their physiological humidification system bypassed (nose, turbinates, blood vessels that provide filtration, humidification and heating for inspiring gas). |
|
|
FACTORS AFFECTING THE EFFICIENCY OF HUMIDIFIERS |
1. TIME of contact between the gas and water: the longer the gas and water molecules are in contact with each other, the greater the mixing and the more humidity is delivered. High flow - less time for water and gas to spend together, less humidification. 2. The SURFACE AREA involved in the gas/water contact: the greater the surface area of the gas/water interface, the more humidity molecules can push their way into gas mixture. The more small bubbles the diffuser produces, the bigger the surface area (like comparing surface area of elastic arteries and capillaries. There are so many small capillaries, that when adding their cross sections together, they have more surface area than the aorta alone). 3. TEMPERATURE: the greater the temperature, the more humidity molecules can push their way into the gas mixture. Clinical example: simple humidifiers can provide 100% RH at room temperature (22-23 degrees Celsius) but at body temperature that is equivalent to only 1/3 of the RH needed. |
|
|
SIMPLE HUMIDIFIER PASSOVER (BLOWBY) |

Gas passes over the water surface, like an ocean breeze. These are very inefficient due to decreased time and surface area exposure. Clinical examples: old incubators and the Emerson post-op ventilator (original one - looks like a pressure cooker; has an inlet for dry air, an outlet for humidified air; a pressure release valve; water level measurement outside the pan; used a copper pad to filter bacteria from the water+air when it came out to the patient; by heating it he turned it into a complex humidifier). |
|
|
SIMPLE HUMIDIFIER BUBBLE (DIFFUSERS) |

These are the most common type used in respiratory care. Gas is conducted below the water surface through a capillary tube and broken into small bubbles via a diffuser - a specialized stone with multiple micro pores. The bubbles float to the water surface and break, so at this point the gas and the water molecules have mixed. - Not heated; for patients with mild to moderate conditions who only need a little help with humidity. - The more tiny bubbles, the more surface area, the more humidity. - Has a popoff valve: sometimes when we get to a patient's room we might hear it go off because the patient is likely tangled or lying on his/hers tubes. - Small bore tubing Clinical Examples: older non-disposable are Puritan or Ohio Bubblers. Newer disposables include Aquapak 302 (pre filled), Husdon, Bard Parker, OEM. |
|
|
Water used for humidifiers |
We use sterile distilled water, which can be expensive to buy all the time, so now we can just buy pre-filled simple humidifiers for use per patient. How long does it last? It depends on the flow we are using. |
|
|
Important Clinical Points on Humidifiers |
The smaller the bubbles the diffuser produces, increased surface area is produced, increased efficiency of the humidifier. The higher the flow rate used in a Bubble, decreased time gas and water spend together, decreased efficiency of the humidifier. Bubbler humidifiers are dramatically affected by the water level. Decreased water level leads to decreased output due to decreased surface area. |
|
|
To accurately evaluate a humidifier: |
1. Can the unit deliver a high RH and not break down in the clinical environment? 2. At what water level does the efficiency of the unit drop? (how long until we have to change it) 3. Does the unit leak gas, spill or do other things that drive you and the nurses crazy? 4. How much does it cost for what it gives you? (how to get hospital administrators to spend more on equipment? KEEP LAWSUITS AWAY by giving a report on equipment that breaks and could be a problem for the patient's treatment. |
|
|
Heated Humidifiers |
We know that simple humidifiers provide 100% RH at room temperature (22 degrees Celsius), but only 1/3 of body humidity (37 degrees Celsius). In order to provide body humidity we need to turn to COMPLEX HUMIDIFIERS. Normally, our nose with its turbinates supplies a great deal of humidity so that by the time atmospheric gas reaches the tracheal carina, it is 100% RH at 37 degrees Celsius no matter what its starting conditions were. Patients who are intubated (endotracheal tube) or trached (tracheotomy tube) have their upper airway bypassed (that normally does the work of humidifying and heating incoming air). Therefore, therapists must choose appropriate complex humidifiers to replace the upper airway. - increased temperature (sits on a heating platform) - Large Bore Tubing |
|
|
RAIN OUT |
All three factors (TIME, SURFACE AREA, TEMPERATURE) are used to increase the water carrying ability of the gas. As complex humidifiers heat gas to 37 degrees C (compared to room temp 22 degrees C) gas can cool in the delivery tube as it leaves the humidifier on its way to the patient. This causes condensation in low spots and block the tube and gas flow to the patient. |
|
|
COMPLEX HEATED HUMIDIFIERS WICK |

A sponge or hydrophilic paper absorbs water via capillary action. As gas passes over the wick, the water evaporates and humidity is delivered to the patient. Conchapak Aquaterm I, II, and III: A low resistance paper wick is placed inside a metal canister. It is sold with its own gravity feed system and sterile distilled water. Watch out for one way valve. It has a servo-controlled heater and sensing probe, and can be used as a high flow device. As with the Bird, the wick is disposable. Sterile distilled water is gravity fed in the bottom of the canister to wet the wick with a safety overflow on top. |
|
|
COMPLEX HEATED HUMIDIFIERS MODIFIED PASSOVER |
Passover humidifiers that use heat, increased surface area, time and other devices to increase their efficiency. Example: Fisher Paykell |
|
|
COMPLEX HEATED HUMIDIFIERS HME |

Heat Moisture Exchangers or Hygroscopic Moisture Exchangers: used to be called artificial noses; Example: Engstrom Edith, Pall, and Humidivent The patient must have an artificial airway in place; The HME is placed at the patient's wye on the ventilator or via adapter directly on the ETT or trach tube. On exhalation it traps saturated gases and 37 degrees C in its hydrophilic filter. On inhalation, the warm saturated gases are released from the paper back to the patient. In order to use these optimally the patient needs to be well hydrated. These devices are extremely useful in the chronically ill pediatric population with bronchopulmonary displasia (BPD), to increase mobility and a normal lifestyle. When working ideally, these HMEs should be able to recover 70-90% RH from the exhaled gas. Hygroscopic HMEs add a hydrophilic salt (sodium based) to the HME to increase its efficiency. |
|
|
Gravity Feed Systems in Complex Humidifier |
Will drip inside the humidifier (prevents infection); We don't need to open the humidifier to pour more sterile distilled water in it, just switch the bag/container. |
|
|
Servo-Control System |
Our goal is to deliver humidified gas to the patient at body temperature (37 degrees C). The servo control system consists of one proximal probe (near the outlet in the humidifier), one distal probe (near the patient wye - away from humidifier) and a feedback loop. We set the temperature to 37 degrees C (to achieve body humidity), the probes send temperature information to the humidifier constantly so it can get as close to 37 degrees C as possible (it heats up or cools down to maintain the 37 degrees Celsius). |
|
|
Heated Wire System |
- Body Humidity = 37 degrees C - at 1 ATM (760 mmHg) - Humidified gas coming out through the tubing which is standing at room temperature (22 degrees C) tends to cool and loose volume (less temperature, less capacity to carry water vapor) so condensation occurs inside the tubing (rain out). Rain out can cause near drowning or block the flow of gas through the tubing. Because of that we have heated wires inside the large bore tubing. Heated wires heat the gas flowing in the tubes to avoid condensation (rain out) that happens if saturated gas leaves an area of 37 degrees C to an area of 22 degrees C. We use the pigtails to connect the heated wires to an electrical source in the humidifier. Pigtail for inspiratory line will only fit into the inspiratory line; same with expiratory line. - We can use water traps in the inspiratory/expiratory lines to catch the eventual rain out - always put it at the lowest point of the tubing. Book Pg 174, fig 6-21 - When condensate (rain out) forms, the ribs on the large bore tubing catch and hold it, and overflow tends to pool in the tubing. Placement of a trap or drain bag at the lowest point of the circuit prevents condensate from obstructing the tubing. |
|
|
6 factors that affect the FINAL TEMPERATURE of gas delivered to the patient |
FLO LEFT RON TO DATE HENRY 1. FLOW: the higher the flow, the less humidity 2. LENGTH OF TUBING: the longer the tubing, the more the gas is likely to rain out, the less humidity 3. ROOM TEMPERATURE: the room being colder than the humidified gas increases chances for rain out, decreases humidity 4. TEMPERATURE SET ON HUMIDIFIER: 37 degrees C - Body Humidity 5. DENSITY OF THE GAS: Helium X Oxygen - oxygen is denser (the denser the gas, the more humidity it can hold). When going through surgery under anesthesia, they give dry gas for several hours - because anesthetics are so light that they can't keep water vapor molecules up in the air. 6. WATER LEVEL IN THE HUMIDIFIER: humidifier needs to have a certain level of water to function properly, otherwise surface area will not be enough for efficient humidification. |
|

Fisher-Paykel Modified Passover Humidifier |
- air passes over the water surface - IV water bag (gravity feed system) - water drips down straight into the transfer chamber. - How do we control the water level: inside the transfer chamber there are two plastic floats, a blue and a white float. Water drips down, goes into the transfer chamber and the blue float rises. When the transfer chamber is filled to a limit, the blue float has risen to its full position, blocking the water inlet in the transfer chamber and preventing more water from coming in. In case the blue float doesn't work, the white float will prevent the system from floods - will not allow water to come out through the tubes. |
|

Conchapak |
- large water reservoir (gravity feed system) - water drips down (gravity fed) into a tube at the bottom of the reservoir - water travels through the tube and into the canister, forming a 'pond' on the bottom of the canister. The wick gets moistened from capillary action from this water reserve. - dry gas from source comes in through the inlet, pick up moisture from the wick and goes out to the patient. - canister sits on a chamber unit that heats up the canister to 37 degrees C - top tubing of the canister = to stop the canister from flooding - remember to turn the water reservoir to the side before perforating it. |
|
|
Rotometer |
- used to calibrate flowmeters - plug the flowmeter and turn on the flow (2L/m, for example) - small bore tubing connects the flowmeter to the rotometer - the flow in the flowmeter should be the same as the one showing on rotometer |
|
|
How and why is the gravity feed system used in complex humidifiers? |
The gravity feed system stands above the humidifier and has an IV tubing that ends inside the transfer chamber of the humidifier. Water flows through the tubing due to gravity. Inside the transfer we have two floats: a small blue float and a large white float. When the transfer chambers is being filled up with water from the gravity feed system, the blue float rises. When the transfer chamber is filled to its limit, the blue float block rises up to that limit, blocking the inlet for the water and preventing the water from coming in. If the blue float does not work, the white float acts to prevent floods. The gravity feed system is used to prevent infection and contamination that would happen if we had to open the transfer chamber refill with water. If water runs out, we just need to switch the bag. |
|
|
What is "rain out"? How and why are heated wire circuits used with complex humidifiers? |
Rain out is the condensation that happens when the humidified gas flows from a heated environment (inside the transfer chamber, 37C) through the length of the large bore tubing that is standing at room temperature (22-23C). When gas that is heated cools down, it looses its capacity to hold water vapor, and rain out occurs. Heated wire circuits go inside the large bore tubing and they heat up the gas while it is traveling through the tubing, so that the cooler room temperature doesn't cause the humidified gas to condense (rainout). |
|
|
How and why is the servo control system used on complex humidifiers? What are the two types of humidifiers that use servo-control systems? |
The servo control system consists of one proximal probe (measuring temperature in the humidifier), one distal probe (measuring temperature close to the patient - away from the humidifier), and a feedback loop that constantly tells the humidifier to heat up or cool down -according to the information it receives from the two probes - so the humidifier can maintain the originally set temperature (37C - body temperature). Two types of humidifiers that use the servo control system is the Fisher Paykel and the Wick humidifier. |
|
|
How can we tell an HME (Heat Moisture Exchanger) is not adequate humidification for a patient? What type of humidifier should we switch the patient to? |
In order to use an HME, the patient needs to be very well hydrated. If the patient is connected to too many IVs, or if he has a poor skin turgor test, or the patient's secretions are too thick (yellow/green in color) that means he/she is not hydrated enough to provide the humidification needed to use an HME. We should switch the patient to a complex humidifier, that will provide the amount of humidification to meet the patient's demands. |
|
|
Humidity: |
simply water in gas phase |
|
|
Humidifiers put out... |
Molecular Water; Particles can't be seen with the unaided eye. |
|
|
Nebulizers put out... |
Particulate water (aerosol); which are droplets of water suspended in a gas; can be seen with the unaided eye. |
|
|
AEROSOL |
Liquid or solid particles suspended in a gas, providing both humidity and additional liquid applied locally to the airway. |
|
|
Community Acquired Infections |
pulmonary infections, for example, that can be acquired in the neighborhood; not the most serious. |
|
|
Nosocomial Infections |
picked up at hospitals; can kill; either urinary tract infections (UTI) or a respiratory infection (URI - upper respiratory infection); very virulent (potent) - add more days to a patient's hospital stay - cost more money to the hospital. |
|
|
2 ways that aerosols can be measured |
1. Particle size (less than 0.5um - 100um): a major factor in determining how deep into the respiratory tract a particle will land. The stability of a particle is directly related to its size. 2. Total volume output: in cc(ml)/min; The smaller size particles the nebulizer puts out, the lower the total output. This is okay as smaller particles have optimal local effect with minimum systemic side effects, but it is critical when administering a drug. |
|
|
Particle Sizes: |
> 100um: do not enter the respiratory tract 5 - 100um: will deposit in the mouth, nose, and upper airway 2 - 5um: will deposit in the bronchi and bronchioles 0.5 - 2um: can enter the alveoli =0.5um: highly stable, tends to not be deposited (inhaled and exhaled) <0.5: deposited by Brownian Motion (some can deposit, some cannot. not enough deposition as it would happen with 0.5-2um) |
|
|
what size particles will deposit in the upper airways? |
5 - 100um |
|
|
What size particles will be deposited in the bronchi and bronchioles? |
2 - 5um |
|
|
What size particles will reach the alveoli only? |
0.5 - 2um |
|
|
What size particles are so small that they will not deposit but be exhaled? |
0.5um |
|
|
Brownian Motion |
Particles that are less than 0.5 um will deposit by Brownian Motion; Brownian motion means that the smaller the aerosol particles get, the more they resemble the gas molecules hitting them. A particle that is 0.5um is the most stable, it is likely to be inhaled and exhaled without depositing in the airway. The random motion of particles is similar to gas molecules in the air when the particles are smaller than 0.5um. When particles are in random motion they deposit on the lung walls mostly by chance (Brownian Motion). The smaller the particle size, the more vigorous the movement is. Diffusion is the most important mechanism for deposition in small airways and alveoli. |
|
|
6 factors that affect particle deposition |
1. Gravity: Stokes Law states that the rate of sedimentation = density x square of the diameter; the larger particles will be more affected by gravity and will deposit sooner in the respiratory tract; Gases that have a small diameter or low density have a hard time bouncing off and keeping aerosol particles up in a mixture (we have to use them as dry gases - anesthetics for example).
2. Kinetic Activity: particles larger than 0.5um will deposit by gravity and particles smaller than 0.5um will deposit by Brownian Motion
3. Particle Inertia: inertia involves both mass and velocity, so a large particle traveling in a gas stream that changes direction will tend to stay in the original direction and will collide with the airway surface at a bifurcation in a conducting airway; From notes: the greater the particle mass, the more likely it is to be deposited in the upper respiratory tract at a bifurcation in a conducting airway.
4. Physical nature of the particle: - Hygroscopic particles = "water loving"; absorbs water so they increase in size and deposit sooner in the respiratory tract; example: PROPYLENE GLYCOL (antifreeze - very effective in letting drugs dissolve) - isotonic (concentration of salt in the solution is the same as the concentration of salt in the body = osmolarity; 0.9% NaCl is the osmolarity of the body) will deposit easier because it matches the body osmolarity; stable particle size as same osmolarity as the body; Example: normal saline - hypertonic (concentration of salt in the solution is higher than the concentration of salt in the body) patient will cough, there is no deposition; this solution absorbs water and increases particle size, example: Ocean water - hypotonic (concentration of salt in the solution is lower than the concentration of salt in the body), patient will cough, no deposition; lose water to the tissues, decrease size of particles, and travel further down the respiratory tract than expected. Example: distilled water.
5. Temperature and Humidity: the higher the temperature, the more capacity the gas has to carry aerosol, the more humidity.
6. Ventilatory Pattern: ideally, patient should take slow and deep breaths (a tidal volume 2 times the normal Vt), but in the clinical setting that is not possible. A slow flow rate prevents premature deposition of the particles due to gravity, inertia, and increased kinetic motion. In addition, a deeper breath distributes large volumes of gas more uniformly in the lungs due to recruitment of deflated alveoli. It is necessary to talk to the patient and work with him on getting slow deep breaths. |
|
|
Nebulizers: General Characteristics |
Many nebulizers we use clinically use Bernoulli's jet principle: the decrease in lateral pressure and sucking action not only causes air to be entrained but also causes water to be drawn up the capillary tube. The water and gas meet, particles are formed, large particles are baffled and the smallest ones go out to the patient. Nebulizers always have a baffle. Atomizers have no baffle, so large particles fall into the pharynx and nasal cavity. Example: topical anesthetics used for bronchoscopy or decongestants. Any object in the way of particles that converts large particles into small ones is considered a baffle. |
|
Small Volume / Small Reservoir Nebs |
Hand held nebs, used to deliver medication; Clinically called "mini nebs", rain drop nebs, etc; Aerosol masks can be given to patient's with "tremor" problems that cannot hold the mini neb still; Mouth piece can be used for infants too (just put it over the nose and mouth so they can inhale it). Two basic types: 1. SIDESTREAM NEBS, where the aerosol is produced via jet on the side on the main stream of gas, and then the particles float to the main stream to be delivered to the patient; give a lower total output but smaller particles; (A sidestream device has the jet - nebulizer - positioned adjacent to and connected to the main flow of gas. Will generally produce smaller particles because of the longer pathway the aerosol has to travel to reach the main flow of gas.) 2. MAINSTREAM NEBS, where the main flow of gas passes through the solution and helps create aerosol; give a higher total output and larger particles, and are more common in the clinical practice. |
|
|
SideStream Neb |

|
|
|
Mass Median Aerosol Diameter (MMAD) |
This is a concept used in pulmonary system research articles that tries to accurately describe the size of [articles in the clinical environment. Remember the "MEDIAN" is the HALF WAS POINT. This term indicates that in a study, one half of the particles are bigger than the number shown and the other half of the particles is smaller than that number (average size of particles in a study). For example, the label of a nebulizer says it produces MMAD 5um = 50% of the particles will be bigger than 5um, and 50% will be smaller. |
|
|
LARGE VOLUME NEBS WITH AIR ENTRAINMENT |
These large volume nebulizers can hold at least 500 ml (cc) of water. Using the jet principle, they are designed to deliver aerosol to the patient for an extended period. These may be used on post-op patients that have just undergone surgery with dry anesthetic gas. The small volume nebs are used to deliver bronchodilator drugs to patients with airway narrowing, so they last only about 10 minutes. The older large volume nebs are non-disposable (the green one on the picture - ex: Bird, Puritan All Purpose, Ohio Deluxe) and had to be resterilized between patients. The newer large volume nebs are all disposable (ex: Inspiron, Travenol - blue clear one in the picture with donut heater connection on top). One of the goals of large volume nebs is to meet or exceed the patient's inspiratory flow demands. A sick patient can easily breathe 2-3x the normal minute ventilation; the way to meet this demand is through air entrainment. |
|
|
Minute Ventilation |
The volume of gas inhaled/exhaled from a person's lungs per minute. Ve = Tidal Volume (Vt) x Respiratory Rate (f) Average Vt for an adult = 400 - 600ml (500ml) Average RR for an adult - 12 to 20 breaths/min (15b/m) Ve = 500ml x 15 = 7500 ml/min or 7.5L/min (we say a healthy adult's Ve is usually less than 10L/m) Average Vt for pediatric = 5 - 400ml (250ml) Average RR for pediatric = 20 - 30 breaths/min (25b/m) Ve = 250ml x 25 = 6250 ml/min or 6.3 L/m Average Vt for infants = 5 - 50 ml (30 ml) Average RR for infants = 40 - 60 breaths/min (50b/m) Ve = 30ml x 50 = 1500 ml/min or 1.5 L/m If a patient's Ve is not met, the patient will be sucking in room air through the mask's exhalation ports resulting in a decreased FiO2. The best way to meet the patient's Ve and flow demands is by watching to make sure there is ALWAYS LEFTOVER MIST AT THE END OF INSPIRATION. If not, increase the flow! |
|
|
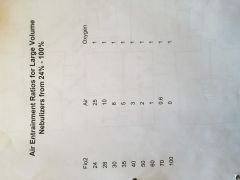
Entrainment ratios for large volume nebulizers |
|
|
|
Hospital Policy on Large Volume Nebs |

Patients that need 50 - 60% FiO2 should have two nebs (both nebs have to be set up with same FiO2 %) Why??? Because patients that need such a high FiO2 are very sick, and one neb only will not be enough to meet their Ve demands. The higher the FiO2, the lower the flow, the thicker the mist (water and gas have more time to spend together and create aerosol - more humidification). |
|
|
Heated Aerosol |
In order to increase the moisture carrying capacities of gas we provide heat via rods, plates, donuts or jelly roll heaters. The immersion rods and plates are hard to sterilize and may be a source of bacterial contamination. They are also inefficient as they heat the entire water source. The donut and jelly roll system only heat the aerosol going to the patient at that instant. Both systems have a metal sleeve incorporated to increase heating. All of these disposable systems have air entrainment from 28 - 100%; however, a drawback is that no heated nebulizer system is servo-controlled, therefore you must place a thermometer near the patient. |
|
|
Nebs as a source of bacterial contamination |
We used to think that since nebulizers put out both particulate and molecular water that bacteria could climb on the larger particles of water and ride into the patient's respiratory tract. In order to prevent nosocomial infections we would change our nebs QOD. Newer research has shown that the patient spewing bacteria into the delivery tubes, not the nebs, may be the real cause. Therefore, we could change our nebs less frequently and save more money. Does not mean we don't need to change it frequently, just less frequently. Which piece of equipment should be changed more often, a humidifier or a nebulizer? NEBULIZER! |
|
|
What is the difference between molecular and particulate water? What type of particles does a humidifier put out? And a nebulizer? What type of device must be changed more often and why? |
Molecular water cannot be seen with the unaided eye. Particulate water is water particles suspended in a gas and can be seen with the unaided eye.
Molecular water is what a humidifier puts out, and particulate water is what a nebulizer puts out.
A nebulizer should be changed most often because the size of the particles created are large enough for bacteria to get attached to and cause cross contamination. |
|
|
How can humidity deficit occur when using a humidifier or a nebulizer? What are the anatomical and physiological consequences of a humidity deficit to the respiratory system? |
Humidity deficit may occur due to inadequate humidification from systemic dehydration or a poorly working humidifier or nebulizer. In order to figure out the humidity deficit caused by a humidifier, we subtract the humidity output from 44mg/L (with the help of biomed). In the clinical environment we look for the increased viscosity of the patient's secretions. If on a simple humidifier the patient presents dry mucus, dry mucous membrane, nose bleeds (patient is inspissated), we need to switch to a complex humidifier to meet the patient's humidity demands. Humidification is important to keep nosocomial infections away, which can lead to a serious pulmonary infection. |
|
|
State Bernoulli's principle and explain how jet nebulizers use this principle: |
Bernoulli's principle states that as a gas that is flowing through a tube meets a restriction, the forward velocity of the molecules increases so more molecules can go through the restriction at a given time. The increase in forward velocity causes a drop in lateral pressure and a suction effect, that can be used to entrain more fluid to the patient. In a jet nebulizer, the decrease in lateral pressure not only causes air to be entrained but also causes water to be drawn up the capillary tube. The gas and the water meet, particles are created and baffled, so the larger ones precipitate and fall back into the water reservoir and only the smallest one go out to the patient. |
|
|
What is the difference between an atomizer and a nebulizer? |
An atomizer does not have a baffle, like nebulizers do. Therefore, the larger size particles that are usually baffled in a nebulizer will end up being delivered to the patient (sizes that deposit on the upper airways = 5-100um). |
|
|
Example of when we use atomizers in respiratory care |
Application of anesthetics to patients that need to be intubated. The larger particles, since not baffled, will deposit sooner in the upper airway by gravity and that prevents the patient's gag reflex to be stimulated while being intubated. |
|
|
Explain why when we move from 24-100% the aerosol density increases, but the aerosol output decreases. Why is this important clinically? |
As the FiO2 increases, the flow decreases, water and gas have more contact time to form particles, so the density (thickness) of the mist increases. Aerosol output decreases because less flow goes through the nebulizer as the entrainment ratios get smaller. This is important because we have to ensure patient safety. When checking on a patient that is on 70% FiO2 (two nebulizers) we should expect to see a dense mist after inhalation. If that is not the picture, there is no mist left after inspiration, we need to make sure the settings of the nebulizers are correct, and if they are, the patient needs more flow (this flow is not meeting the patient's demands). |
|
|
Why do most hospitals have a policy that patients on 50-60% must be set up with two nebulizers wyed together? |
Because at a high FiO2, the flow is not enough to meet the patient's demands with only one nebulizer. By having two nebulizers wyed together we double the flow to meet the patient's demands. |
|
|
What is the difference between a mainstream and a sidestream nebulizer? Which do we use most commonly in the clinical environment? |
Mainstream nebulizers have the jet in the main flow of gas; sidestream nebulizers have the jet on the side of the main flow of gas, so it creates particles that float to the main flow before being delivered to the patient. The most commonly used is the mainstream nebulizer. |
|
|
What solution do we dilute respiratory drugs in and why? |
We use isotonic saline solution to dilute respiratory drugs in, because the salt concentration in this solution is the same as the salt concentration in the body (same osmolarity), therefore there is a better deposition of the particles since the body does not recognize it as foreign. |
|
|
Why do we use sterile distilled water with large volume nebulizers? |
Because it is free of pathogens. |
|
|
Explain what a normal adult minute ventilation is. When we adjust the flow on a patient's large volume nebulizer, what minute ventilation are we aiming for? |
Minute ventilation is the product of Tidal Volume (amount of air we breathe in or out) times the respiratory rate (breaths per minute). The average tidal volume for a healthy adult is 500ml, and the average respiratory rate is 15 breaths/min, which gives an average minute ventilation of 7.5L (or less than 10L/m, which accounts for different tidal volumes and different respiratory rates). When we adjust the flow on a large volume nebulizer, we should aim for 2 to 3 times the normal minute ventilation (we should observe if there is any mist left between breaths; if the mist is completely disappearing the patient needs more flow). |
|
|
What would you do if a patient on a cold large volume nebulizer was wheezing? |
If the patient is wheezing, the cold mist is likely to be irritating the patient's airways. To fix that, we can add a heater to the nebulizer (preferable a heater that heats only the particles going to the patient and not one that heats the entire nebulizer at once - it is more efficient. The newest nebulizers are most likely to heat only the exiting particles (donut heater or jelly rolls). |
|
|
Metered Dose Inhalers MDI's |
In place of mini-neb or small medication neb treatment, these medications are often given. They take less of the therapist's time to administer, but require extensive patient education for proper administration. These small canisters of bronchodilator drugs are measured out in "puffs" of medication. Each puff contains a very exact amount of drug (unit dose). Doctors normally order the MDI as 2 puffs of drug Q4" (every 4 hours). The drug is propelled into the patient's lungs using fluorocarbons as the solvent. These chemicals can cause fatal cardiac arrhythmias if used too often in a short period. Tolerance to the normal dose (TACHYPHILAXIS) can easily develop in users. The proper administration technique is rarely used, so recently "spacers" were developed to help patients with lack of coordination. The spacers allow the patient to squeeze the drug into the bag/container and then breathe in at their own rate and depth. (Spacers allow the patient to breathe at their own rate, tidal volume, and get more of drug - better deposition). To use it we need to shake it really well, because the drug (solute) is dissolved in a solvent (liquid), to make sure we are delivering the drug and not only the liquid. HISTORICALLY... the solvent was Propylene glycol (same family as antifreeze) or Fluorocarbon (used more often, same used in refrigerator coils that cool the air). They were found to cause cardiac arrhythmias because of overuse from patients not knowing how to use the equipment. We now use HFA (Hydrofluoroalkenes) which are similar to fluorocarbons but do not cause cardiac arrhythmias. |
|
|
MDI Categories of Drugs |
1. SYMPATHOMIMETICS (mimics the sympathetic nervous system) to open airways - bronchodilation; example: Albuterol 2. PARASYMPATHOLYTIC (ANTICHOLINERGIC) - inhibits the parasympathetic nervous system; example: Atrovent 3. STEROIDS: corticoids (glucocorticoids); inhibits inflammation, decreases inflammation in the airways, decrease mucosal edema (swelling of the lining of the airway); example: QVAR (beclomethasone) |
|
|
3 Types of MDIs |
1. medicine (solute) dissolved in a liquid (solvent) 2. dry powder 3. combination of drugs (sympathomimetic + parasympatholytic) |
|
|
Explain why we use MDIs and give an example of each type (liquid, dry powder, combination). |
MDIs give a unit dose every time they actuated; they are much more convenient than using a small volume neb, which requires a source of gas to be used; they save the therapist's time as well. Liquid = Albuterol Dry Powder = Advair (steroid + bronchodilator) Combination = two drugs at once (sympathomimetic + anticholinergic or sympathomimetic + steroid); Combivent (albuterol + atrovent = sympathom. + anticholinergic). |
|
|
Explain briefly how bronchodilators work: give an example of a steroid, a sympathomimetic and an anticholinergic (parasympatholytic). |
Bronchodilators act on the smooth muscle that encircles the airways; they relax the smooth muscle allowing for the airway to open, or dilate. Steroid: Qvar (beclomethasone) Sympathomimetic: Albuterol Anticholinergic: Atrovent |
|
|
Why do we have spacers with MDIs? |
To allow the patient to inhale their medication at their own tidal volume, their own pace, so we can have better deposition of particles. |
|
|
What hazards did the old solutions of MDIs have? What have we done to prevent this? |
MDIs used to be dissolved in fluorocarbons or propylene glycol, which causes cardiac arrhythmias due to patient overuse of medication. Now we use hydrofluoroalkenes (HFA) as a solvent, which is very similar to fluorocarbons but do not cause arrhythmias. |
|

Large Volume Nebs II CENTRIFUGAL NEBULIZER |
Like a centrifuge; particles move far away; a spinning disk that rotates on a hollow shaft, water is drawn up the center of the shaft and thrown outward by the centrifugal force through breaker combs (the baffle) = Aerosol is produced. Used in home care; ex.: Devilbiss, Hankescraft; air entrainment is limited. In the home care, it is a large source of bacterial contamination because people don't usually clean them (can be a source of COMMUNITY ACQUIRED INFECTIONS). |
|

Large Volume Nebs III ULTRASONIC NEBULIZER |

These nebs use piezoelectricity as their principle of operation. Electricity passes through a ceramic disk, which changes the shape of the disc and causes it to emit a specific length sound wave (1.35 Mc). This sound wave travels from the disc through tap water in the coupling chamber. The sound wave hits the bottom of the medication cup (which contains isotonic saline and diluted drug inside) and causes a geyser inside. The large particles fall back into the solution while the smaller particles are picked by the source gas (normally room air via blower fan) and taken out to the patient. The frequency of the sound waves determines the particle size (very stable at 3um) while the amplitude control determines the amount of aerosol output. Many models have an indicator to show if the tap water is too low. The whole point of using the ultrasonic nebulizer is that engineers have designed it to create very small particles (2-3um) and they should be able to get to the alveoli. Remember: we cannot change the particle size on this nebulizer, but by changing the amplitude - on the amplitude dial - we can adjust the amount of mist. |
|
|
Troubleshooting the Ultrasonic Nebulizer |
If the neb doesn't work: 1. clean the ceramic disk off with an alcohol prep pad and clean the blower fan filter; 2. check to make sure tap water is in the coupling chamber and there is enough for functioning (and remember, when done using the ultrasonic neb, dump the water and clean everything with alcohol) 3. check electrical connections: WATCH OUT FOR LEAKAGE! (make sure the three prongs are there, especially the ground one!) Clean each unit at the end of the shift! They are an excellent source for nosocomial infections. PSEUDOMONAS ARUGINOSA = grows in all of our respiratory care equipment; when patient is infected - green sputum; virulent organism, very difficult to kill. |
|
|
Explain the Principle of operation of the Centrifugal Nebulizer |
The hollow shaft draws water up from the reservoir, and as the spinning disk spins it creates particulate water. The particles are thrown towards the breaker combs, which baffles the large particles and only the small ones go out to the patient. |
|
|
Explain why Centrifugal Nebulizers may be more dangerous than they look. |
Home care nebulizers are a great source of bacterial contamination because people do not usually clean them properly. This can lead to community acquired infections. |
|
|
Explain in detail: Piezoelectricity and how the ultrasonic nebulizer works. |
The ultrasonic nebulizer contains a piezoelectric ceramic transducer (or ceramic disk) that converts electrical charges it receives into energy. So, the ceramic disk receives electrical charges and changes shape, causing vibrations (sound waves) to be produced that are transmitted through tap water in the coupling chamber to the medication cup. When these waves reach the medication cup, it creates a geyser that sheds aerosol particles. Gas flow is required only to convey aerosol particles from the nebulizer to the patient, and that is achieved by using a built-in fan to direct room air through the nebulizer. |
|
|
What is the function of the coupling chamber? What fluid do we use in it? |
The coupling chamber serves as a transmitter of the vibrations produced by the ceramic disk into the medicine cup. We use tap water, because it is filled with different particles that distilled water does not contain, and those particles assist in transmitting the sound waves to the medicine cup more efficiently. |
|
|
What controls the size of the particles that the ultrasonic neb puts out? What does the amplitude control do? |
The size of the particles produced is set by the manufacturer and cannot be adjusted. What we can control is the rate of aerosol production (amount of mist - thick, thin) which is directly related to the signal's amplitude. So by adjusting the amplitude control, we can adjust the amount of mist produced. |
|

Bleed-in System |
If a patient needs between 21-28% (ex. a BPD child or a COPD adult), we set up a bleed-in system. We run a a nebulizer off room air flowmeter (21% oxygen) or air compressor. In the delivery tube, we cut in an adaptor hooked up to an OXYGEN FLOWMETER. A little further down the delivery tube we cut in another adaptor for the oxygen analyzer. We adjust the oxygen flow and analyze the FiO2 at the patient. Be sure to tape and mark the O2 flowmeter or the nurses will be adjusting it and disturbing the system. |
|
|
Give 3 clinical examples of when a bleed-in system can be used: |
1. COPD (Chronic Obstructive Pulmonary Disease) patients: they need oxygen but we cannot give too much because they might stop breathing 2. Infants that are feeding; 3. Home ventilators: if we need to send someone home on a ventilator, and the patient just needs a small amount of Oxygen. |
|
|
Hypotonic Solution |
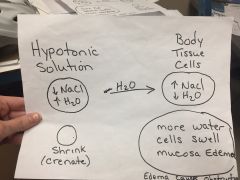
More water than salt; concentration of salt in solution is lower than the concentration of salt in the body; Hypotonic solution will move into the mucosal cells, the mucosa will swell and that is a potential obstruction of the airway Water moves from an area of high concentration to low concentration (of water). |
|
|
Hypertonic Solution |
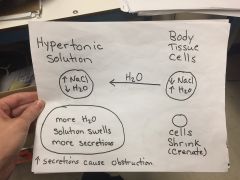
More salt than water; concentration of salt in solution is higher than concentration of salt in the body; Water moves out of the mucosal cells into the airway lumen (causes crenation of the mucosal cells, or shrinking) - bronchorrhea (potential airway obstruction as well). |
|
|
Mucociliary escalator |
The lining of the upper or conducting airways; The mucosa lining in the respiratory tract is uniquely designed to prevent infection from spreading to the lower airways. The epithelium (pseudostratified columnar ciliated) is unique in that it contains cilia that beat in a whipping motion. The epithelium all touch the basement membrane, but they do not all reach the lumen. On top of the cilia there are two layers of mucus. The bottom layer is the SOL, that is secreted by the bronchial glands in the submucosa (thin, watery substance). The top layer is the GEL (thick and viscous), and it is secreted by the goblet cells (wine glass shaped cells that are interspersed in the pseudostratified epithelium). Particles of debris that land in the gel are moved toward the back of the pharynx by the forward whipping motion of the cilia. The top of the cilia just touches the gel layer at the top of their upstroke; this prevents organisms and dirt from infecting the lower respiratory tract. In order for this system to work, drinking and eating enough fluid must properly hydrate the patient. If the mucosal layer becomes inspissated, the cilia will stop beating and the patient will be an easy target for an infection. Once the mucus is dried out, it is much harder for water to repenetrate it so the patient can be rehydrated. Clinical signs of dehydration include loss of turgor of the skin, lethargy and weakness, decreased blood pressure and decreased urine output (I's and O's - input and output). If infection does spread into the alveoli, the pulmonary macrophages will ingest the offending organisms up to a certain level. However, invading organisms can easily overwhelm them. Smoking and alcohol can compromise both the mucociliary escalator and the macrophages. Every time someone smokes a cigarette, the escalator stops for 7 minutes, increasing the risk for a pulmonary infection. |
|
|
CLINICAL USES OF AEROSOL THERAPY |
1. To rehydrate or wet down the respiratory tract postoperatively due to inhalation of dry gas, or from systemic dehydration (we use a large volume neb); 2. To deliver medication to the alveoli to relax the smooth muscle surrounding the bronchioles, thus causing bronchodilation; used to reverse bronchospasm caused by asthma or the aerosol particles themselves (cold aerosol that can irritate the mucosa, in case heating up the aerosol doesn't succeed); we use a small volume neb (isotonic solution + drug); 3. To decrease mucosal edema (swelling) and airway irritation in certain disease states such as croup 4. To thin out bronchial secretions and stimulate cough (mucolytic) |
|
|
CLINICAL HAZARDS OF AEROSOL THERAPY |
1. Bronchospasm can be caused by aerosol particles that we are giving to relieve mucosal edema. Clinical signs of bronchospasm would be wheezing, and we can correct that by heating the aerosol going out to the patient. 2. Bronchodilator drugs given to relieve bronchospasm have their own strong side effects: nausea and vomiting, muscle tremors, tachycardia, nervousness and anxiety. 3. Drug reconcentration, especially if one is using Ultrasonic nebs, can be a THEORETICAL hazard (the saline is nebulized first and then the drug). 4. To thin out secretions and stimulate cough (remember hypertonic and hypotonic solution can cause airway obstruction). 5. Infections can be caused by unclean equipment (nosocomial); most common organism = Pseudomonas aeruginosa = it is gram negative with a stickly sweet smell to the patient's secretions. The mucus is normally a light green color. RT equipment should be cleaned at least once a day. |
|
|
Sputum Induction |
Different hospitals, different ways to do it, BUT: - an ultrasonic nebulizer or a mini neb is used - isotonic, but more often hypertonic or hypotonic solutions are used 3 major types of exams are done on sputum: 1. Bacteriological - culture and sensitivity 2. Bacteriological - gram stain 3. Exfoliative Citology |
|
|
Bacteriological Exam CULTURE AND SENSITIVITY (C&S) |
We examine a sputum smear under the microscope to identify the organisms (culture), and then we determine the antibiotics that are most likely to kill or at least stop it from growing/proliferating (sensitivity) Type of bacteria: cocci, bacillus, spirochete |
|
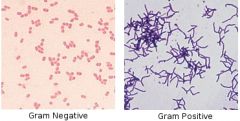
Bacteriological Exam GRAM STAIN |
In the lab or ER we stain first with crystal or gentian violet. The organisms with thick cell walls hang on to this dye even after being washed in alcohol. They are called gram + (positive) organisms. After the violet dye, we wash the slide with isopropyl alcohol and then restain in safranin red. Organisms with a thin cell wall will have it dissolved by the alcohol and pick up the red dye. These are gram - (negative) organisms. The Mycobacterium tuberculosis has its own special stain, carbol-fuchsin, known as the Acid Fast Bacillus (AFB) that uniquely stains the cell wall of this large organism (pink dye) |
|
|
Exfoliative Cytology |
This test depends on the fact that cancerous cells fall off (shed) their tissue more easily than normal cells. This is the same principle of the Pap Smear used to detect cervical cancer. We use this same principle to look for cancerous cells (especially bronchogenic) in sputum smears. |
|

UNINEB |
Small volume neb - 1 dose of drug; can hold ~ 5ml of total solution; 1 treatment takes 10-15 min to give (estimate that we can give 4 treatment in an hour) UNINEB serves as a second line of defense = intermediate size neb that can hold up to 20ml of total solution and are designed to last one hour. It is bigger; same Bernoulli's jet principle (mainstream); According to how sick the patient is, we can give more drug. How much drug to give to the patient? According to patient's size and weight (because someone that is the same age as another person does not mean they get the same dose). |
|
|
Unineb Calculations for 1hr treatment |
Patient A is an adult, we need to give 3ml of albuterol + 500mcg of atrovent (=2.5ml). 1. Add the drugs: 3ml + 2.5ml = 5.5ml TOTAL DRUG 2. Unineb holds 20ml total solution, how much normal saline? 20 ml (TOTAL SOLUTION) - 5.5ml (TOTAL DRUG) = 14.5ml of normal saline |
|

CONTINUOUS NEB |
Really sick patient; 1. decide drug dose (2ml, 3ml, 4ml x hour) 2. how many hours for the continuous neb (2, 3, 4 hours) 3. read the manufacturer's insert that tells the total volume output (25ml/hour, 30ml/hour) |
|
|
Continuous neb calculations |
Doctor tells to give the patient 3ml per hour for 4 hours: 1. total drug going to the patient: 3ml x 4 hours = 12ml of total drug 2. manufacturer's output = 30ml/hour: 30ml x 4 hours = 120ml of total solution 3. 120ml (total solution) - 12ml (total drug) = 108ml of isotonic saline |
|

SPECIALIZED NEB Respiguard |
For pentamidine treatments for HIV+ patients or cancer patients (their immune system is suppressed, they are very susceptible to opportunistic infections such as PCP - PneumocystisCarina Pneumonia - which is very aggressive and we don't know if it is a parasite or a fungus). Typically, once a month the patient will come in to the clinic and first we will give an albuterol treatment to bronchodilate. Second we give the pentamidine treatment (6-8ml of solution made by the pharmacy). Pentamidine can cause a healthy person to cough violently - we do not want to breathe that so we use the Respiguard. The Respiguard has one way valves in the wye that allows the patient to get the drug but inhibits it from coming out so we don't breathe it. Also has a pell filter to keep the drug in the system. |
|
|
Insensible Water Loss |
The amount of water we lose everyday from our body through our lungs and skin but we are not aware of it. |
|
|
Daily Intake |
The majority of our daily intake of fluid is oral; 2/3 of our intake comes from liquids; 1/3 comes from food; Body synthesizes 150-200ml of water from H2 oxidation; Normal daily intake is 2400ml/day (1L = 0.26 gallons; 2.4L = 0.62 gallons); Hospital: we measure the I's and O's (intake/output ratio) - what goes in must be peed out otherwise the fluid will end up in edema. |
|
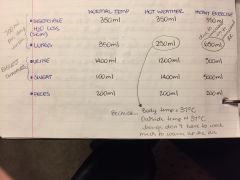
|
Normal insensible water loss is ~ 700ml/day (350ml+350ml). Changes from the normal occur in hot weather when the atmosphere has already done some of the respiratory system's work by pre-warming and humidifying the inhaled gases. In exercise, due to an increase in Vt, more insensible water is lost from the lungs. Urine output is dramatically affected by the body's need to conserve fluid to maintain blood pressure. The output of sweat increases with hot weather and exercise. We know that the skin protects us from major water losses and invading infections. In burn victims (especially 3rd degree), the epidermis and dermis have been burned. The epidermis contains cholesterol that prevents evaporation of massive amounts of water from our skin. We say the skin is CORNIFIED (contains cholesterol - prevents water loss). Burn victims can lose 4-5L of fluid a day in insensible loss due to their lack of skin. |
|
|
Explain the concepts of Solvent and Solute |
Solvent is the liquid we dissolve a drug, which is the solute. |
|
|
State the 3 types of solutions that can be used for sputum induction and give an example of each: |
Hypertonic Solution: ocean water; concentration of salt in solution is higher than the concentration of salt in the body; Hypotonic Solution: distilled water; concentration of salt in solution is lower than the concentration of salt in the body Isotonic Solution: normal saline; same osmolarity as the body |
|
|
Explain why hypertonic and hypotonic solutions can cause airway obstruction: |
Hypertonic solutions, when introduced to the respiratory tract, will cause crenation of the mucosal cells because the concentration of salt in the solution is higher than the concentration of salt in the body fluid (so water tends to move from a higher concentration to a lower concentration). This release of fluid from the mucosal cells, or bronchorrhea, is a potential airways obstruction. Hypotonic solutions, when introduced to the respiratory tract, will cause the water from the solution to be absorbed into the mucosal cells (mucosal swelling) because the concentration of salt in the solution is lower than the concentration of salt in the body (water moves from higher concentration to lower concentration). The swelling of the mucosal cells is also a potential airway obstruction. If a patient's airway is obstructed, the patient will be coughing and gasping for breath; sounds like wheezing, gurgling. Also, we can hear stridor (whistling sound) on inspiration due to narrowed airway. |
|
|
Name two types of nebulizers that could be used for sputum induction |
Ultrasonic nebulizer and mini neb (small volume neb) |
|
|
Define 2 types of exams that can be done in induced sputum: |
Bacteriological exam (gram stain and C&S): thick cell walls will absorb violet dye (gram +); thin cell walls will be washed away in alcohol and will absorb safranin red dye (gram -); tuberculosis has its own stain (carbol-fuchsin) known as the Acid Fast Bacillus (AFB). Exfoliative cytology: we can search for abnormal cells (cancer cells tend to shed easily); same principle of the pap smear. |
|
|
3 clinical uses of aerosol and 3 hazards |
Uses: 1. post srugery to wet down the airways that were exposed to dry gas (anesthetics) 2. to deliver medication 3. to decrease mucosal edema, thin out mucus Hazards: 1. bronchospasm due to cold aerosol 2. side effects of drugs: muscle tremors, tachycardia, nausea and vomiting, nervousness and anxiety,... 3. nosocomial infections cause by bacterial contamination in equipment |
|
|
SPECIAL NEB DNAase (Pulmozyme) administration |
We used to use different kinds of nebulizers for different drugs, but nowadays these drugs have become so common that we just use a small volume neb. DNAase (pulmozyme) is a drug used for cystic fibrosis patients (CF) who have very thick and viscous secretions; it is a mucolytic drug (thins out mucus, which is 95% water and 5% other substances... In this case we are trying to thin out these 5%); it breaks down DNA bonds in mucus so the patient can cough it up. Nowadays we just use a small volume neb to administer the drug. |
|
|
Classification of Oxygen Devices |
1. LOW FLOW DEVICES (VARIABLE PERFORMANCE): units that DO NOT supply all the inspired gas needed to meet the patient's minute ventilation. Room air is mixed with the oxygen, therefore, depending on the patient's minute ventilation pattern, the FiO2 is variable. Just adds a little bit of oxygen to the patient's minute ventilation. 2. HIGH FLOW DEVICES (FIXED PERFORMANCE): oxygen units that supply all the inspired gas needed to meet the patient's minute ventilation. The FiO2 delivered is not affected by the patient's ventilatory pattern; designed to meet the patient's minute ventilation. |
|
|
RESPIRATORY RATE NORMALS |
Number of breaths per minute; Normal adult: 12-20 Normal pediatric: 20-40 Normal neonate: 40-60 |
|
|
TIDAL VOLUME NORMALS |
The normal amount of air breathed in or out when a person is resting comfortably; Normal adult: 400-600ml Normal pediatric: 50-400ml Normal neonate: 25-50ml |
|
|
MINUTE VENTILATION NORMALS |
the amount of air breathed in or out in one minute; Normal adult: less than 10L/m No real normals for neonates and peds, we learn how to assess work of breathing (WOB). |
|
|
RESPIRATION |
Internal: exchange of CO2 and O2 at the cellular/tissue level External: exchange of O2 and CO2 at the alveoli level (AC membrane) |
|
|
Ventilatory Pattern |

Rate, depth, and amount of work a patient is putting into breathing. Ex.: Cheynes-Stokes, Biots, Kussmauls. 1. Neurological Injury: injury to the brain/brain stem that affects the respiratory/breathing centers in the pons and medulla oblongata. - Cheynes-Stokes: typically injury to pons; increasing and decreasing tidal volumes with periods of apnea - Biots: typically injury to the medulla; very disorganized tidal volumes with periods of apnea; life threatening. 2. Kussmaul's: associated with diabetic ketoacidosis; deep and fast breathing; as RTs we need to intubate these patients and support their respiration while the insuline-glucose issue is resolved. |
|
|
Apnea |
no breathing; Central: problem in the respiratory centers of the brain/brain stem; could be genetic, need a ventilator; Obstructive: tongue, tonsils, obesity; OSA (Obstructive Sleep Apnea) can use BiPAP (pressure on inspiration and expiration) or CPAP (not as serious, pressure on expiration to force the airway to stay open). |
|
|
Deadspace |
an area of the lung has ventilation but no perfusion (V/Q mismatch = large number/0); caused by a thrombus or embolus (think of the conducting airways - anatomical deadspace, only air no exchange) |
|
|
Shunt |
an area of the lung as perfusion but no ventilation; (V/Q mismatch = 0/large number) caused by atelectasis (loss of volume in the lung), consolidation (fluid in the alveoli - hard for gas exchange to happen because it increases the thickness of the AC membrane), pneumothorax (collapsed lung). |
|
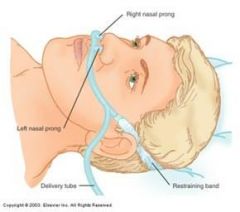
LOW FLOW DEVICES Nasal Cannula |
The advantages of this device are ease of application, light weight, economy and disposability. The disadvantages are instability (easily dislodged from a restless patient); Low flow rates MUST BE MAINTAINED (less or equal to 8L/m) to prevent sinus headaches; Nasal pathologies (deviated septum, mucosal edema, polyps) will decrease oxygen uptake. FiO2 range: 22-50% Flow range: 1/8 - 8L/m Regular NC: Adults: 1 - 4L/m (no need for humidification below 4L/m; higher than 4L/m use a bubbler) Pediatrics: 1/2 - 4L/m (always use a bubbler) Infants: 1/64 - 1.5L/m (always use a bubbler) |
|
|
LOW FLOW DEVICES Nasal Catheter |
This device is passed through one nasal passage with its tip in the oropharynx. There are 2 placement methods: 1. The distal 1/3 is lubricated with a water soluble gel (like isotonic saline, it will not irritate the mucosa, dissolves in the body easily), then the catheter is slid along the nasal passages until the catheter tip is just passed the uvula. We use a tongue depressor to visualize the uvula. Then we pull back the catheter until it has disappeared (to prevent aspiration pneumonia), and tape the catheter to the nose. 2. BLIND METHOD: measure from the tip of the nose to the tip of the ear lobe and place as before; not safe. Force should not be used to advance the catheter down either nare, as mucosal edema will result. Catheters should be changed every 8 hours as the body interprets them as foreign bodies and quickly adheres to them. FiO2 range: 22 - 50% Flow range: 1/8 - 8L/m |
|
|
ASPIRATION PNEUMONIA |
When air enters the patient's stomach in large quantities, it becomes distended and the patient vomits. The pH of vomit is less than 2, very acidic, so this acidic ion is aspirated into the trachea which is directly in front of the esophagus. This acid eats away the lung parenchyma causing further respiratory complications. For this reason, we always try to place nasal catheters using the first method described (visualizing the uvula), and not the blind method. In order to prevent aspiration pneumonia, deeply comatose patients or an elderly patient with obtunded (confused) reflexes such as post stroke (CVA - cerebrovascular accident) patient should NOT use a catheter. Today we use them rarely, but all the problems they cause are still with us (nasopharyngeal suctioning, nasogastric tube placement). Obtunded patients: their gag reflexes are not as good as a young healthy person. Gag reflexes protect our airways. |
|
|
General Characteristics of Oxygen Masks |
Masks are used when we need oxygen quickly and for a short period of time. They are uncomfortable and can cause pressure necrosis of the skin. They are also hot, as they trap the radiating heat from the nose and mouth. The humidity that is trapped from exhaled gas can break down the skin (pressure necrosis). The mask can become a vomit trap. If you have an unconscious patient and he vomits, due to a decrease in gag reflex, vomit can get trapped inside the mask and the patient could possibly aspirate it into his lungs causing further respiratory problems (risk of aspiration pneumonia). If you must use a mask with this type of patient (obtunded), an oral airway must be inserted to prevent the flaccid tongue from obstructing his airway. Evaluate patient for gag reflexes Oral airway = goes over the tongue like a hook |
|
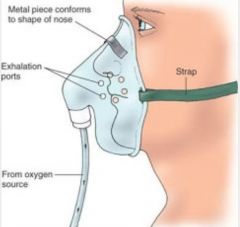
LOW FLOW DEVICES Simple Mask (3-in-1 mask, medium concentration elongated mask) |
Loose fitting disposable unit used very often on ambulances, not so much in the hospital. Room air can be drawn in around the edges of the mask (loose fitting) and through the exhalation ports. A low flow of oxygen is necessary to flush the deadspace for carbon dioxide removal. The FiO2 delivered to the patient depend upon his ventilatory pattern and the amount of room air being drawn in. Normal FiO2 rates: 35 - 55% Normal flow rates: 6 - 10L/m |
|
|
Clinical question 1: Would a simple mask be a good device to use in a patient taking slow, shallow breaths? |
Yes, it is giving enough flow to meet the patient's minute ventilation. But we have to monitor the patient so he doesn't stop breathing. |
|
|
Clinical question 2: Would a simple mask deliver a high or a low FiO2 in a situation where the patient is taking slow, shallow breaths? |
If patient's minute ventilation = 6L/m, 4L/m are provided by the mask and 2L/m are being drawn in through side ports on the mask and the edges of the mask. Patient is taking slow and shallow breaths, so not that much room air is being entrained, therefore it is a high Fio2 in this case. |
|
|
Clinical question 3: What would the FiO2 on a simple mask be if the patient is tachypnic or in acute respiratory failure? |
FiO2 would be very low, because patient will be drawing in a lot of room air. It is not a good equipment in this case, we will need more flow than what the mask can provide. |
|
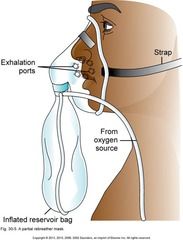
LOW FLOW / HIGH FLOW DEVICE Partial Rebreather Mask |
This can be either a low flow or a high flow device depending on the patient's ventilatory pattern. The purpose of this mask is to conserve oxygen by rebreathing some gas from the conducting airways. The conducting airways are all the generations of bronchi and bronchioles that DO NOT participate in gas exchange, therefore remain relatively high in FiO2. The reservoir bag holds 100% oxygen on inspiration; the patient draws oxygen from the bag into the mask and gets a high FiO2. During exhalation, the first 1/3 of the gas comes from the conducting airways (ANATOMICAL DEADSPACE) and goes back into the bag. The second 2/3 of expired gas, which has participated in gas exchange, goes out the mask ports (the pressure in the reservoir bag prevents the last 2/3 of the exhaled gas from coming in). The oxygen flow into the bag should be high enough to prevent it from collapsing and to wash out carbon dioxide. The exhalation ports serve as emergency inlets for room air in case the Oxygen source gets disconnected. Normal FiO2: up to 60% (depends on how the patient is breathing Normal flow rates: 6 - 10L/m or what keep the reservoir bag inflated on inspiration. |
|
|
High Flow Devices General Characteristics |
Historically, the first high flow device was a rebreather mask used in anesthesia. The mask tightly covered the nose and mouth. It had an attached reservoir bag from which the patient inhales. As this is a closed circuit, exhaled carbon dioxide is adsorbed through a filter while fresh oxygen is added to replace the gas metabolized by the patient. Provides the entire patient's minute ventilation |
|

HIGH FLOW DEVICES |
Mask with valves and reservoir bag On inspiration, the valve between the mask and the bag opens. 100% source of oxygen flows to the patient; the mask valves (on the side ports of the mask) close due to a sucking action of the patient. On exhalation, the mask/bag valve closes so the fresh 100% oxygen source gas is not contaminated with exhaled gas. Meanwhile the side port valves open, allowing the patient to exhale carbon dioxide. we take one side port valve off so in case the oxygen source is disconnected, the patient can draw in room air and not suffocate. The disposable hospital model with one side port valve off really delivers ~ 70% oxygen due to the leaks around the face and the missing valve. Normal flows to start an adult are 6 to 10 L/m. If a specialty gas must be given (Helox, Carbogen) we try to make a very snug fit and replace the valve, then closer to 100% can be achieved. This type of patient must be monitored constantly by health care practitioners. Humidification systems CANNOT ADD EFFECTIVE HUMIDITY due to the high patient flows, and also they can be a DANGER AS HUMIDITY MAY MAKE OF ONE THE ONE WAY VALVES STICK. |
|
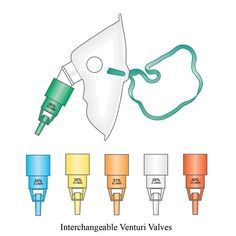
HIGH FLOW DEVICES Venturi Mask (Air Entrainment Mask) |
HAFOE (High Air Flow, Oxygen Enriched); Uses Berunoulli's principle, a jet entrains air just distal to the restriction. The smaller the jet (restriction), increased forward velocity, decreased lateral pressure, more air entrained, decreased FiO2. All Venturi Masks have as their goal to give an exact FiO2 while providing total flow higher or equal to the patient's peak inspiratory flow. In addition to the size of the jet (restriction), the FiO2 is determined by the size of the entrainment port, L/m to the jet (remember to follow the manufacturer's specifications) and the amount of resistance encountered in the system. The back pressure caused by hooking up several devices together will cause decreased air entrainment, therefore an increased FiO2 to the patient. At FiO2 lower or equal to 40%, no humidity will need to be added to the mask, but at higher FiO2 humidity may be needed due to increased flow. For that we use the HUMIDITY COLLAR. Venturi Masks only go up to 50% FiO2 (same principle of FiO2's higher than 50% on a nebulizer, we need to add another neb to provide enough flow... In this case we need to switch to a more complex equipment). FiO2 range: 24 - 50% Flow: whatever is specified by manufacturer on the selected FiO2 The humidity collar is attached to the mask so that the entrance for the aerosol is leveled with the air entrainment port of the Venturi Mask. For this reason, and also not to disturb the FiO2, we attach the neb to an AIR FLOWMETER. These masks are uncomfortable and must be removed for eating and drinking. Once an ABG is obtained, we try to switch the patient over to a comparable setting on a NASAL CANNULA. |
|
|
NASAL CANNULA TO VENTURI MASK (and vice-versa) |
% on Venturi Mask = % of oxygen in room air + 4(x); where x is the flow on the nasal cannula. %VM = %RM + 4(x) 30% = 21% + 4x 30 - 21 = 4x x= 9/4 x=2.25 = 2L/m on NC |
|
|
Pneumatic Large Volume Nebs: High flow or low flow devices? |
All pneumatic large volume nebulizers can be considered high flow devices. Remember when in the high FiO2's (higher than 50%), set up two nebs to provide the patient with adequate flow. |
|
|
MISCELANEOUS DEVICES |
These devices are normally used with high flow setups, but don't neatly fall into the category. |
|

MISCELANEOUS DEVICES Oxygen Blenders |
Mosby, page 102 This piece of equipment incorporates a proportioning valve, to adjust the FiO2, and reducing valves, to decrease the 50 psig down to a comfortable level for the patient. The Bird, Bennet, and Ohio models can give the patient between 90-120 L/m if necessary. These blenders are used with free standing high flow set-ups or on ventilators. Proportioning valve inside the blender moves to provide the selected FiO2. |
|
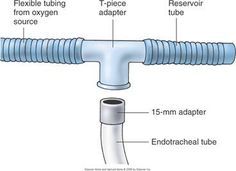
MISCELANEOUS DEVICES Tee Piece (t-piece) |
Used with an endotracheal tube (ETT) especially during weaning. Nor recommended for trach patients. If a patient is intubated and we are trying to wean him: we add a t-piece to the ETT, attach a large volume nebulizer to the T with large bore tubing and see how the patient does. If he gets too tired, go back to the ventilator. Next day, try again. Eventually he will be able to breathe on his own a little longer at every try, until we are safe to remove the ETT. |
|

MISCELANEOUS DEVICES |
This device uses large bore tubing and fits snuggly on the chin. Good to use with patients that suffered nasal or facial trauma. Hooked to a neb for heat and humidity. |
|

MISCELANEOUS DEVICES Aerosol Mask |
Used with large bore tubing and nebs, ultrasonics, or any setup that gives particulate water (aerosol); Large holes that allow aerosol to move freely in and out of the mask. |
|

MISCELANEOUS DEVICES Tracheostomy Collar |
Used in trach patients with large bore tubing and a neb. Provides heat, humidity and oxygen to the patient. Around the 2nd and 3rd tracheal rings is where the trach tube is inserted; the trach collar goes around the neck. VAP (Ventilator Associated Pneumonia): is a type of lung infection that occurs in people who are on breathing machines in hospitals. As such, VAP typically affects critically ill persons that are in an intensive care unit (ICU). |
|
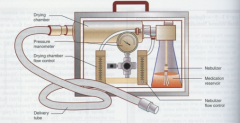
SPECIALIZED NEB SPAG (Small Particle Aerosol Generator) |
RSV (Respiratory Syncytial Virus) is an RNA virus; in healthy individuals it can present with a bad cold (adults, healthy children and elderly as well); easily contracted. When taking care of patients that contracted RSV we need to put them in isolation (wear gloves, gown, mask, be well protected). In patients with chronic illnesses (asthma, CHF) it can be life threatening. Chronically ill children (and adults) develop BRONCHIOLITIS (inflammation of the bronchioles). Best way to treat is IV fluids and major suctioning. Historically (80's and 90's), we gave Ribavarin (Virazole), a solution made by the pharmacy (6g of drug dissolved in 300ml of water), to a child for 12 hours a day for 5 days in a row. Contains a black tube that connects to the drying chamber (a special chamber that removes water from the particles created in order to reduce the size of the particles to 2-3um) and a blue tube that connects to the nebulizer (which has two capillary tubes). The outlet, a large bore tubing connection, could be connected to a peacehood, croup tent, aerosol mask, or a ventilator. When the drug was nebulized it became very sticky, like powdered sugar; so for a ventilator it is necessary to add filters in line so as to not damage the equipment. |
|

INFANT AND PEDIATRIC DEVICES Nasal Cannulas |
We use a sticky play dough type substance that we mold to the child's cheeks (dermaplast, tegederm, duoderm, dots) that secures the cannula and makes it much more difficult for the kids to remove them. We see simple masks, aerosol masks and Venturi masks used on a limited basis in pediatrics. T-pieces and trach collar are used much more frequently. Nasal prongs are very small; Always used with simple bubble humidifier; No-No's: velcro wrapped restraints, soft, for preventing children from taking off equipment. Infants can use from 0.5 - 1/5 L/m |
|

INFANT AND PEDIATRIC DEVICES Pediatric Hoods (peace hoods) |
Used with both humidifiers and nebulizers, can provide heat, humidity and oxygen. Hoods cover only the child's head, leaving the rest of the body available for nursing care. Blenders can be used to give precise FiO2 (for example in children with BPD). The gas must be warmed s the infant's temperature sensors are on the face: decreased temperature, increased oxygen consumption. The goal is to maintain a Neutral Thermal Environment (NTE) - Maintain body temperature. Use a T-piece inside, connect a large bore tubbing to the end of the T and connect to a nebulizer. Harder ones were used back in the day. Research showed that babies that were in this type of hood eventually ended up with hearing loss due to nebulizer noise being echoed inside the hood. Now we only use heated humidifiers instead of nebs. Babies minimum flow is 5L/m, but in the clinical setting we use 15-20L/m to make sure it all is being washed out and baby is getting enough flow. |
|
|
INFANT AND PEDIATRIC DEVICES Incubators |
Used to produce a NTE for premature infants; Oxygen added via heated neb or humidifier; The newer incubators have double walls to maintain NTE and prevent apnea and bradycardia. The incubator has a temperature knob to adjust temp according to infant's weight and age. Passover humidifier inside the incubator - humidity reservoir/heater was located right below the child's mattress, providing a dark and humid place for bacterial proliferation. So no we do not use those anymore, instead we provide heat, humidity and oxygen by using a complex humidifier that stays outside the incubator (being mindful of the distal probe of the servo-control system: if it stays inside the incubator it could disturb the temperature in the humidifier due to the NTE inside the incubator. To keep the servo control distal probe out of the incubator, attach an extension to the nasal cannula). RED FLAG: With the air entrainments open, the incubator can provide an FiO2 of 40%. In order to provide an FiO2 higher than 40%, we turn the red flag button that closes the entrainment ports on the incubator and also lets everyone know the infant is receiving a high FiO2. |
|
|
INFANT AND PEDIATRIC DEVICES Croup Tent |
These are used in pediatrics to provide a cool temperature within a plastic enclosure. The cool aerosol helps decrease airway edema during croup. Flows of 12 - 15L/m must be used to wash out carbon dioxide. FiO2 is impossible to control (either room air or oxygen). All electrical appliances (nurses call button, electric toys, etc.) should be kept out of croup tents due to possible sparks. Has a small air refrigerator on the back (has coils that cool the air); Large volume nebulizer with horns: one produces the aerosol and blows it to the croup tent, the other brings the cool aerosol/air back into the neb to maintain the cold aerosol circulating. You can try tucking in the plastic curtain under the child's mattress, to provide a higher FiO2 but it is very difficult to control the children not to kick the curtain and remove it. metal hook = grounding 12L/m is a minimum flow on the croup tent; we now run it out of high pressure hoses at 50 psig. |
|
|
Nasal Cannula |
FiO2: 22 - 50% Flow Rate: 1/8 - 8L/m Type of Tubing: Small bore tubing Humidification devices: simple bubbler (always for infants and pediatrics; adults only above 4L/m) High flow or Low flow: Low Flow |
|
|
Nasal Catheter |
FiO2: 22 - 50% Flow Rate: 1/8 - 8L/m Type of Tubing: Small bore tubing Humidification devices: Simple bubbler (always for pediatrics and infants; adults only above 4L/m) High flow or Low flow: Low flow |
|
|
Partial Rebreather Mask |
FiO2: up to 60% Flow Rate: 6 - 10L/m or what keeps the reservoir bag inflated on inspiration Type of Tubing: Small Bore Tubing Humidification devices: NONE High flow or Low flow: Low - High Flow, depending on how the patient is breathing |
|
|
Non-rebreather Mask |
FiO2: up to 70 - 90% Flow Rate: 6 - 10L/m Type of Tubing: Small Bore tubing Humidification devices: NONE High flow or Low flow: High Flow |
|
|
Simple Mask |
FiO2: 35 - 55% Flow Rate: 6 - 10L/m Type of Tubing: Small bore tubing Humidification devices: NONE High flow or Low flow: Low Flow |
|
|
Venturi Mask |
FiO2: 24 - 50% Flow Rate: 3 - 15L/m, according to manufacturer specification on selected FiO2 % Type of Tubing: Small bore tubing; large bore tubing for humidity collar Humidification devices: Nebulizer connected to air flowmeter and to humidification collar on mask (large bore tubing) High flow or Low flow: High Flow |
|
|
Curiosity: adult care, wounds that aren't healing... |
Nurses might put a simple mask close to a wound to give enough oxygen to the tissue and increase the healing process. |
|
|
Non rebreather mask is used... |
1. prior to intubation; 2. for comfort care; 3. fire victim (because of carbon monoxide poisoning). |
|
|
State 3 clinical situations in which a patient could not comfortably wear a nasal catheter: |
1. deviated septum 2. polyps 3. mucosal edema |
|
|
State the proper technique to insert a nasal catheter: |
The device is passed through one nasal passage with its tip in the oropharynx. The distal 1/3 is lubricated with a water soluble gel, then the catheter is slid along the nasal passage until the catheter tip is just passed the uvula. we then pull back the catheter until it has disappeared and tape it to the patient's nose. |
|
|
How can aspiration pneumonia occur in a comatose patient? |
Comatose patients have a depressed gag reflex; if excess air goes into their stomachs (from a nasal catheter, for example), the over distention can cause them to vomit. Vomit has a pH of less than 2, and because gag reflexes are depressed, when it comes up through the esophagus it can easily have access to the larynx and enter the trachea. A low pH can destroy the lung tissue. To prevent this, we should keep these patients on a sitting position. |
|
|
How can an oxygen mask cause necrosis or become a vomit trap? |
Pressure necrosis could happen due to the humidity build up from the exhaled gas into the mask, and the fact that the mask could be too tightly fit on the patient. It can become a vomit trap in case the patient vomits: vomit gets trapped inside the mask and the patient could potentially aspirate it (which is a high risk for aspiration pneumonia). |
|
|
Why should a simple mask not be used for a patient in acute respiratory failure? |
It does not provide enough flow or high FiO2 and will not meet the patient's ventilatory demands. |
|
|
Explain in detail how both partial and non-rebreather masks work: |
Partial Rebreather does not contain valves. 100% oxygen comes into the reservoir bag through small bore tubing and inflates the bag. The patient inhales the 100% oxygen from the reservoir bag and a small amount of room air is entrained through the side ports on the mask. As the patient exhales, the first 1/3 of exhaled gas comes from the conducting airways (which only store oxygen, do not participate in gas exchange) and goes back into the bag. The last 2/3 of exhaled gas come from respiratory airways, in which gas exchange has occurred, therefore the CO2 present is exhaled through the side ports (it does not go back into the reservoir bag because the pressure of 100% oxygen inside the bag + the flow going to the patient flush the CO2 out). The exhalation ports also serve as an emergency in case gas source is disconnected (the patient can draw in room air). The Non-rebreather mask contains 3 one way valves: one on the outlet between the reservoir bag and the mask, and one of each side port on the mask. Gas comes in through small bore tubing connected to the reservoir bag, inflating the bag. On inspiration, as the patient draws air in the valve between the reservoir bag and the mask opens and the valves on the side ports are sucked in closed. On exhalation, the side ports are pushed open to allow for exhaled gas to exit the mask, and the valve between the reservoir bag and the mask is pushed closed by the exhalation pressure. We take off one of the valves on the exhalation ports for safety in case of gas source disconnection, therefore the mask provides ~ 70 - 90% FiO2 due to a small room air entrainment from that "non-valved" side port. |
|
|
Explain the two method that are used to alter the FiO2 in a Venturi Mask: |
By changing the jet size or changing the size of the entrainment port, we can alter the FiO2 on the Venturi mask. Small jet size will cause a higher increase in forward velocity, larger drop in lateral pressure, higher sucking action drawing room air and a lower FiO2. The larger the entrainment port, the lower the FiO2 (more room air is entrained). |
|
|
Why is the humidity collar, that is added to a Venturi mask, run off room air? |
Because the Venturi mask delivers a very specific FiO2, by adding a source of humidification we do not want to interfere with the selected FiO2. Therefore, we connect the humidity collar to a neb that is attached to an Air Flowmeter. |
|
|
Why is the dermaplast or duoderm used in pediatric/infant nasal cannulas? |
To secure the nasal cannula to the child's face so they cannot remove it. Also DOTS (tender grips, like a modified bandaid). |
|
|
Explain how the servo control on the incubator works. |
We nee to maintain a neutral thermal environment (NTE) for the infant. On the dial on the incubator we can select a temperature according to the infant's weight and age and the incubator will heat up or cool down in order to maintain that temperature and a NTE. |
|
|
What does the red flag on the incubator signify? |
The red flag means the entrainment ports are closed and the infant is being delivered oxygen that is higher than 40%. |
|
|
How do we normally deliver heat, humidity and oxygen today? |
In order to deliver heat, humidity and oxygen in an incubator, we need to use an external complex humidifier, making sure there is an extension between the nasal cannula and the distal probe of the servo control so the probe can stay outside the incubator (otherwise it will disturb the temperature set in the humidifier because of the NTE inside the incubator). |
|
|
Why do we normally NOT use the passover humidifier built into the incubator? |
We don't use the passover humidifier built into the incubator because it is a great source of bacterial proliferation, therefore a source of infection. |
|
|
Explain the path of cool air circulation throughout the croup tent. How much flow should be set in order to wash out carbon dioxide? Why is it so difficult to maintain a stable FiO2 in a croup tent? |
Air is cooled using the refrigerator coils and blown into the croup tent by the fan. Aerosol is produced in the large volume jet nebulizer that contains two large horns: one horn delivers the aerosol into the croup tent, the other horn brings cool air and formed aerosol back into the nebulizer. This way, cool aerosol keeps on circulating throughout the tent. Minimum flow is 12 L/m, but we now use high pressure hoses at 50 psig, therefore the flow is a lot higher. Because it isn't a tightly enclosed space, we cannot maintain a stable FiO2 (there are leaks in the plastic curtain, the child could kick it if you try tucking the ends under the mattress, we might have to open the sides of the plastic curtain to deliver medication, etc.) |
|
|
Why do we maintain infants in a neutral thermal environment? |
Because if it is too cold or too hot, the infant increases his/her work of breathing and oxygen consumption. Our goal is to make it as comfortable as possible for the child to maintain a minimum WOB; babies can cold if they are too hot or too cold. |
|
|
How do we deliver heat, humidity and oxygen to the oxyhood? What is the minimum flow to washout carbon dioxide? |
We use a t-piece connected to large bore tubing and a heated (complex) humidifier. We can also use a nebulizer, however, it is not indicated due to risk of hearing loss. Minimum flow is 5 L/m (6 - 10L/m), clinically we use higher flows (~ 15 L/m) to start. |
|
|
Goals of oxygen therapy |
1. To treat hypoxia and hypoxemia 2. to decrease work of breathing 3. To decrease myocardial work |
|
|
4 Types of Hypoxia |
1. Hypoxic Hypoxia 2. Circulatory Hypoxia 3. Histotoxic Hypoxia 4. Anemic Hypoxia |
|
|
HYPOXIC HYPOXIA |
A condition that results from reduced alveolar oxygen tension. Causes: low ambient oxygen tension or HYPOVENTILATION (less oxygen goes in, more carbon dioxide builds up). OXYGENATION: oxygen availability VENTILATION: carbon dioxide levels Low ambient oxygen tension comes from a low concentration of oxygen at 1ATM (for ex, high altitudes). Hypoventilation comes from not enough oxygen flowing into the alveoli (for ex., trauma to the respiratory centers, COPD) If pO2 is dropping, oxygen takes up less room in the lungs, so carbon dioxide can go up and occupy more room in the lungs. Damage to respiratory centers => brain forgets how to breathe => need a ventilator. |
|
|
CIRCULATORY HYPOXIA |
A condition that results from inadequate blood flow to the tissues or cells. Systemic conditions that can bring this on are SHOCK or CHF (congestive heart failure). Local conditions that can cause this are arterial/venous obstruction (pulmonary embolism). A circulation problem; Shock = tissues aren't getting perfused with blood; Shock is a medical emergency in which the organs and tissues of the body are not receiving blood. This deprives the organs and tissues of oxygen (carried in the blood) and allows the build up of waste products. Can result in serious damage or even death. CHF => ineffective contraction of the heart => blood can't get to tissues because it is too thick Pulmonary embolism => cuts blood flow |
|
|
HISTOTOXIC HYPOXIA |
Foreign substances in the blood prevent oxygen perfusion into the body's cells or cellular utilization of oxygen. An example would be cyanide poisoning that blocks mitochondrial receptor sites (cristae) for oxygen. Remember = toxic to cells |
|
|
ANEMIC HYPOXIA |
A condition of decreased oxygen content of the blood due to decreased hemoglobin levels or hemoglobin's inability to transport oxygen. Examples: anemia or carbon monoxide inhalation from fires or leaky mufflers. CO binds to the iron on the hemoglobin (which is also the site of binding for oxygen) 210 times faster than oxygen does. It takes the spot that oxygen uses for being carried throughout the body in the blood, and it is really tough to remove it. |
|
|
How effective is giving oxygen in HYPOXIC HYPOXIA? |
Responds best to oxygen as we immediately increase oxygen tension in the alveolus and blood (because the problem is only the low pO2). |
|
|
How effective is giving oxygen in CIRCULATORY HYPOXIA? |
Responds poorly to oxygen; No matter how much oxygen is in the blood, the blood is not getting to the tissues. CHF/Shock = we need to improve perfusion/circulation. We can give drugs to improve the contraction of the heart (POSITIVE IONOTROPES, such as Digitalis, Digoxin; also CHONDROTROPES, which increase the heart rate - sympathomimetic or parasympatholytic drugs such as epinephrine or norepinephrine). |
|
|
How effective is giving oxygen in HISTOTOXIC HYPOXIA? |
Will not respond at 1ATM of pressure, cells are unable to utilize the oxygen available. We need a hyperbaric chamber (hyper = higher than normal; baric = pressure). |
|
|
How effective is giving oxygen to ANEMIC HYPOXIA? |
You can saturate whatever hemoglobin is available, but still it may not be sufficient to meet the patient's needs. We need to increase the amount of hemoglobin (or RBCs), so we give either whole blood or packed RBCs. In case of CO poisoning: non-rebreather (70-90% oxygen) to force the CO out of the binding spot it is occupying in the hemoglobin so oxygen can have its spot back. |
|
|
Refractory Hypoxemia |
Even after giving high levels of oxygen there is no improvement in oxygenation. Refractory = difficult to deal with; It is an effect of ARDS (acute respiratory distress syndrome). Circulatory, histotoxic, and anemic hypoxia can all result in REFRACTORY HYPOXEMIA. |
|
|
4 Causes of HYPOXEMIA |
1. V/Q defect; 2. Hypoventilation; 3. Diffusion defects; 4. Shunt |
|
|
CAUSES OF HYPOXEMIA V/Q Defect |
Due to a mismatch between the two (ventilation/perfusion) caused by cardiopulmonary diseases. The result is that oxygen doesn't get into the capillaries or the tissues. Perfusion = blood flow to tissues 1:1 match is ideal; When you have zero/large number = means zero ventilation, but perfusion is happening = atelectasis, consolidation (fluid in alveoli, pulmonary edema), pneumothorax, pneumonia (PND). When you have large number/zero = means you have ventilation, but perfusion is not happening = usually caused by a thrombus or embolus. |
|
|
CAUSES OF HYPOXEMIA Hypoventilation |
Diminished ventilation to the alveolus due to pulmonary trauma or neuromuscular disease. PaCO2 is high, PaO2 is low = not moving much gas in and out Neuromuscular diseases: problems with the nerves or the neurotransmitters that go across synapses. Muscular dystrophy: sex link disease (passed from mother to son); Duchenne's muscular dystrophy. People with muscular dystrophy lose control of their voluntary muscles (or voluntary ability to move; respiratory function is affected as well - diaphragm) |
|
|
CAUSES OF HYPOXEMIA Diffusion Defect |
Pulmonary fibrosis (literally "scarring of the lungs" - is a respiratory disease in which scars are formed in the lung tissues, leading to serious breathing problems - associated with occupational diseases, such as the ones caused by asbestos), granulomas (caused by chronic irritation - such as smoking; type of tumor), interstitial or alveolar edema (fluid spills over the alveoli - we can give diuretics/Lasix). These prevent the normal transport of oxygen from alveoli to bloodstream or carbon dioxide from bloodstream to the alveoli for elimination (they increase the thickness of the AC membrane). |
|
|
CAUSES OF HYPOXEMIA Shunting |
Arterial/venous connection with no blood perfusing to the alveolus (blood does not get oxygenated). Congenital Heart Disease (CHD), such as atrial septum defect (ASD) or ventricular septum defect (VSD). ASD: could happen because the foramen ovale did not close properly, or in people with pulmonary hypertension (pressure inside the atria ends up getting too high and forces open the fossa ovalis - scar tissue left over when the foramen ovale closes). Blood ends up flowing from Left Atrium to Right Atrium (high pressure to low pressure); it puts a strain on the RA and will end up causing cor pulmonale (Right sided heart failure - RSHF). Patient will not be cyanotic because the blood has already been oxygenated. VSD: blood flows from Left Ventricle to Right Ventricle (high pressure to low pressure); will also cause cor pulmonale but faster, because of higher pressure in ventricles. |
|
|
Effects of Hypoxia |
1. Increased respiratory rate, increase tidal volume (VT), increased minute ventilation (Ve). 2. Increased tachycardia and cardiac output (amount of blood the heart puts out in a minute - CO = SV x HR - in adults 4 - 6 L/m), vasodilation of the blood vessels, vasoconstriction of pulmonary vessels |
|
|
SPECIALTY GASES Hyperbaric Oxygen Therapy |
There are two types: 1. A monoplace chamber, for one person; delivers 100% oxygen at up to 3ATMs of pressure; similar to a one man submarine. 2. An expensive multiplace room that holds many people and can dive too many ATMs. 100% O2 given at 1ATM = ABG shows PaO2 ~ 600 to 700 mmHg 100% O2 given in a hyperbaric chamber (3ATM) = ABG shows 1800 - 2100 mmHg |
|
|
SPECIALTY GASES Hyperbaric Oxygen Therapy Physiological Effects of High PaO2 |
1. New capillary bed formation (dramatically speeds up wound healing) 2. Arteriolar constriction 3. Alteration of growth of aerobic and anaerobic organisms (anaerobic infections - encourage patient to heal much faster) |
|
|
SPECIALTY GASES Hyperbaric Oxygen Therapy Physiological Effects of Increased Pressure |
Decrease in the size of the bubbles dissolved in the blood, therefore able to reverse the "bends" or Decompression Sickness. Example: When diving, every 33 feet someone dives represents 1ATM. The body is under a huge amount of pressure, so to back to surface divers need to go slowly, otherwise bubbles can form in the blood and become emboli (which can kill). It is not usually what we are treating, but just an example. |
|
|
SPECIALTY GASES Hyperbaric Oxygen Therapy Harmful Effects of Hyperbaric Oxygen |
1. CNS Toxicity: convulsions, sweating, pallor (an unhealthy pale appearance) and restlessness; 2. Pulmonary Toxicity: the breathing of 100% oxygen under increased atmospheres leads quickly to symptoms: cough, dyspnea, chest tightness. 50% oxygen for extended periods of time appears to be safe. |
|
|
SPECIALTY GASES Hyperbaric Oxygen Therapy Clinical Applications of Hyperbaric Oxygen |
1. Carbon monoxide or cyanide poisoning 2. Decompression sickness or gas embolism 3. Skin grafts, smoke inhalation, thermal burns 4. Acute peripheral arterial insufficiency and poor wound healing 5. Intestinal Obstruction 6. Refractory osteomyelitis (bone and bone marrow inflammation - oncology patients) and radionecrosis (oncology patients that went through radiation - kills the cancer but also damages healthy tissues) of bone and soft tissue. |
|
|
SHUNT |
Perfusion but no ventilation; Blood doesn't make it to the lungs. |
|
|
DEADSPACE |
Ventilation but no perfusion; Only condition that fits this description os THROMBUS/EMBOLUS |
|
|
PULSE OXYMETRY How is oxygen carried in the blood? |
1. dissolved = 0.001% 2. bound to Hb (hemoglobin) = 99.9% Pulse Ox only measures the dissolved fraction = DANGEROUS NUMBER |
|
|
PULSE OXYMETRY What if the pulse ox is a good number - do we need more information? |
If the pulse ox is a good number, it means the patient has good dissolved oxygen in the blood; we do not know how much hemoglobin the patient has and what his/her tissue oxygenation status is. |
|
|
PULSE OXYMETRY How the Pulse Ox works |
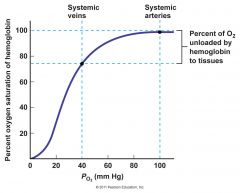
It contains two sources of light: red and infrared; Red we can see with our eyes, infrared we can't see (the wavelength is too long for our eyes). It takes the two types of light and shines through oxyhemoglobin (Hb+O2) and deoxyhemoglobin (Hb-O2). A software inside calculates the Hb dissociation curve (sigmoid curve). Descending portion of the curve = poor saturation Flat portion = good saturation = where we want to maintain most of our patients It shows the saturation of the Hb but DOES NOT SHOW HOW MUCH HEOGLOBIN THE PATIENT HAS. Note that: PaO2 at 96% saturation = 95mmHg (Room Air). If saturation decreases to 88% = PaO2 is 55 mmHg (huge difference). |
|
|
Non-Invasive Monitoring Pulse Oxymetry |
This is a non-invasive way to measure oxygen saturation (the patient doesn't have to be stuck for an ABG routinely). However, these machine must be used very cautiously, as they only tell you about the Hb present, not the actual amount of Hb that the patient has. In other words, the patient can have an excellent saturation and PaO2, but still be very anemic. The machine works the following way: both red and infrared light absorb HbO2 and deoxyHb with different intensities and different wavelengths. We take advantage of this fact by shinning these two types of light thorough a pulsating arteriolar bed. The different ratios of Hb/HbO2 for red and infrared light can be read out as a saturation. More info on Mosby pg 334 |
|
|
Non-Invasive Monitoring Pulse Oxymetry Two basic types of Pulse Ox |
1. Functional type: 99% of the pulse ox's we use are this type; uses the equation HbO2 / Total Hb, where Total Hb = Hb + HbO2 2. Fractional Type: uses the equation HbO2 / Total Hb + DysHb (dysfunctional Hb) |
|
|
Non-Invasive Monitoring Pulse Oxymetry Examples of DysHb (dysfunctional hemoglobin) |
1. CoHb (Carboxihemoglobin): where CO takes the O2 spot in the hemoglobin; CO bind to the Fe+2 on heme 210x faster than oxygen; fire and leaky muffler patients; we use a CO-oxymeter to measure CO dissolved in blood; use a non-rebreather to knock off CO from Hb; Rural Area, non-smoking person = 1 - 2% CO in blood Urban Area, non-smoker person = 5 - 6% CO in blood Urban Area, smoker person = 8 - 0% in blood 2. MethHb: happens when the iron portion of the Hb molecule changes from the ferrous form (Fe+2) to the ferric form (Fe+3); methHb is unable to transport any oxygen; Substances that can cause methHb: nitrates, nitrites, nitrous gases, nitroglycerin, sulfonamides. Sources of these substances are well water, show polish, welding materials, powdered milk, and red wax crayons as well as cured meats. Treatment: methylene blue, in severe cases (it converts ferric iron back to ferrous so Hb can function properly). Nitroglycerin (same as TNT) = massive vasodilator for patients with heart problems (severe coronary artery disease, if coronary arteries get clogged it causes terrible angina) - patient looks beet red, flushed; can be given in tablets, sublingual, paste (on skin).; only taken in an emergency. |
|
|
Non-Invasive Monitoring Pulse Oxymetry The Advantages of Pulse Ox |
- no heating or skin prep of the the site - no calibration - multiple monitoring sites are available |
|
|
Non-Invasive Monitoring Pulse Oxymetry The Disadvantages of Pulse Ox |
- motion artifacts are picked up in moving patients - it does require a pulsating arteriolar bed |
|
|
How would saturation change in the pulse ox if a person in exercising, is anemic, or was in a fire? |
Saturation measured on the pulse ox is the saturation of oxygen dissolved in the blood. It does not account for the amount of hemoglobin a person has. In general, if a person is exercising the saturation should not change. However, we have two different cases: if a healthy person is exercising, heart rate will increase and respiratory rate will increase to compensate for the oxygen being consumed by the muscle tissue, therefore, the saturation should not change. If we have a COPD patient put through a 6 minute walk, the saturation will decrease rapidly. This happens because, as part of the disease process, the patient is losing functional lung tissue everyday, therefore he cannot compensate for oxygen being used by the muscles even though the heart rate is also increasing. COPD patient's lungs cannot do the extra work to help replenish oxygen in the blood. As the pulse ox does not measure the amount of Hb, an anemic person would probably present no changes in the saturation as well. Which is dangerous and inaccurate, because the patient might present signs of fatigue and the pulse ox is showing 99% saturation. Patients that were in a fire is the same situation; since the pulse ox only accounts for dissolved oxygen in the blood, it does not account for how much Hb the patient has, in this case we will need a separate machine to measure carbon monoxide accurately. The pulse ox will be inaccurate. |
|
|
Explain the theory of how the pulse ox works: |
We have two sources of light (red and infrared) that measure oxyhemoglobin and deoxyhemoglobin. The pulse ox has an oxyhemoglobin curve generated by a software, which represents the % saturation of oxygen dissolved in the blood (it does not account for how much Hb the patient has). |
|
|
How can you asses the patient's oxygen saturation WITHOUT a pulse ox? |
Vitals ABGs Mentation Assesment |
|
|
In what types of patients would the pulse ox NOT be accurate (examples of clinical situations) |
- if a patient has just coded; - cardiopulmonary bypass (patient is cooled) - patients that are hypothermic (not enough blood flow to the skin) - drugs that cause vasoconstriction (for raising blood pressure) or vasodilation - anemic patients - fire patients |
|
|
SPECIALTY GASES Helium Therapy |
Helium comes from the deep mines in the southwest, therefore it is expensive and must be conserved; Physiologically, it neither participates nor interferes with any bodily processes, as it is inert. It is odorless, tasteless, non-combustible, nonexplosive, poorly soluble. Helium has an extremely low density, therefore it is very ineffective at transporting drugs and humidity (similar to anesthetic gases). However, due to its low density, it can easily negotiate airway obstructions (remember Graham's Law). The result is that when Helium is mixed with any other gas, the density of the mixture is low, so it can ventilate the lungs with minimal effort. The commercially available mixtures are: 80% He / 20% O2 70% He / 30% O2 |
|
|
SPECIALTY GASES Helium Therapy Clinical Uses |
Clinical uses of Helium therapy are in extremely severe bronchial asthma and severe COPD cases. When the patient is very hypoxic and has an increased WOB, Helox mixtures can get oxygen to the tissues. Helox is also commonly used in children with severe airway obstruction (can put them on Helox while waiting for them to go to the operation room or bronchoscopy to remove obstruction). When giving Helox, a tightly fitting non-rebreather mask or an artificial airway must be in place to prevent leaks. As Helium has a different density than O2, we must use a flowmeter correction factor if we have to use an oxygen flowmeter to administer Helox. 80/20 mix: 1.8 x reading on the O2 flowmeter 70/30 mix: 1.6 x reading on the O2 flowmeter Nowadays this si not an issue because he have the correct equipment. |
|
|
SPECIALTY GASES Helium Therapy Side Effects |
The only adverse side effect of Helox is a high pitched distortion of the human voice. This must be considered in the conscious non-intubated patient. |
|

SPECIALIZED NEBULIZER Breath Actuated Nebulizer |
Designed so the patient can breathe in the medication on inspiration and on expiration, the medication gets trapped inside the neb and it is not wasted. We can use it when we have a very expensive drug that we do not want to waste, and we want to make sure the patient inhales the entire dose. As the patient exhales, gas leaves through the outlets on the top of the neb, but medication stays in. More expensive. More on Mosby, pg 191 |
|
|
SPECIALTY GASES CO2 Therapy or CARBOGEN |
Carbon dioxide will not support combustion (inert) nor it will maintain life. It is 1.5 times as heavy as air, colorless, odorless. |
|
|
SPECIALTY GASES CO2 Therapy or CARBOGEN Physiological Responses |
1. Respiratory centers located in the medulla oblongata are stimulated with up to 10% CO2, but depressed by CO2 mixtures higher or equal to 10%. If CO2 is building up in the system, when stimulating the breathing centers in the brain they will cause tachypnea (breathing much faster) to try to get rid of CO2. Increased RR, increased Vt, increased Ve. 2. Circulation: direct stimulation of the cardiovascular centers in the brain causes an increase in BP by up to 40 mmHg (systolic), increase in HR by up to 20 beats/min, increase ionotropic effects (increase in the force of contraction of the heart muscle), constriction of the vascular beds supplied by the sympathetic nervous system (blood is divert from non-essential organs to essential organs such as brain, heart, kidneys). If CO2 is increased locally, vasodilation of the blood vessels take place as in exercising muscle or transcutaneous CO2 monitoring. 3. CNS Response: in low concentrations it causes mental depression; in high concentrations it causes convulsions and loss of consciousness. We can give carbogen only to patients with a responsive respiratory center, otherwise fatal HYPERCAPNIA will ensue. For example, we would not give this to a patient with COPD due to his respiratory centers decreased response (CO2 and also hyperventilation would cause increased WOB). |
|
|
SPECIALTY GASES CO2 Therapy or CARBOGEN How do we use it clinically? |
1. To improve cerebral blood flow in an elderly patient with a massive stroke (CVA) => the results are usually less than spectacular due to arteriosclerosis of the remaining blood vessels; High levels of CO2 in the brain causes vasodilation so we use i to open up the blood vessels that were constricted when the CVA happened. Nowadays we give tPA (tissue plasminogen activator), which allows for blood perfusion to the area. If done quickly within the first critical hours it can bring good results and prevent larger brain damage. 2. To overcome HYPOVENTILATION and prevent post operative atelectasis => CO2 stimulates HYPERVENTILATION, therefore better V/Q ratio; newer techniques are available that are much safer, such as Incentive Spirometry (IS). 3. Singulation (hiccups): This condition is caused by the spasmodic contraction of the diaphragm against a closed glottis due to an irritated phrenic nerve. In patients who are post-op or have debilitating diseases, gastric distention and metabolic toxins may cause unrelenting hiccups. Carbon dioxide appears to work by initiating rhythmic discharges to the diaphragm that are so strong they override the spasmodic contractions from the hiccups. This doesn't work very well... Remember: C3,C4,C5 KEEP THE DIAPHRAGM ALIVE (ORIGIN OF THE PHRENIC NERVE). 4. Uses in Philadelphia: Scheiss Eye Institute at Presby; given as a retinal vasodilator to improve eye sight post cataract surgery. Increases blood flow to the retina; Cataract: lens becomes cloudy due to scar tissue. |
|
|
SPECIALTY GASES CO2 Therapy or CARBOGEN Ways that Carbogen is administered: |
- 5% CO2 / 95% O2 for ~ 10 minutes; - Therapist must stay with the patient at all times (why? see "Physiological Responses"); - > 5% CO2: MD must be present at all times; - Administer with a well fitting NON REBREATHER MASK (we don't want CO2 escaping to the room). |
|
|
SPECIALTY GASES CO2 Therapy or CARBOGEN Potential Side Effects |
Headache (HA), dizziness due to a drop in diastolic BP, dyspnea, palpitations, dimming vision, muscle tremors, paresthesia (a sensation of pricking, tingling, or creeping on the skin having no objective cause and usually associated with injury or irritation of a sensory nerve or nerve root), coldness of the extremities, mental depression. If any of these appear, notify the MD. Toxic Symptoms = stop treatment immediately = dyspnea, nausea and vomiting, disorientation, increased systolic BP,... Carbogen = danger = use with extreme care. At CHOP given to Left Ventricle Hypoplastic Surgery candidates to decrease pulmonary blood flow and edema post-op. |
|
|
PaO2 in the brain (head) |
High levels = Vasoconstriction Low levels = Vasodilation |
|
|
PaO2 in the lungs |
High levels = Vasodilation Low levels = Vasoconstriction |
|
|
PaCO2 in the brain (head) |
High levels = Vasodilation Low levels = Vasoconstriction |
|
|
PaCO2 in the lungs |
High levels = Vasoconstriction Low levels = Vasodilation |
|
|
PaO2 and PaCO2 |
1. PaO2 <---> PaCO2 = inversely related! 2. Whatever happens in the head, the opposite happens in the lungs 3. Patients with neurological injuries = if PaCO2 in the head increases, it causes vasodilation of blood vessels in the brain = brain swells and gets bigger; risk of herniation of the brain tissue down the neck = DEATH. If PaCO2 goes down, it causes vasoconstriction = brain gets smaller. To get rid of CO2 we put the patient on a ventilator (increases RR and Vt) = HYPERVENTILATE the patient to keep CO2 lower than normal to prevent brain herniation. The only problem is: low CO2 = high pH = ALKALOSIS. Hyperventilation is only good for 24 hours, while the body tolerates it. |
|
|
SPECIALTY GASES CO2 Therapy or CARBOGEN Congenital Heart Disease |
HLHS (Hypoplastic Left Heart Syndrome) - smaller left side of the heart than normal - atrophy of the left ventricle = so small it cannot work properly (atretic LV) - full terms infants, cyanotic - undergo cardiac cath; turn the right ventricle into left ventricle to pump blood to the whole body through shunts; - we want to prevent problems in the lungs, such as pulmonary edema, so we give a low level of 100% CO2 to cause vasoconstriction (bleed in system). |
|
|
Pathophysiologic Effects of Oxygen Therapy |
The lung normally contains 80% Nitrogen and 20% Oxygen (what we breathe from room air). If the patient breathes in 100% Oxygen, the Nitrogen is washed out resulting in Nitrogen Washout Atelectasis and Surfactant Destruction. |
|
|
Oxygen Toxicity can come about from 2 general causes: |
1. METABOLIC - Free radicals are formed when oxygen is at high levels. Oxygen loses an electron and the free radical looks like "O-". This is unstable and goes around eating up healthy lung tissue (parenchyma). An enzyme in our body, SOD (super oxide dismutase), helps O- free radicals to recombine into O2. When the O2 levels are high, SOD is saturated (used up) and then O- free radicals continue to destroy lung tissue. Clinically it means that we cannot have patients on high levels of oxygen for a lengthy period of time, because it causes damage to the lungs. 2. When oxygen levels are high, the Type I pneumocytes (thin) start to die. They end up being replaced by Type II pneumocytes (which are thicker and produce surfactant, but can differentiate into Type I in case of damage). The loss of Type I cells means that much less oxygen can cross the alveolar capillary membrane (because it becomes thicker). |
|
|
Morphological Effects of Oxygen Therapy |
The mucociliary escalator slows down, then stops (nothing will work to bring mucus up and clear the lungs). This results in pulmonary infection. Also, surfactant, which keeps alveoli open, is destroyed = can cause atelectasis. |
|
|
Type of Diseases Associated With Oxygen Toxicity |
1. INFANT RESPIRATORY DISTRESS SYNDROME (IRDS): Premature babies have very little surfactant and alveoli. This results in massive atelectasis: they have to be placed on ventilators while they increase their alveoli numbers and surfactant. If they are still on oxygen when they are 1 month old, we officially diagnose them with BPD (bronchopulmonary dysplasia) or chronic pulmonary disease of the infant. 2. The high FiO2 required to support the premature infant's PaO2 can result in RETINOPATHY OF PREMATURITY (ROP) or RETROLENTAL FIBROPLASIA (RLF - fibrin in the eye behind the lens). This is when blindness results because fibroblasts and capillaries grow in the vitreous humor of the eye and block the retinal rods and cones. About 10% of premies develop this disease. 3. In adults, just about anything bad that can happen to you in life can cause ADULT RESPIRATORY DISTRESS SYNDROME (ARDS) = Pneumonia, head trauma, exposure to chemicals, motor vehicle accidents, ... Results in extreme lung consolidation, making it very difficult to ventilate the patient. Extreme pulmonary edema. |
|

Non-invasive Monitoring TRANSCUTANEOUS MONITORING |
Lab Book pg 32 HEAT INDUCED HYPEREMIA (more blood going to the skin due to heating) = by heating the skin above normal body temperature (37C), more blood diffuses to the capillaries and allow O2 and CO2 to be more readily available on the skin surface. Equipment used: CAPNOGRAPH with calibration gas (calibration for high and low O2 and CO2 levels) |
|

Non-invasive Monitoring TRANSCUTANEOUS MONITORING How to use it: |
- Instrument is turned on and sensor is allowed to warm up; once it reaches the desired temperature (42-44C), calibration is done. Sensor membrane is changed if necessary. Desired temperature, time in one spot, high and low alarms are set. - double sticky disk is applied with electrolyte solution to make better skin contact; - typical temperature range: 42C for infants/peds, 44C for adults - Typical time in one spot: 2 hours (premature baby - start by leaving from 30 min - 1 hr and checking the spot because they might burn easily; and peds) to 4 hours (adult) - The best place to put on a patient is a flat hairless area with a little bit of fat (intercostal spaces, abdomen, thigh). - The capnograph sensor is a dual electrode to measure PaO2 and PaCO2; it incorporates both Clarks electrode (PaO2) and Severinghaus' electrode (PaCO2). - PaO2 that appears in the monitor: calculated at 1ATM 760 mmHG - 47mmHg [water vapor pressure] = 713 713 x .21 = ~ 159mmHg (the partial pressure of oxygen in room air, shown in the monitor when calibrated). In the blood: 80 - 100 mmHG, lower because oxygen has to travel through many structures, so it ends up losing a little pressure). Make sure it correlates with ABG, otherwise we cannot use it. |
|
|
Non-invasive Monitoring TRANSCUTANEOUS MONITORING Limitations |
1. Shock (hypoperfused state) = no perfusion, no measurement 2. Vasoactive drugs (Vasoconstrictors = dopamine; Vasodilators = nitroglycerin): constrictors decrease the size of the blood vessels; will not give an accurate reading or will give a very low number because there isn't enough blood perfusing to the skin. Vasodilators might show a higher number or not work well. 3. Thickness of the patient's skin (less accurate in adults) |
|
|
What is the normal range of PaO2 or PaCO2 read when the TCPO2/TCPCO2 is on the patient's skin? |
PaO2: 80 - 100 mmHg (~95mmHg) PaCO2: 35 - 45 mmHg (~40mmHg) Same as a normal ABG |
|
|
Briefly explain how induced hyperemia allows O2 to diffuse to the skin: |
By heating the skin above normal body temperature (37C) we increase perfusion to the area and that allows for O2 and CO2 to be more readily available on the skin surface, so the sensor can read it. For infants/peds we increase the temperature up to 42C, for adults 44C. |
|
|
Baby Rendell is a full term infant suspected of PFC/PPHN, who has been given dopamine. How will this affect his TCPO2 and TCPCO2? |
Dopamine is a vasoconstrictor; it can cause the reading to be inaccurate (can show a lower reading or not measure at all). Vasoconstrictors reduce the size of the diameter of the blood vessels, so blood is not going to be as readily available as wanted. |
|
|
What is the most appropriate length of time to keep a TCPO2 electrode at one site on a premature infant? |
2 hours: we start by leaving for 30 min to an hour, always checking to see if there is any burns on the skin. |
|
|
You have just removed the TCPO2/TCPCO2 electrode from baby Street after 4 hours. A red wheal (bump, elevated red spot) with swelling appears on that area of his skin and it doesn't go away after a few minutes. What adjustments should you make to the monitor before you put it back on little Street? |
Change the spot, decrease the temperature, decrease time on spot. |
|

Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography |
Capnography: recording the changing levels of expired CO2; CO2 and water absorb infrared light, therefore we remove the water via filter (otherwise it will read a higher level of CO2). The higher the level of CO2, the more infrared light will be absorbed. |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Factors that affect the EtCO2 |
1. Cellular production of CO2 = varies with the patient's metabolism; ex.: hypothyroidism = slow thyroid = low level of CO2 2. Transport of CO2 from the cells to the lungs = varies with patent's circulation; Ex.: CHF = poor circulation 3. Elimination of CO2 from the lungs = central/peripheral chemoreceptors; Ex.: chronic lungers' chemoreceptors do not work efficiently anymore. |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Physiology |
1. Any disease/event that causes alveolar HYPOVENTILATION will increase the EtCO2 (neurological trauma, drugs, asthma, diffusion defect). 2. Decreased EtCO2 = Decreases pulmonary blood flow = suspect EMBOLI |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Instrumentation |
1. SIDESTREAM (aspiration devices): see book pg 264, fig 8-27A; Novametrix, older models; it is a connection to the mainstream of gas that aspirates small samples of exhaled gas and reads it on the side (sensor is placed on the side of the mainstream); 2. MAINSTREAM (non-aspirating devices): Hewlett Packard, Nellcor = all recent ones are this type; sensor is in the main flow of exhaled gas (see fig 8-27B pq 264 on Mosby) |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Inside the Capnograph |
See page 263, fig 8-26B Inside the capnograph there is: - a light source - chopper (looks like a helicopter) - reference cell: standard/calibration (has a known amount of CO2 and infrared light) - sample cell: from patient - CO2 detector (where CO2 flows into) - filter to remove water vapor Reference cell and sample cell are compared and a number is generated (% or mmHg). How to convert CO2% to torr (mmHg): Normal EtCO2 = 5.6% 0.056 x 713 = 40mmHg - remember to turn % into decimal - 713 comes from 760 - 47 equation. |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Normal Waveform |
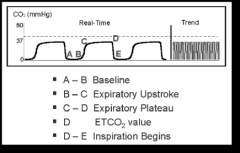
Cathy's normal given in class was slightly different, but just know: A: air from conducting airways, does not participate in gas exchange; DEADSPACE GAS; first gas to be exhaled; B: air from conducting airways + alveolar gas (contains a little gas exchange) C: alveolar gas D: EtCO2 reading (change from alveolar gas - from the bases to the apices of the lung) |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography ABG Correlation with EtCO2 |
Should be within 3-10 mmHg; if greater, do not use monitor = check the factors that affect EtCO2 |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Techniques |
You may ask an adult to take a deep breath and exhale, but a child will probably not cooperate as well... So for children we can try the chest squeeze technique; be gentle, watch out for recent feeding, surgical sites, chest tubes, CVP or atrial lines. Whether on or off ventilator = squeeze the chest at the end of inspiration. - How do you get a newborn's Vital Capacity: when an spontaneously breathing child cries. |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography A couple of extra notes... |
EtCO2 = noninvasive form of PaCO2 (that we would get from an ABG); Always make sure it correlates with ABG otherwise we cannot use it We use this in peds/infants so we don't have to stick them for a blood gas all the time, but also for neurological patients in the ICU |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Normal Capnogram |
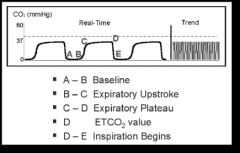
The normal capnogram is a waveform which represents the carying CO2 level throughout the breath cycle. D: the highest point; end tidal concentration |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Increasing EtCO2 level |
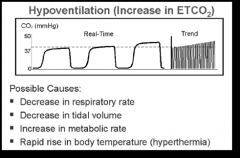
An increase in EtCO2 from previous levels; Possible Causes: - decrease in RR (hypoventilation) - decrease in Vt (hypoventilation - increase in metabolic rate (fever, exercise,...) - rapid rise in temperature (Malignant Hyperthermia) |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Malignant Hyperthermia |
Google: Malignant Hyperthermia (MH) or Malignant Hyperpyrexia is a rare life-threatening condition that is usually triggered by exposure to certain drugs used for general anesthesia - specifically the volatile anesthetic agents and SUCCINYLCHOLINE, a neuromuscular blocking agent. It is passed down through families; causes fast rise in temperature and severe muscle contractions when exposed to anesthetics. Cathy: Some patients might lack an enzyme that helps maintain body temperature; we (usually) don't know the person has this condition until the patient is under anesthesia: their temperature goes up (for example, 107F); high temperatures like that can result in seizures and death; if it happens we need to work in getting their bodies cooled (iced bath) to get back to normal body temperature. These types of patients cannot undergo surgery. |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Inadequate Seal Around the Endotracheal Tube |
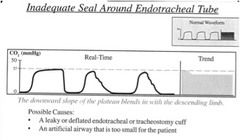
The downward slope of the plateau blends in the with the descending limb Possible causes: - a leaky or deflated endotracheal or tracheostomy cuff - An artificial airway that is too small for the patient Suppose we have a patient who has croup; airway is swollen - as we intubate we inflate the cuff to a certain amount. As we give steroids to reduce the inflammation, the inflated cuff becomes too small as the swelling of the airway decreases and we end up having a leak. |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Endotracheal Tube in the Esophagus |
Waveform evaluation: A normal capnogram is the best available evidence that the ETT is correctly positioned and that proper ventilation is occurring. When the ET tube is placed in the esophagus, either no CO2 is sensed or only small transient waveforms are present. Is this happens, patient will not be breathing (respiratory distress, can't hear anything with the stethoscope). |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Faulty Ventilator Circuit Valve |
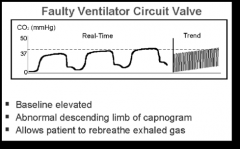
Wavelength evaluation: baseline is elevated; abnormal descending limb of capnogram; allows patient to rebreathe exhaled gas. Patient is rebreathing exhaled gas because it isn't going all the way down to the baseline; expiration is shortened. |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Cardiogenic Oscillations |

Cardiogenic Oscillations appear during the final phase of the alveolar plateau and during the descending limb. They are caused by heart beating against the lungs. Characteristics: - rhythmic and synchronized to heart rate - may be observed in pediatric patients who are mechanically ventilated at low RR (10 - 15 beats/min) with prolonged expiratory times. Peds/infants: the chest isn't completely ossified so heart beat tends to reverberate more than if the rib cage was ossified. It is easy for heart sounds to be reverberating into the airway. |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Muscle Relaxants (Curare Cleft) |
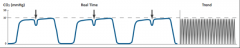
Cleft are seen in the plateau portion of the capnogram. They appear when the action of the muscle relaxant begins to subside and spontaneous ventilation returns. Characteristics: - depth of the cleft is inversely proportional to the degree of drug activity - position is fairly constant on the same patient, but not necessarily present with every breath. Curare = old type of muscle relaxant Muscle relaxants are given to a patient to relax de muscles so the patient doesn't have a constant signal of pain. When trying to intubate a patient that is fighting to get the procedure done (altered), we give a muscle relaxant, so he/she doesn't fight the machine. When the muscle relaxant starts to wear off, we have the cleft, because the patient starts to regain spontaneous breathing. Muscle relaxants work to relax all the respiratory muscles as well, so the patient cannot breathe on his own. Unless we give a sedative, the patient's mind is still active. Patients may panic if they are only given a muscle relaxant (their brain keeps on telling them to breathe but he cannot move). |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Obstruction in Breathing Circuit or Airway |
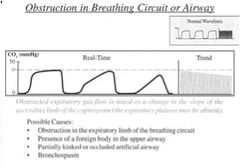
Obstructed expiratory gas flow is noted as a change in the slope of the ascending limb of the capnogram (the expiratory plateau may be present). Possible causes: - obstruction in the expiratory limb of the breathing circuit - presence of a foreign body in the upper airway (food - steak specially on alcoholic patients) - partially kinked or occluded artificial airway (if there is too much of the ETT or trach tube exposed it could bend) - bronchospasm (constricted airways = less room for CO2 to get out). |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Decreasing EtCO2 Level |
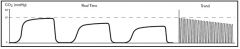
A decrease in the level of EtCO2 from previous levels Possible causes: - increse in RR (Hyperventilation) - increase in Vt (Hyperventilation) - decrease in metabolic rate - fall in body temperature (due to cold temperatures of water/weather) - More CO2 is being exhaled - we might see this in patients in risk for brain herniation that we have to hyperventilate. |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography Rebreathing |
Elevation of the baseline indicates rebreathing (may also show a corresponding increase of EtCO2) Possible causes: - faulty expiratory valve - inadequate inspiratory flow - malfunction of a CO2 absorber system - partial rebreathing circuits - insufficient expiratory time not enough time to exhale |
|
|
Non-invasive Monitoring End Tidal (EtCO2) Monitoring - Capnography EtCO2% to mmHg |
10% CO2 1. transform it into decimals = .10 2. multiply by 713 0.10 x 713 = 71.3 mmHg |