![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
30 Cards in this Set
- Front
- Back
|
What population is pyelonephritis most commonly seen in? |
Females |
|
|
How is the laboratory diagnosis of acute pyelonephritis made? (what lab criteria must be met) |
Pyruria Blood Cell Casts 10³-10⁵ organisms per ml |
|

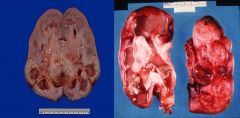
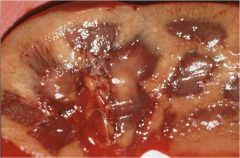
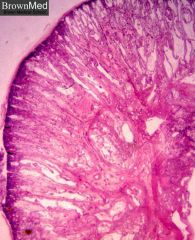
What pathologic characteristics are seen here?
What is the most likely diagnosis? |
Yellow streaks (pus = yellow-white color) Bulging cut surface Enlarged Inflammation of calyces and pelvis Petechial Hemorrhage
Acute Pyelonephritis |
|
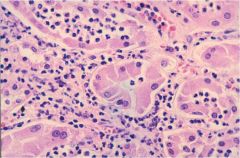
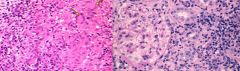
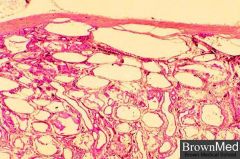
What pathological findings are observed?
What diagnosis is this consistent with and why? |
Intertubular PMNs PMNs in the interstitium
Acute Pyelonephritis since PMNs are characteristic of an acute bacterial infection. |
|
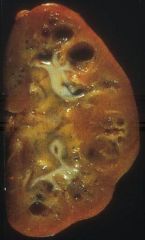
What pathology can be seen here?
What is this an example of? |
Dilated pelvis and calyces filled with pus
Pyonephrosis (complication of pyelonephritis) |
|
|
What is causes chronic pyelonephritis (CPN)? |
Chronic Obstruction (leads to recurrent acute infections and inflammation superimposed on obstructive lesions and thus scaring)
Reflux nephropathy (UTI superimposed on congenital VUR) |
|

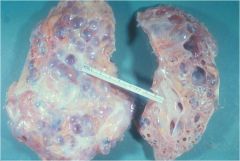
What pathology can be seen here?
What condition is this associated with? |
Irregular, discrete corticomedullary scars (pitted scars) Dilated, blunted calyces --- resemble deer antlers
Chronic Pyelonephritis |
|
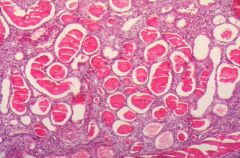
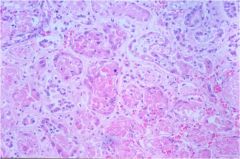
What pathology is seen here?
What is this pathology pathoneumonic for? |
"Thyroidization" (patchy atrophic tubules with hypertrophic, dilated surviving tubules filled with colloid casts)
Chronic Pyelonephritis |
|
|
What lab findings are seen in Chronic Pyelonephritis (CPN)? |
- bacteruria > 10⁵ per ml - low grade pyruria - hematuria - proteinuria - ↑ BUN - ↑ Cr |
|
|
What diagnosis should you think of in association with a proteus infection? |
Xanthogranulomatous Pyelonephritis |
|
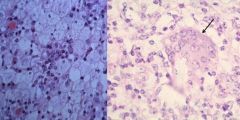
What pathology is seen on the left?
What is the arrow pointing to on the right?
What is the most likely diagnosis? |
Foamy macrophages mixed in with plasma cells, PMNs, and giant cells
The arrow on the right points to a multinucleated giant cell
|
|
|
What type of obstruction is associated with Xanthogranulomatous pyelonephritis? |
Staghorn Calculus |
|
What pathological features can be seen on the right and left?
What is the most likely diagnosis based on this pathology? |
Right: Interstitial Edema and Interstitial Infiltrate (primarily T lymphocytes and monocytes) Left: Granuloma formation, eosinophils, histiocytes
Acute Interstitial Nephritis (AIN) |
|
|
What diagnosis should you be thinking about when urine output < 400 ml per 24 hours |
Acute Tubular Necrosis (ATN |
|
What pathologic features can be seen here?
What is the most likely diagnosis? |
Cortex is very pale relative to the medulla (there is a sharp contrast)
Pale areas associated with necrosis
Acute Tubular Necrosis (ATN)
|
|
What pathologic features can be seen here?
What is the most likely diagnosis? |
Dead & dialated tubular cells (no nuclei) Glomeruli spared Hyaline and granular casts
Acute Tubular Necrosis (ATN)
|
|
What pathologic features can be seen here?
What is the most likely diagnosis? |
Enlarged Kidney, multiple cysts with variable sizes
Autosomal Dominant (Adult) Polycystic Kidney Disease - cysts in these individuals vary in size (if the patient was known to live past infancy likely ADPKD since ARPKD is usually fatal in infancy) |
|
|
What other pathology may be seen in individuals with Autosomal Dominant (Adult) Polycystic Kidney Disease (ADPKD)? |
Berry Aneurysm Mitral Valve Prolapse Cystic Liver Disease |
|
|
At what point in life do symptoms normally present in individuals with ADPKD? |
Middle age (most commonly 4th decade) |
|
What pathologic features are seen here?
What is the most likely diagnosis? |
Numerous cysts that are highly variable in size Cysts lined by simple epithelium Intervening parenchyma appears normal
ADPKD |
|

What pathologic features are seen here?
What is the most likely diagnosis? |
Enlarged Kidney Cysts are small relative to ADPKD Cysts are relatively symetric and uniform in size
Autosomal Recessive Polycystic Kidney Disease (ARPKD) |
|
|
What other pathology is present in individuals with Autosomal Recessive (Infantile) Polycystic Renal Disease (ARPKD)? |
Hepatic Cysts |
|
What pathologic features are seen here?
What is the most likely diagnosis? |
Cysts lined by uniform cuboidal cells Few glomeruli No normal parencyma
Autosomal Recessive PKD |
|
What pathologic features are seen here?
What is the most likely diagnosis? |
Small contracted kidney, Granular surface, Medullary Cysts (particularly at corticomedulary junction)
Medullary Cystic Disease (aka. Uremic Medullary Disease) |
|
|
What is the prognosis in Medullary Cystic Disease (aka. Uremic Medullary Disease)? |
Progress to renal failure 5-10 years after onset of symptoms |
|
|
Where in the kidney do cysts appear in Medullary Sponge Kidney? |
Pillary Collecting Ducts of the Renal Medulla |
|
|
What symptoms do individuals with Medullary Cystic Disease exhibit?
Why do they exhibit these symptoms? |
Polyuria & Polydipsia
Due to defect in concentrating ability |
|
|
What important correlation is there with Dialysis Cystic Disease (Acquired Cystic Disease)? |
Increased incidence of Renal Adenoma and RCC within the walls of the cysts |
|
|
How many pathogenic organisms must be present in order to diagnose pyelonephritis? |
> 10³ organisms/ mL |
|
|
In individuals that present with pyelonephritis and papillary necrosis is seen on biopsy, what condition are they likely to have? |
Diabetes mellitis |