![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
127 Cards in this Set
- Front
- Back
|
What are the pre-renal causes of AKI? |
1. Hypotension 2. Shock 3. Renal artery stenosis |
|
|
What are the intrinsic renal causes of AKI? |
1. Pyelonephritis 2. Drugs - NSAIDs - aminoglycosides (gentamycin) 3. Tubulointerstitial nephritis 4. Thromboemboli 5. Microscopic arteritis 6. HUS (thrombotic microangiopathy) |
|
|
What are the post-renal causes of AKI? |
Obstructive causes: - calculi - tumours - prostate enlargement - retroperitoneal fibrosis |
|
|
What causes chronic kidney failure? |
1. Diabetic nephropathy 2. Hypertension 3. Chronic pyelonephritis 4. Chronic glomerulonephritis 5. Polycystic kidney disease |
|
|
What is the pathophysiology of kidney damage in HUS? |
Microthrombi form on epithelium damaged by Shiga-like toxin. This leads to mechanical haemolytic (presence of schistocytes on peripheral blood smear) and platelet consumption. This process predominantly affects the kidneys, leading to acute renal failure due to ↓ renal blood flow. |
|
|
What is the pathophysiology of Goodpasture's syndrome (anti-GBM disease)? |
Auto-antibodies to glomerular basement membrane (BGM) attack the glomeruli and alveoli leading to type II (IgG mediated) hypersensitivity. Causes rapidly progressive (crescentic) glomerulonephritis. |
|
|
What is the histological appearance of the glomerulus in Goodpasture's syndrome?
|
Rapidly progressive (crescentic) glomerulonephritis. Linear membrane staining for IgG on immunofluorescence (due to anti-GMB autoantibodies). |
|
|
Which auto-antibodies are responsible for vasculitic glomerulonephritis? |
cANCA antibodies (Wegener) pANCA antibodies (microscopic polyangiitis) |
|
|
What is the pathophysiology underlying vasculitic glomerulonephritis? Which vasculitis syndromes is it associated with? |
Auto-antibodies trigger degranulation of neutrophils and fibrinoid necrosis producing rapidly progressing (crescentic) glomerulonephritis. No immune deposits in the glomeruli. Associated with Wegener's (cANCA) and microscopic polyangiitis (pANCA) |
|
|
Name 4 causes of autoimmune glomerulonephritis: |
1. Wegener's 2. Microscopic polyangiitis 3. SLE 4. Goodpasture's |
|
|
On the histological level, what is the distinction between nephritic and nephrotic syndrome? |
Nephritic - disruption of the glomerular basement membrane. Nephrotic - disruption of podocytes. |
|
|
What are the characteristic features of nephritic syndrome? |
Nephritic = inflammatory. 1. Haematuria + red cell casts 2. Proteinuria <3.5 g/day 3. Hypertension 4. Oliguria |
|
|
What are the characteristic features of nephrotic syndrome? |
Nephrotic = massive proteinuria 1. Proteinuria > 3.5g/day 2. Hypoalbuminaemia 3. Hyperlipidaemia |
|
|
An example of which syndrome - nephritic or nephrotic - is acute post-streptococcal glomerulonephritis?
|
Nephritic |
|
|
What causes rapidly progressive (crescentic) glomerulonephritis? |
1. Vasculitic glomerulonephritis - Wegener - microscopic polyangiitis 2. Goodpasture's 3. SLE 4. IgA nephropathy |
|
|
What are common causes of acute tubular necrosis? |
1. Ischaemia 2. Nephrotoxicity - NSAIDs - gentamycin |
|
|
What are common causes of tubulointerstitial nephritis? |
Drugs: - proton pump inhibitors - antibiotics - NSAIDs - diuretics |
|
|
What technique can be used to visualise changes present in the glomeruli in minimal change glomerulonephritis? What changes would be apparent? |
Electron microscopy - fusion and destruction of podocytes (not visible under light microscopy or immunofluorescence) |
|
|
What is immunofluorescence? |
Light microscopy with a fluorescence microscope used to visualise antibodies used to label biomolecule targets |
|
|
What is the aetiology of membranous nephropathy? |
80% idiopathic (antibodies to podocyte antigen) 20% associated with drugs, SLE, malignancy |
|
|
Is membranous nephropathy an example of nephrotic or nephritic syndrome? |
Nephrotic |
|
|
What is the pathophysiology of renal changes in diabetic nephropathy? |
Non-enzymatic glycosylation of: - GBM - leads to increase in permeability and thickening - Kimmelstiel-Wilson lesion - efferent arterioles - increases GFR and leads to mesangial expansion |
|
|
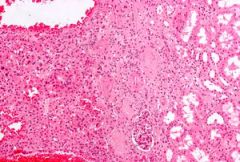
What is the appearance of renal tissue in diabetic nephropathy under light microscopy? |
1. Kimmelstiel-Wilson lesion - eosinophilic nodular glomerulosclerosis 2. Mesangial expansion 3. Thickening of GBM |
|
|
what is the commonest type of glomerulonephritis (produces nephritic picture)? |
IgA nephropathy |
|
|
What is the pathophysiology of IgA nephropathy? |
Mesangial immune complex deposits with mesangial proliferation. |
|
|
Name two disease processes which cause immune complex deposition in the kidneys, leading to nephritic syndrome. |
1. IgA nephropathy 2. Lupus nephritis |
|
|
Name 4 causes of renal cysts: |
1. Adult polycystic kidney 2. Childhood polycystic kidney 3. Medullary sponge kidney (medullary cystic disease) 4. Simple renal cysts |
|
|
What is a common iatrogenic cause of renal cysts? |
Long-term dialysis |
|
|
Which kidney tumours commonly have a cystic appearance? |
1. Wilms tumour 2. Cystic renal cell carcinoma |
|
|
What is a renal oncocytoma? What is its significance? |
Benign epithelial cell tumour - clinically mimics malignancy: - painless haematuria - flank pain - abdominal mass |
|
|
What is the histological appearance of renal oncocytoma? |
Large nests of benign cells with round nuclei and eosinophilic, granular cytoplasm. |
|
|
What types of tissues compose angiomyolipoma tumours? |
Muscle, vessels and fat |
|
|
What is the most common type of kidney cancer? |
Renal cell carcinoma (85% of malignant renal tumours) |
|
|
Name 5 risk factors for renal cell carcinoma: |
1. Male sex 2. Smoking (2x risk) 3. Obesity 4. End stage kidney disease 5. von Hippel Lindau syndrome |
|
|
What is von Hippel Lindau syndrome? |
Mutation of von Hippel-Lindau tumour suppressor gene causes: - haemangioblastomas - pheochromocytoma - multiple renal cysts → renal cell carcinoma |
|
|
Clinical presentation of renal cell carcinoma: |
Classic triad: (present in <10% cases)* 1. Haematuria 2. Loin pain 3. Abdominal mass Often presents with non-specific symptoms, paraneoplastic phenomena and/or metastases (1/3 of cases). *similar to presentation of renal oncocytoma - benign tumour |
|
|
Renal cell carcinoma is associated with ectopic production of which hormones? |
- EPO - PTHrP - ACTH |
|
|
What are the common paraneoplastic manifestations of renal cell cancer? |
1. Polycythaemia (ectopic EPO production) 2. Pyrexia of unknown origin |
|
|
What is the macroscopic appearance of renal cell carcinoma? |
- rounded to nodular - commonly has pseudo-capsule - haemorrhagic and necrotic areas - often partly/completely cystic |
|
|
What is the microscopic appearance of renal cell carcinoma? |
Clear cells with granular cytoplasm Sometimes eosinophilic cells Nuclei with prominent nucleoli |
|
|
What malignant tumours of the kidney are there? |
1. Renal cell carcinoma 2. Wilm's tumour 3. Transitional cell carcinoma of the renal pelvis |
|
|
What biological therapies can be used in renal cell carcinoma?
|
Tyrosine kinase inhibitors (sunitinib) |
|
|
When does Wilm's tumour commonly present? |
In children <5y |
|
|
What is the microscopic appearance of Wilm's tumour? |
Undifferentiated blastoma (comprises structures of developing foetal kidney - tubules, glomeruli, stroma) |
|
|
What types of kidney stones are there? |
1. Calcium oxalate/phosphate (70%) 2. Magnesium ammonium phosphate (15%) 3. Uric acid (5-10%) 4. Cystein (1%) |
|
|
What are the risk factors for developing kidney stones? |
1. ↑ amount of solute (i.e. hypercalcaemia) 2. ↓ amount of solvent (i.e. dehydration) 3. urinary stasis (i.e. obstruction) 4. occurrence of nidus (centre which the stone forms around) |
|
|
What are the clinical features of renal stones? |
1. Colicky pain 2. Haematuria 3. Obstruction → hydroureter and hydronephrosis 4. Recurrent or chronic infections (pyelonephritis) |
|
|
What can cause hydronephrosis? |
1. Pelvic-ureteric junction abnormality 2. Renal calculi 3. Tumour obstructing lower urinary tract 4. Vesico-ureteric reflux 5. Benign prostaticW hyperplasia 6. Prostate or bladder cancers |
|
|
What is the difference between pyelonephritis and pyonephrosis? |
Pyonephrosis - frank pus collection in the renal pelvis, calyces and interstitium Pyelonephritis - suppurative bacterial infection of renal pelvis, calyces and interstitial |
|
|
What are some predisposing factors to pyelonephritis? |
1. Congenital anatomic abnormalities 2. Diabetes 3. Immune suppression 4. Urinary stasis - calculi - prostate enlargement - retroperitoneal fibrosis |
|
|
What is the aetiology of adult polycystic kidney disease? |
Autosomal dominant defect of the APKD1 gene |
|
|
What is the aetiology of childhood polycystic kidney disease? |
Autosomal recessive |
|
|
What conditions are associated with adult polycystic kidney disease? |
1. Berry aneurysm 2. Aortic aneurysms 3. Spleen, pancreas and liver cysts |
|
|
What is a staghorn calculus? |
Renal calculus taking shape of renal pelvis and calyces |
|
|
What is the most common cause of formation of renal calculi? |
Urinary stasis
|
|
|
Which type of renal stones are most commonly seen in context of infection? |
Triple phosphate stones (ammonium magnesium phosphate) |
|
|
Which infections predispose to formation of ammonium magnesium (triple) phosphate stones? |
Urease +ve bacteria (i.e. Proteus, Klebsiella) that hydrolase urea to ammonia. Commonly form stag horn calculi. |
|
|
What is the common presentation of polycystic kidney? |
1. Hypertension 2. Abdominal mass 3. Loin pain 4. Recurrent infections 5. Renal calculi 6. Haematuria 7. Berry aneurysm |
|
|
Which conditions are known to lead to papillary necrosis of the kidney? |
POSTCARDS (Beethoven) Pyelonephritis Obstruction Sickle cell disease TB Cirrhosis of liver Analgesic/alcohol abuse Renal vein thrombosis Diabetes Systemic vasculitis |
|
|
What are the complications of a horseshoe kidney? |
Infections Pelviureteric obstruction |
|
|
What epithelium lines the urinary tract? |
Transitional (urothelium) |
|
|
What type of bladder cancer is most common? |
Transitional cell carcinoma |
|
|
What types of bladder cancer are there? |
1. Transitional cell carcinoma 2. Squamous cell carcinoma 3. Adenocarcinoma |
|
|
What are the risk factors for transitional cell carcinoma of the bladder? |
Pee SAC: - phenacetin - smoking - aniline dyes - cyclophosphamide |
|
|
What is the usual first presentation of bladder cancer? |
Painless haematuria |
|
|
What investigations would you perform on a patient who presented with painless haematuria to look for cancer? |
1. Urine cytology 2. Cystoscopy +/- biopsy 3. CT 4. IVU |
|
|
What are the histological features of urothelial carcinoma? |
Resembles normal transitional epithelium but thicker, lacks differentiation towards the surface, cells pleomorphic and increased nucleus:cytoplasm ratio |
|
|
What radiographic tests can be used to visualise the urinary tract? |
CT KUB IVU (intravenous pyelogram) - contrast imaging |
|
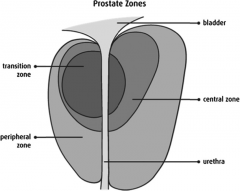
Which zone of the prostate is the common site for carcinoma? |
Outer peripheral zone |
|
|
What symptoms are associated with benign hyperplasia of prostate? |
Hesitancy Poor flow Terminal dribbling Frequency Urgency Nocturia |
|
|
Other than urinary symptoms, what complications are associated with BPH? |
1. Bladder smooth muscle hypertrophy with trabeculation and diverticula 2. Acute urinary retention 3. Infections 4. Hydronephrosis |
|
|
Which investigations would you perform to investigate a suspected prostate cancer? |
1. PR 2. PSA test 3. Transrectal ultrasound 4. Needle biopsy |
|
|
What form of bony metastasis is associated with prostate cancer? |
Instead of osteolytic lesions like in majority of metastatic deposits, in most cases prostate cancer causes osteosclerotic deposits |
|
|
What is the histological appearance of prostate cancer? |
95% adenocarcinoma - numerous small glands - loss of basal cell layer - loss of architecture - pleomorphism |
|
|
What is prostatic intraepithelial neoplasia? |
Pre-cancerous precursor lesion with hallmarks of dysplasia that has not invaded past the basal cell layer into the prostatic stroma yet |
|
|
What staging system is used for prostate cancer? |
Gleason score |
|
|
What type of testicular tumours are there? |
1. Germ cell tumours - seminoma - non-seminoma - mixture 2. Sex cords/stromal tumours - Leydig cells - Sertoli cells 3. Lymphomas/leukemias |
|
|
What is the precursor lesion to germ cell tumours of the testes? |
Germ cell neoplasia in situ |
|
|
What are the risk factors for developing germ cell testicular cancer? |
1. Cryptorchidism 2. Infertility 3. Hormonal influences 4. Family history |
|
|
What is the typical population affected by germ cell tumours of the testes? |
Males 22-55 |
|
|
What is the microscopic appearance of seminoma? |
Large cells with watery cytoplasm and vesicular nuclei |
|
|
What serum markers have the greatest predictive value in diagnosis of testicular cancer? |
1. LDH 2. AFP (alpha-fetoprotein) 3. hCG 4. PLAP |
|
|
What is PLAP a marker for? |
Seminoma (not a standalone marker - rises with smoking) |
|
|
Other than seminoma, what types of germ cell testicular cancer are there? |
1. Embryonal carcinoma 2. Choriocarcinoma 3. Teratoma 4. Yolk sac tumour |
|
|
What is the standard treatment for testicular cancer? |
Orchidectomy +/- chemotherapy |
|
|
Which of the three markers: α-fetoprotein, βhCG or LDH is the best marker of tumour burden? |
LDH |
|
|
Which testicular cancer is associated with raised α-fetoprotein? |
Yolk sac tumour |
|
|
Which testicular cancer is associated with raised βhCG? |
choriocarcinoma |
|
|
Which organisms can lead to inflammation of testes? |
Chlamydia trachomatis Neisseria gonnorhoeae E coli TB Mumps |
|
|
What risk factors are a predisposition to developing UTI? |
1. Female 2. Age 3. Anatomical abnormalities of the urinary tract 4. Indwelling catheter 5. Immunosuppression (including diabetes) 6. Sexual intercourse 7. Exposure to spermicide |
|
|
Clinical features of uncomplicated UTI: |
1. Dysuria 2. Frequency 3. Urgency 4. Suprapubic tenderness |
|
|
What factors can complicate UTI? |
- abnormal renal/genitourinary tract, - voiding difficulty, - impaired renal function, - impaired host defences - virulent organism (i.e. Staph aureus) |
|
|
Why can UTI be more dangerous in pregnant women? |
↑↑↑ risk of pyelonephritis |
|
|
Complications of UTI: |
1. Pyelonephritis 2. Papillary necrosis 3. Abscess 4. Sepsis |
|
|
What is emphysematous pyelonephritis? |
Infection with gas-forming E coli, citrobacter and others causes severe necrotising multifocal bacterial nephritis. Extraluminal gas seen in parenchyma and perirenal space on abdo x ray. Always requires nephrectomy. |
|
|
Which population of patients is especially susceptible to emphysematous pyelonephritis? |
Diabetics |
|
|
What is xanthogranulomatous pyelonephritis? |
Severe, chronic inflammation of the kidney with focal destruction of renal parenchyma. Renal tissue is replaced with lipid-laden, foamy macrophages |
|
|
What does +ve leukocyte esterase on urinalysis signify? |
Presence of ↑ WCC = pyuria |
|
|
What could cause sterile pyuria? |
1. Previous antibiotics 2. Tumours 3. Fastidious organism 4. STI |
|
|
Which antibiotic commonly used to treat UTI would be contraindicated in pregnancy, and why? |
Trimethoprim - inhibitor of folate deficiency |
|
|
What is the significance of nitrites on urinalysis? |
Bacterial metabolite - convert nitrates to nitrites |
|
|
What is the preferred antibiotic to use in uncomplicated UTI in a non-pregnancy female? What is the alternative? |
1. Nitrofurantoin (concentrated in urine) 2. Trimethoprim |
|
|
What is the preferred antibiotic treatment for acute pyelonephritis? |
Co-amoxiclav (for sepsis add single gentamicin) |
|
|
What are some potential confounding factor making urea an imperfect way to measure renal function? |
1. Low in liver failure 2. High after protein meal 3. High in GI bleed 4. High in dehydration |
|
|
What are some potential confounding factor making creatinine an imperfect way to measure renal function? |
Related to muscle mass |
|
|
What is the equation for renal clearance? |
Clearance = ([a]urine x urine flow rate)/[a]plasma |
|
|
What would be the level of urine glucose in tubular interstitial nephritis? |
Increased due to reduced ability of the kidneys to reabsorb glucose |
|
|
What are the two mechanisms driving hypocalcaemia and consequent bone disease in renal failure? |
1. ↓ active vit D 2. ↑ phosphate due to impaired excretion |
|
|
What is the definition of clearance? |
Volume of plasma completely cleared of a substance in a given time |
|
|
What is maximum clearance rate equal to? |
GFR |
|
|
What is an example of overflow proteinuria? |
Bence-Jones proteins in multiple myeloma/ Waldenstrom's macroglobulinaemia |
|
|
What is an example of glomerular proteinuria? |
Albumin in diabetic nephropathy |
|
|
What is an example of tubular proteinuria? |
Impaired reabsorption of normal filtered protein - i.e. β2-microglobulin |
|
|
What is an example of secreted proteinuria? |
Increased secretion of Tamm-Horsfall protein - most abundant protein in normal urine |
|
|
What is Fanconi syndrome? How does it present? |
General reabsorptive defect in PCT; presents with increased urinary excretion of nearly all amino acids, glucose, bicarbonate and phosphate. |
|
|
What is a complication of Fanconi syndrome? |
Proximal renal tubular acidosis. |
|
|
What causes Fanconi syndrome? |
Hereditary (i.e. Wilson disease) Multiple myeloma Nephrotoxins Ischaemia |
|
|
Name three causes of aminoaciduria: |
1. Fanconi syndrome 2. Phenylketouria 3. Cystinuria |
|
|
What is the pathophysiology of cystinuria? What are the complications? |
Defect of a COAL transporter (specific amino acid transporter) in the tubules. Complications: formation of cystine stones. |
|
|
What are the electrolyte changes observed in normal anion gap acidosis? |
Loss of HCO3- is compensated by increase in Cl- |
|
|
What is Type 1 renal tubular acidosis? |
Due to reduced tubular secretion of H+ in DCT |
|
|
What is the pH of urine in type 1 tubular acidosis? |
Alkaline > 5.3 |
|
|
What electrolyte disturbance can be a consequence of type 1 renal tubular acidosis? |
Hypokalaemia (instead of H+, K+ is excreted in exchange for Na+) |
|
|
What is the treatment for type 1 renal tubular acidosis?
|
1. Bicarbonate 2. Potassium |
|
|
What is type 2 renal tubular acidosis? |
Increased loss of HCO3- due to reduced reabsorption in PCT
|
|
|
What is type 4 renal tubular acidosis? |
Hypoaldosteronism → hyperkalaemia Inhibition of ammonia excretion in proximal tubule → urine becomes more acidotic as buffering capacity falls → |
|
|
What is the pH of urine in type 2 tubular acidosis? |
< 5.5 |