![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
128 Cards in this Set
- Front
- Back
|
What is the most common renal cyst? |
Cortical cyst |
|
|
Cortical Cyst |
hangs off cortex - considered acquired lesions possibly arising from ducts or tubules |
|
|
Which Renal Cyst: - 50% of population older than 50 - ASYMPTOMATIC - incidental finding |
Cortical Cyst |
|
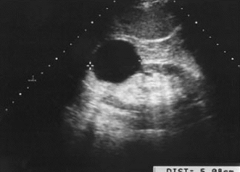
Which type of renal cyst? |
Cortical cyst |
|
|
Ultrasound cannot determine between types of cysts, but can determine....? |
Location |
|
|
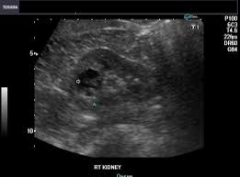
Peripelvic Cyst |
renal sinus / center of kidney |
|
|
Complex cysts are considered.... |
malignant until proven otherwise |
|
|
U/S of Complex Cysts |
- thick walls (< 1 mm, malig) - internal echoes (infection, hemorrhage) - thin septations (may be normal but if contains vascularity, likely malig) - fine calcifications in wall or septum |
|
|
Any irregularity at base of cyst is considered... |
malignant growth |
|
|
Bosniak Classification |
Catergory 1 - 0% malig Category 2 - 0% malig Category 2F - 5% malig Category 3 - 50% malig Category 4 - 100% malig |
|
|
Category 1 Bosniak Classification |
- simple, benign - thin walls - no calcifications - no septations - no atypical features *NO further evaluation |
|
|
Category 2 Bosniak Classification |
- cystic lesions - ONE or TWO thin septations < 1mm - fine calcifications in walls/septa - appear HYPERECHOIC but contain all other features of Category 1 cysts - 3cm or less in depth - 25% of wall OUTSIDE kidney walls - NO vascularity |
|
|
Category 2F Bosniak Classification |
minimally complicated cysts (doesn't look like category 1 or 2) *FOLLOW-UP 6 months-1 year |
|

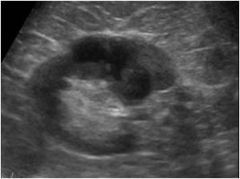
Which Bosniak classification? |
category 2 |
|
Which Bosniak Classification? |
Category 2F |
|
|
Category 3 Bosniak Classification |
- uniform wall thickening - nodularity : esp. at base - thick/irregular peripheral calcification - multiloculated - multiple vascular septa *REQUIRE biopsy or surgery to evaluate |
|
Which Bosniak classification? |
Category 3 |
|
Which Bosniak classification? |
Category 3 |
|
|
Category 4 Bosniak Classification |
- diffuse wall thickening - walls increased vascularity - large nodules - CLEARLY solid vascular component *presumed RENAL CELL CARCINOMA - only tx - nephrectomy |
|
|
Which Bosniak classification is presumed renal cell carcinoma? |
Category 4 |
|
Which Bosniak classification? |
Category 4 |
|
|
Parapelvic Cyst |
- originates from renal parenchyma - likely lymphatic in nature - does NOT communicate w/ collecting system - asymptomatic unless very large |
|
|
Do Parapelvic cysts communicate with collecting system? |
NO |
|
Which renal cyst? |
Parapelvic |
|
|
U/S Parapelvic Cyst |
- well-defined mass with NO internal septations - may cause obstruction if located in MEDIAL LOWER portion |
|
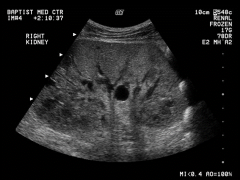
Which type of renal cyst? |
Parapelvic |
|
|
Von Hippel-Lindau Disease (VHL) |
autosomal dominant genetic disorder - abnormal growth of tumors throughout body (retinas, adrenals, kidneys, pancreas) Typically cortical cysts |
|
|
Acquired Cystic Kidney Disease |
- found in native kidney of patients w/ renal failure who are undergoing dialysis - incidence INCREASES with time (typically after 3 years dialysis, 90% after 5 years) |
|
|
U/S of native kidney with acquired cystic kidney disease |
small, echogenic w/ multiple simple cysts |
|
|
If Chronic Renal Failure, how many cysts per kidney? |
3-5 cysts - internal echoes common (represent hemorrhage) |
|
|
What is Acquired Cystic Kidney disease associated with? |
increased incidence of Renal Cell Carcinoma |
|
54 year old w/ end-stage renal disease...which pathology? |
Acquired cystic kidney disease |
|
|
Autosomal Recessive PKD (ARPKD) |
- infantile (IPKD) - fatal - 4 forms |
|
|
U/S Autosomal Recessive PKD (ARPKD) |
- bilat, enlarged kidneys - diffusely echogenic - hyperechoic - loss of cortical medullary distinction |
|

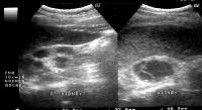
Fetus - which renal pathology? |
Autosomal recessive PKD (ARPKD) |
|

Fetus - which renal pathology? |
Autosomal recessive PKD (ARPKD) |
|
|
Newborn PKD types 1 and 2 |
1. Perinatal (before birth) 2. Neonatal (after birth) *both present at birth *rapid renal failure leads to death in infancy |
|
|
U/S of Newborn PKD |
- oligohydramnios - nephromegaly |
|
|
Childhood PKD types 3 and 4 |
3. Infantile 4. Juvenile *occurs 3-5 years *affects LIVER (hepatic fibrosis) |
|
|
U/S Childhood PKD |
liver echogenic w/ multiple liver cysts |
|
|
4 things associated w/ IPKD |
1. renal dysfunction 2. pulmonary hypoplasia 3. periportal fibrosis 4. portal HTN |
|

Which renal pathology? *pediatric |
Infantile Polycystic Kidney Disease (IPKD) |
|
|
with Autosomal Dominant PKD / Adult PKD, patients are usually....? |
hypertensive |
|
|
U/S Adult PKD |
multiple irreg cysts bilat in massively enlarged kidneys *cysts may also be in spleen, liver, pancreas |
|
|
What occurs in 20% of Adult PKD cases? |
Berry aneurysm (in circle of Willis) |
|

Which renal pathology? |
Adult PKD |
|
|
Which renal pathology: - usually nonhereditary disease - may be unilateral or bilateral (fatal if bilateral) - most common form of cystic disease in neonates - believed to occur in utero as result of urinary tract obstruction |
Multicystic Dysplastic kidney disease (MCDK) |
|
|
Which renal pathology:
appears as large, noncommunicating cysts interspersed with echogenic areas and an absence of renal parenchyma? |
Multicystic dysplastic kidney disease |
|
|
What can occur if Multicystic dysplastic kidney disease is unilateral and not removed?? |
- HTN, hematuria, infection, flank pain - increase incidence of malig |
|

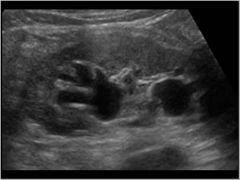
Which renal pathology? *this image is a pediatric case |
Multicystic dysplastic kidney disease |
|

Which renal pathology? |
Multicystic dysplastic kidney disease |
|
|
What is the development anomaly occurring in medullary pyramids and consists of cystic or fusiform dilatation of distal collecting ducts? |
Medullary sponge kidney *unknown etiology |
|
|
What does Medullary Sponge kidney cause? |
stasis of urine and stone formation *due to this, calcium deposits form in tubules |
|
|
U/S Medullary Sponge Kidney |
hyperechoic medullary pyramids *may be unilateral or segmental |
|
|
4 things associated with Medullary Sponge Kidney |
1. Beckwith-Wiedemann syndrome (overgrowth disorder) 2. PKD 3. Caroli's Disease 4. Congenital hepatic fibrosis |
|
|
U/S Medullary Sponge Kidney |
- loss of corticomedullary differentiation - multiple medullary small cysts - hyperechoic calyces (with or without stones) |
|

Which renal pathology? |
Medullary sponge kidney |
|
|
First indication of a renal neoplasm |
abnormal renal contour |
|
|
Complex (solid, calcifications) renal masses are considered... |
malignant until proven otherwise 10-15% have mets @ diagnosis |
|
|
If you find a mass that is likely to be malignant, what else should you check? |
- IVC and renal vein for thrombus/tumor - contralateral kidney, liver and retroperitoneum for mets |
|
|
Adenoma, Oncocytoma, Angiomyolipoma, and Tuberous Sclerosis are all...? |
BENIGN |
|
|
What is the most prevalent benign kidney tumor? |
Adenoma |
|
|
Usual size of Adenoma? Where do they originate from? |
1-3cm originate from : renal tubular epithelium |
|
|
Which benign renal neoplasm is highly vascular and mimics renal cell carcinoma? |
Adenoma *must be differentiated via histology |
|
|
What is the very large, vascular form of Adenoma? |
Oncocytoma |
|
|
Which renal neoplasm: - occurs middle to old age - typically asymptomatic (maybe hematuria or pain) - difficult to differentiate from RCC |
Oncocytoma |
|
|
If an Oncocytoma has a central stellate scar....? |
infarct from outgrowing blood supply *doesn't rule out RCC but helps differentiate |
|
|
Renal Angiomyolipoma (AML) composed of? |
composed of fat, blood vessels, and muscle |
|
|
Which renal neoplasm: 80% cases in females 80% in R kidney found in 80% patients with tuberous sclerosis |
renal angiomyolipoma (AML) |
|
|
Which renal neoplasm: - usually hyperechoic - not very large - primary complications include intratumoral hemorrhage and organ displacement |
renal angiomyolipoma (AML) |
|
|
D/D renal angiomyolipoma |
maybe small RCC's |
|
|
What is the genetic disease that causes benign tumors to grow on various organs (kidneys, brain, heart, eyes, skin, lungs) ? |
Tuberous Sclerosis |
|
|
People with Tuberous Sclerosis have increased incidence of...? |
renal cysts and angiomyolipomas (bilat) |
|
|
Renal Cell Carcinoma AKA..... |
Hypernephroma Adenocarcinoma Grawitz's tumor |
|
|
What is the most common of ALL renal neoplasms? (85%) |
renal cell carcinoma |
|
|
Which renal neoplasm: - twice as common in men (6-7th decade of life) - appears bilateral (typically good news) |
renal cell carcinoma |
|
|
Clinical presentation of RCC |
nonspecific but maybe: hematuria (most common) flank pain palpable mass *only 15% present w/ all three |
|
|
What are RCC's likely to produce? |
Hormones (can cause endocrine symptoms) |
|
|
U/S of Renal cell carcinoma |
- unilateral focal mass - varied echogenicity - partially cystic or calcified |
|
|
A complete ultrasound study (if a suspected RCC) must include: |
1. renal vein (involved 20-30% of time) 2. IVC (mets more common on R than L) 3. para-aortic lymph nodes and renal hilum nodes 4. contralateral kidney |
|
|
Renal cell carcinoma can metastasis to...? LLLBC |
local lymph nodes lungs liver bone contralateral kidney |
|
|
Prognosis of Stage 1 RCC |
tumor WITHIN kidney 80-100% 5 year survival rate |
|
|
Prognosis of Stage 2 RCC |
tumor confined to fascia 65-75% 5 year survival rate |
|
|
Prognosis of Stage 3 RCC |
tumor has regional mets 25-50% 5 year survival rate |
|
|
Prognosis of Stage 4 RCC |
distant mets 0-20% 5 year survival rate |
|
|
What percent of patients with RCC have lung mets upon diagnosis? |
1/3 |
|
|
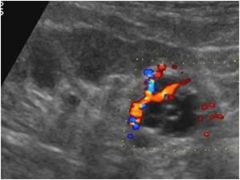
Doppler characteristics of RCC |
- vascularity in 95% - vessels typically within tumor - LOW RI - renal vein and IVC invasion 5-24% of cases |
|
|
Normal Renal vein and IVC Doppler vs. presence of thrombus or obstruction |
normal - low velocity, PHASIC flow abnormal - damped flow, absent flow, continuous flow |
|
What stage of RCC would you say this is? Survival rate? |
stage 3 25-50% |
|

What stage of RCC would you say this is? Survival rate? |
stage 1 80-100% |
|
|
What makes up 90% of all UROTHELIAL carcinomas? |
Transitional cell cancer (TCC) |
|
|
Prognosis of Transitional cell cancer |
90% 5 year survival rate (after removal) |
|
|
Which renal neoplasm: - 90% of all renal pelvis tumors - 7% of all renal tumors - ~61 years old, men |
Transitional cell cancer |
|
|
Which renal neoplasm: - painless hematuria - tumors small and bilat (too small to see via ultrasound) |
Transitional cell cancer |
|
|
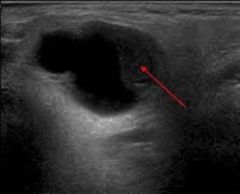
U/S Transitional cell cancer |
- only LARGE tumors seen with u/s - thickening of urothelial lining - * INTRALUMINAL mass - shape of tumor will match space it fills - solid mass in renal sinus - splitting of central echo similar to hydro (but not cystic) - bulky hypoechoic mass |
|
|
What may TCC be confused with? How to differentiate? |
prominent renal papillae in presence of hydronephrosis - RCC will only be in affected pyramids, papillae would be in ALL |
|
Which renal neoplasm? |
Transitional cell cancer |
|
Which renal neoplasm? *note echogenic material filling the ureter |
Transitional cell cancer |
|
|
Which renal neoplasm: - rare - highly invasive - poor prognosis - chronic infection/irritation - gross hematuria - palpable kidney due to severe hydro |
squamous cell carcinoma |
|
|
Which renal neoplasm: - "diffusely enlarged kidney that maintains shape" - renal echotexture destroyed & replaced by stone - 50% of cases - large mass in renal pelvis - may be obstruction from stones |
squamous cell carcinoma |
|
|
2 forms of renal Lymphoma |
1. primary - rare (3%) 2. secondary - more common |
|
|
How does Secondary renal lymphoma occur? |
hematogeneous spread (90%) OR direct extension via LYMPHATIC channels spread by Non-hodgkin's more common than Hodgkin's |
|
|
Which renal neoplasm: - BILAT enlarged kidneys - tumors hypoechoic compared to pyramids - may appear as renal cyst but WILL NOT have posterior enhancement |
renal lymphoma |
|
|
Ill-defined hypoechoic renal tumors can be easily mistaken for....? |
renal CYSTS *tumor will have NO POSTERIOR ENHANCEMENT |
|
|
Mets to the kidney usually comes from...? |
lung, breast, colon, renal cell carcinoma from contralateral kidney |
|
|
When is mets to the kidney typically found? |
autopsy *rare to find in life |
|
|
Why is mets to the kidney common? |
LARGE amount of blood flow through kidneys |
|
|
What is the most common childhood renal tumor? |
Nephroblastoma / Wilms' tumor |
|
|
2 most important considerations with Wilms' tumor |
1. can the tumor be resected ? 2. unilateral or bilateral ? |
|
|
What is the most common solid renal tumor in patients 1-8 years old? |
Wilms' tumor *peak incidence at 2.5-4 years *more common in males |
|
|
Wilms' tumor occurs 2-8x more commonly in patients with...? |
HORSESHOE kidney |
|
|
Which renal neoplasm: - large asymptomatic flank mass - hematuria - fever - malaise - HTN |
Wilms' tumor |
|
|
U/S of Wilms' tumor |
- large - well-circumscribed - smooth mass - echogenicity slightly greater than liver - renal vein or IVC thrombus |
|
|
Occurence of Renal vein / IVC thrombus with Wilms' tumor |
40% have thrombus at time of diagnosis |
|
|
What needs to be determined (on u/s) with a Wilms' tumor? |
- whether SOLID or CYSTIC - renal in origin |
|
|
If you see what looks to be a Wilms's tumor, but renal contour is UNAFFECTED bilaterally, most likely...? |
ADRENAL neuroblastoma ** Wilms' will DESTROY renal contour |
|

Which renal neoplasm has this typical appearance? |
Wilms' tumor / Nephroblastoma |
|
|
IVC thrombus and Wilms' tumor |
|
|
What is the precursor to Wilms tumor? |
Nephroblastomatosis *found in 25% unilateral Wilms *found in 100% bilateral Wilms |
|
|
2 forms of Nephroblastomatosis |
1. Pancortical - replaces renal parenchyma 2. Superficial - subcapsular rind of primitive tissue surrounded by NORMAL renal tissue |
|
|
U/S of Superficial Nephroblastomatosis |
- thick rim of hypoechoic tissue - irregular central contours - smooth outer contours |
|
|
Kidney size - Nephroblastomatosis |
LARGE |
|

*note HUGE kidneys *9 month old |
Nephroblastomatosis |
|
|
Mesoblastic Nephroma AKA Fetal Renal Hamartoma |
BENIGN - composed of connective tissue REPLACING normal renal parenchyma (nephrons being replaced) |
|
|
What is the most common solid renal mass in the first 3 months of life? *rare in older children and adults |
Fetal Renal Hamartoma / Mesoblastic Nephroma |
|
|
S/S of Fetal Renal Hamartoma |
- asymptomatic abdominal mass - hematuria - HTN |
|
|
U/S Fetal Renal Hamartoma |
- preservation of renal shape until tumor becomes LARGE - echogenic with low-level echoes *more heterogenous than Wilms' - in large masses: hemorrhage, necrosis, cyst formation |
|
2 month old, presents with asymptomatic abdominal mass and hematuria |
Fetal Renal Hamartoma / Mesoblastic Nephroma |