Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
13 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
What are the hallmarks of nephritic syndrome?
|
Hematuria
RBC Casts Mild to moderate protinuria |
|
|
|
Describe post-infectious glomerulonephritis from its onset to cure
|
-Infection (S. Pyogenes) causes release of high levels of compliment
-Compliment deposits in the subepithelial layer of the GBM -Nephritic syndrome caused by neutrophills. -Eventualy self curing upon destruction of compliment |
|
|
|
What population is this disease most severe in?
|
Adults, 40% of affected adults progress to fulminant CKD
|
|
|
|
What is the most common cause of nephritic syndrome worldwide?
|
IgA nephropathy (Berger's Disease)
|
|
|
|
What is the pathogenesis of IgA Nephropathy?
|
-Increased IgA secretion due to a genetic mutation
-IgA secretions get trapped in the mesangium and activate the complement pathway. |
|
|
|
Describe the history of a typical IgA nephropathy patient
|
Adult, intermitent hematuria.
May progress to RPGN or CRF |
|
|
|
What would you suspect in a child with IgA nephropathy and palpable purpura on her legs and bottox?
|
Henoch-Schoenlein Purpura
|
|
|
|
Rapidly progressing glomerulonephritis has what characteristic pathological finding on biopsy?
|
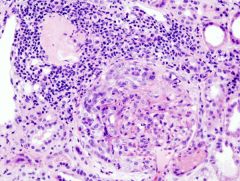
Crecent shaped glomeruli
How are these created? |
Fibrin leaks into the glomerular capillaries
|
|
|
What is the pathology of Alport's Syndrome.
|
A mutation in the genes which compose type IV collagen.
This leads to dysfunction of the GBM, hearing dysfunction, and respiratory dysfunction What would you expect to see clinically in a patient with Alport's |
Males (the disease is mostly X-linked) with hematuria. Family Hx of hearing loss, renal failure, etc.
NO Ig on the biopsy |
|
|
A young male presents with intermittent hematuria, no Hx of infection or viremia.
Normal urinalysis. Normal biopsy on H&E. What disease is it? |
Benign familial hematuria
|
|
|
|
Differentiate RPGN type 1 from type 2
|
Type 1 - Breaks in the GBM with linear IgG deposition.
Type 2 - Direct injury to the endothelial cells mediated by Ig with granular deposits |
|
|
|
List 3 causes of RPGN type II
|
-Postinfections
-Lupus -IgA nephropathy (or HSP) |
|
|
|
Pauci-immune glomerulonephritis (RPGN III) gets its name from the fact that there are no Ig deposits seen.
What diseases cause this? |
Small vessel diseases
Wegner's Granulomatosis (c-ANCA) Churg-Strauss (p-ANCA) |
|