![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
31 Cards in this Set
- Front
- Back
|
Proximal tubule first part? second part? where in the kidney? |
PCT 60% Proximal straight tubule 40% in the cortex |
|
|
what feature does PCT have for ↑ absorption |
microvilli → brush border |
|
|
Secondary active transport in PT types of transporters few examples? |
ion chanels exchangers cotransporters |
|
|
Primary active transport in PT types of transporter example? |
pumps |
|
|
Transcellular movement in PT |
through cell |
|
|
paracellular movement in PT |
between cells |
|
|
Water absorption in PT how much water is absorbed in PCT? |
Na+ movement makes osmotic gradient for water to follow water moves transcellularly + paracellularly passively through AQP1 PT is water permeable implying filtrate is almost isotonic with interstitial space i.e. effectively isotonic with plasma NB not isosomotic which is a different thing 70% of water is absorbed by the end of the PCT |
|
|
Na+ movement in PT |
down electrochemical gradient into epithelial cells drives movement of other substances e.g. glucose and AAs and water (by making osmotic gradient) uses Na+/K+ ATPase to move Na+ out at basolateral |
|
|
why does water flow paracellularly? |
because of net outward hydrostatic pressure in tubule and osmotic forces |
|
|
Water transport SUMMARY |
paracellularly through tight junctions of the epithelial cells AQP1 transporter apical side, exits AQP1 basal side of epithelial cells |
|
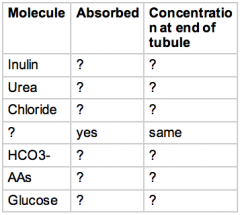
Table of molecules along PT |
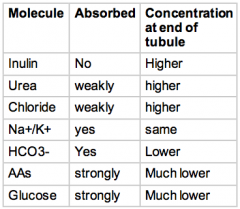
think of what substances the body really wants to keep top 3 conc ↑ because 70% water has been reabsorbed |
|
|
Glucose transport Early PT |
Apical SGLT 2: Na+ + Glucose Basal GLUT 2: Glucose |
|
|
Glucose transport Late PT want to absorb more Na+ than early PT? |
Apical SGLT 1: 2Na+ + Glucose Basal passively GLUT 1: Glucose harder to absorb Glucose distally as [glucose] ↓ |
|
|
SGLT 2 |
low affinity high apacity 90% |
|
|
SGLT 1 |
high affinity low capacity 10% distal PT |
|
|
Max tubular load |
2.1 mmol/min
this is tubular maximum transport |
|
|
Tubular maximum transport glucose |
maximum rate of absorption of glucose |
|
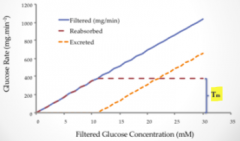
Describe the graph |
If GFR is constant amount filtered proportional to [filtered glucose] once glucose >≈12mM reabsorption is limited to 400mg/min and glucose excretion ↑ difference b/w filtered & reabsorbed → excretion of a substance in this case glucose Maximum Tubular transport = is max b/w reabsorbed and x axis e.g. glucosuria in DM |
|
|
Canagliflozin Dapagliflozin class of drugs? indication? mechanism? paradoxical Sx? |
SGLT 2 inhibitors
-gliflozin? Rx for DM mechanism: inhibit SLGT 2→ glucosuria → ↓ blood sugar levels Sx: ↑ risk of UTI cystitis |
|
|
AA Tm? general trend of transport? movement by charge? |
Max tubular transport Tm is limited many many different transporters (similar to those from DIG) Gradient of Na+, H+ Neutral AAs move together Positiv AAs move together |
|
|
HCO3- draw a diagram of the absorption? which drug interacts with this? what's special about the _N+/_K+ exchanger? (think NAS) |
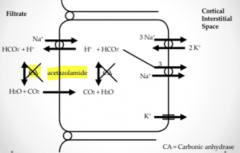
Acetazolamide -Na+/H+ exchanger is the most important -CO2 diffuses through and reabsorbed back into blood -3Na+/2K+ exchanger -Na+/3HCO3- cotransporter on basolateral side -HCO3- is driving reabsorption of Na+ normally the other way round in nephron -main mechanism is removal by reacting with excess H+ -CA ↑ rate at which eqm is reached |
|
|
Acetazolamide what type of drug is it? indications? mechanism? implications of mechanism |
weak diuretic NOT REALLY USED AS DIURETIC indications: Glaucoma mountain sickness - HCO3- Na+ and water stay in the filtrate mechanism:stops Carbonic anhydrase from working implications of mechanism: so get metabolic acidosis urine is alkaline -both of these are becauses HCO3- is not reabsorbed |
|
|
Acetazolamide and Mountain sickness |
ascending to altitude, hypoxia, ↑ respiratory rate, [CO2] ↓, get respiratory alkalosis, since gives metabolic acidosis helps to return to normal pH |
|
|
how much HCO3- is in the filtrate? |
25mM |
|
|
Cl- methods of reabsorption? draw the diagram. |
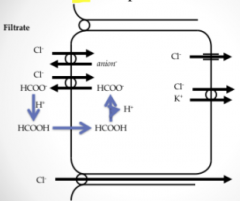
active and passive main active Cl-/Anion exchanger e.g. - Cl-/HCOO- - Cl/HCO3- to avoid running out of anions to pump into filtrate, HCOO- recycling, helps drive the Cl- uptake Paracellular bulk flow? -HCOO- reacts Cl-/K+ Na+/H+ exchanger |
|
|
HCOO- in terms of Cl- reabsorption |
in filtrate reacts with acidic environment → methoanoic acid |
|
|
why does [Cl-] ↑ along the length of the PT? |
given absorption of HCO3- with charge difference balanced by Na+ absorption less Cl- is moved than Na+ in early PT given water is reabsorbed with Na+ and HCO3- this means that [CL-]↑ slightly along PT distal PT is more permeable to Cl- than HCO3- or other anions so paracellular reabsorption of Cl- happens |
|
|
Albumin in PT |
little albumin enters filtrate some does and binds plasma membrane of epithelial cells → catabolised to AAs for recycling in the body |
|

Organic anion secretion in PT |
PAH 9(p-aminohippuric acid) - organic anion Furosemide Penicillin these compete for excretion OAT (organic anion transporter) Basolateral membranes MRP Multidrug resistance associated Protein |
|
|
MINOR Na+ reabsorption in PT |
ENaC epithelial Na+ channels Na+ channels more prominent in later part of PT allowing 2º active transport |
|
|
MINOR Na+ reabsorption in PT diagram |
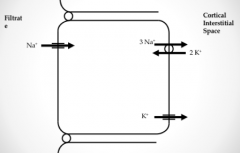
Apical side ENaC Basolateral side 3Na+/2K+ K+ channel |