Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
32 Cards in this Set
- Front
- Back
|
N Di
ser Na? urine? |
N up
urine dilute |
|
|
siadh
ser na urine |
n down
urine conct |
|
|
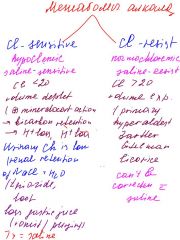
central CI
ser na urine |
na up
urine dilute |
|
|
Pp
ser Na urine |
na down \
urine dilute |
|
|
addison
na k |
na down
k up |
|
|
cushing
na k |
na up
k down |
|
|
gastric outlet obstruction
electrolytes acid base dis |
persist vomit--> dehydration>>volume contr>>>> hypokalemic hypochloremic metabolic alcalosis
hypoK due to renal K loss in effort to retain H+ and from hyperaldesteronism ( it's due to volume contr) emer Tx- NG hydra with saline iv K supplements ammonium chlo could be use in the setting of hypochloremic metab acidosis in order to lower pH in ECF and urine but it will increase diuresis and will worsen the condition of P in use as mono therapy diuresis |
|
|
hypercalcemia-
|
hypercalcemia- non spec symp
and pain constip polyria neuropsych dist acute tx saline folow by loop thasides will worse |
|
|
succinil choline, what contind
|
hyperkalemia
( could lead to) burned and crashed truama |
|
|
met alkalosis
|
|
|
|
hypocalcemia in alcash
|
|
|
|
renal failure Ca ph
|
ca down
ph up sec hyperparat |
|
|
primary hypoparath ca ph
|
ca down ph up
|
|
|
malabs in alcash ca ph
|
both down because vit D rise the both
other case of concordant Ca and Ph down- pancreatitis |
|
|
ort hypoten
diziness dry membrane low serum na and k high urine na and k |

|
|
|
low calory intake .... electr
|

|
|
|
vomiting electr
|

|
|
|
mineralocort def, electr
|

|
|
|
diuretic use for weigh loss electr
|

|
|
|
cushing
|
|
|
|
if increased ca and incr/ norm PTH what it could be
|
mst likely primary hyperparat
or hypocalciuric hypercalcemia in second will be low ca in urine in first will be inreased ca excretion |
|
|
loops were given
what IS in ABG |
1.LOOPS INHIBIT NA/K/Cl COTRANSPORT >>>>>increased excretion of NA ( more Na in urine)( natiuria)
2. also incresed K excre>>> ( hyperkaleuria) >>>hypokalemia 3.increased distal solute delivery and increase Aldesterone level, that will >>> in increased H+ excretion, this will lead to metab alkalosis |
|
|
acute renal failure-- electr?
|
hyperkalemia and metab acidosis
|
|
|
opioids ABG?
|
>>>> hypoventila >>> respir acidosis ( accumul of CO)
|
|
|
if P with cirrosis.. look for ....
|
most like tx is with Loops
complications hypokalemia metab alcalosis renal failure |
|
|
vomiting
|
vomitng>> hypochloremia, hypokalemia
elevated bicarb level Gi flid is rich in H and KCl and loss of it will result in ( read above) loss of H will increase the concentration of bicarb( see on blood gase pH .7.4) 2 vomiting causes the volume contraction>>> to activation RAA system which stimulate the bcarb reabsorbtion realize that volume contr and bicarbreabsorb are the result of hydrogen loss , not cause if it why hypokalemis?>> 1 Gi loss 2.intracellular shift of K caused by alkalosis 3 incr renal secretion of K cause by aldoseron( aldesteron is ramped up by RAA system as ameans to retain fluid tx- isotonic NA CH and K |
|
|
why hypokalemia is hard to correct in alcoholics
|
chr alc have multiple electr abnorm
hypoK hypoPh and hypoMg hypoMg cause the refractory hypoK Mg is a co factor for K uptake and maintence intracellular K level check and correct Mg level in alkash |
|
|
pregnancy AGB
|
high progest >> stimul respir cenc>>> tachypnea>> chronic respir alkalosis.
progest conce is increase in late pregnancy and eventually it will be also metabolic acidosis as compens we will see Mild repira alkalosis with ph > 7.4 and primary decrease in Pco1 and compens decrese in HCO3 |
|
|
grand mal seizures
|
post ictal state >> lactic acidosis- AG met acidosis.
muscle breakdown >>increase lactic acid and degrease hepatic lactate uptake post ictal acvidosis is transient and will resolve in 30-60 min TX-= check ABG in 2 hours again no tx need if not resolve- look for other reason for acidosis |
|
|
2 phases of hypokalemic hypochloremic metabolic acidsosis
|
1 phase generation phase
- loss of gastric fluid- HCh, nacl and h2o -loss of HCL ND NACl >> TO UNBALANCE RETAINING OF H2CO3 -BECAUSE NO ACIDITY IN GASTRIC,.. NO STIMULI TO RELEASE THE BICARB BY PANCREAS...instead bicarb is retain in blood and lead to ... METAB ALKALOSIS 2 phase- maintance because of volume loss>> decrease the volume pressure>> activate RAA system ( kidney responce) aldosteron try to retain water for expense of H and K loss in urine. Aldosteron >> to hypokalemia and contraction alkalosis. thi si will be maintenance phase for metab alkalosis from vomiting tx saline and k |
|
|
hypocalcemia after trauma
|
usually and after operation also, when will be multiple blood transfusion
look for case with hemorrhage and trauma usually hypocalcemia will be from volume expansion and hypoalbuminemia usually will be asymptomatic, because ionized ca in normal but when after transfusion that ca will be bind by citrate.. symptoms as hyper deep reflexes could occur. muscle crams or even convulsions too. severe hypomagnesemia may mimic hypocalcemia because it decrese PTH secretion and decrease periferal resposiv to PTH |
|
|
mild hypermagnesemia
|
decrese deep refl
severe >> loss of deep tendon refl and muscle paral apnea and cardiac arrest |