Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
9 Cards in this Set
- Front
- Back
|
achalasia- defenition
|
A motor disorder of the esophagus characterized by impaired relaxation of
the lower esophageal sphincter (LES) and loss of peristalsis in the distal twothirds of the esophagus. Thought to result from the loss of inhibitory interneurons in Auerbach’s plexus |
|
|
history
|
Progressive dysphagia, chest pain, regurgitation of undigested food, weight
loss, and nocturnal cough are common symptoms. ■ 2°causes of achalasia include malignancy (gastric carcinoma, lymphoma) and Chagas’ disease. 2° achalasia may present with greater weight loss and a shorter duration of symptoms in older patients. |
|
|
ds
|
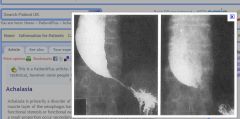
Barium swallow reveals esophageal dilation with a “bird’s beak” tapering
of the distal esophagus (see Figure 2.6-1). ■ Manometry shows ↑ resting LES pressure with incomplete relaxation upon swallowing and ↓ peristalsis in the body of the esophagus. ■ Endoscopy may be helpful for excluding 2° causes of achalasia. |
|
|
tx
|
Nitrates, CCBs, or endoscopic injection of botulinum toxin into the LES may
provide short-term relief of symptoms. Pneumatic dilation or surgical myotomy may result in long-term relief |
|
|
tx
|

|
|
what that
|
what
|
|

|
d
|
|
|
relief of achalasia in patients who because of age or comorbidities are not candidates for endoscopic or surgical intervention.
|
* Botulinum toxin injection can afford relief of achalasia in patients who because of age or comorbidities are not candidates for endoscopic or surgical intervention.
|
|
|
pseudoachalasia
|
Patients with pseudoachalasia tend to be older than patients with achalasia, have a shorter duration of symptoms, and have greater weight loss. Neither barium esophagography nor esophageal manometry can distinguish between primary and secondary achalasia. In this case, a history of lymphoma and the presence of a submusosal lesion require further evaluation. Endoscopic ultrasonography will allow delineation of the depth and invasiveness of the lesion, as well as permit transluminal needle biopsy of the mas
|