![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
144 Cards in this Set
- Front
- Back
|
Abbreviations and directional terms: Left and Right |
L or Le
R or Rt |
|
|
Abbreviations and directional terms: Medial and Lateral |
M
L |
|
|
Abbreviations and directional terms: Cranial and Caudal |
Cr
Cd |
|
|
Abbreviations and directional terms:
Cranial and Caudal is in reference to anything ____ to the _______ on extremeties |
proximal to the carpus/tarsus |
|
|
Abbreviations and directional terms: Dorsal and Ventral |
D
V |
|
|
Abbreviations and directional terms: Palmar and Plantar |
Pa
Pl |
|
|
Abbreviations and directional terms: Palmar and Plantar refers to anything _____ to the _________ |
distal to the carpus/tarsus |
|
|
Abbreviations and directional terms: Proximal and Distal |
Pr
Di |
|
|
Abbreviations and directional terms: Oblique and Rostal |
O
R |
|
|
Terms used for describing the position of patient designates the _______ of the X-ray beam |
direction |
|
|
_________ or _____ states where X-ray beam enters the body |
1st letter or term |
|
|
_________ or ______ states where X-ray beam exits body |
2nd letter or term |
|
|
When you combine two terms, the combination of the _____ and the _____ ______ is used.
Ex. |
root and the combining vowel ( usually “o”)
Ex. Dorso-ventral Palmaro-dorsal Cranio-caudal |
|
|
Right and left are not used in combination with other terms and should ________ any other terms.
Ex. |
precede
Ex. Right lateral |
|
|
Medial and lateral go ______ when used with other terms.
Ex. |
second
Ex. dorso-medial
|
|
|
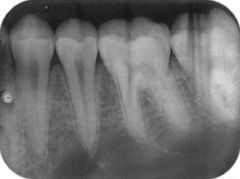
What body parts do we typically radiograph? (8) |
Skull Dental Thorax Abdomen Pelvis Spine Forelimb Hindlimb |
|
|
What are the common views we take of the skull, spine, pelvis, thorax and abdomen? (4) |
V/D D/V R lateral L lateral |
|
|
X-rays enter the patient on its dorsal aspect and X-rays exit the patient on its ventral side |
Dorso-Ventral (DV) radiograph |
|
|
X-rays enter the patient on its ventral aspect and X-rays exit the patient on its dorsal side |
Ventro-Dorsal (VD) radiograph |
|
|
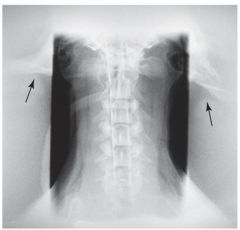
Beam enters on the patient’s right side and exits on patients left side or visa-versa |
Lateral radiographs |
|
|
Lateral radiographs with patient laying on Left side
|
Left lateral |
|
|
Lateral radiographs with patient laying on Right side |
Right lateral |
|
|
What are the common views we take of the forelimb and hindlimb? (6) |
Cranial/caudal(Proximal to the carpus/tarsus) Caudal/cranial(Proximal to the carpus/tarsus)
Dorsal/Palmar(Distal to the carpus/tarsus) Palmar/Dorsal(Distal to the carpus/tarsus)
Dorsal/Plantar(Distal to the carpus/tarsus) Plantar/Dorsal(Distal to the carpus/tarsus) |
|
|
Usually used for skull and extremities. “Neither perpendicular nor parallel.” |
Oblique views |
|
|
Oblique views are named by stating ______ _____ of ______ first then if it is______ or _______, then stating ____ _____ and if it is _______ or ______. |
entrance side of limb medial or lateral exit side of limb medial or lateral |
|
|
Oblique view of horse carpus taken from the front with the x-ray machine positioned towards middle of horse’s body |
Dorsal-Medial-Palmaro-Lateral Oblique |
|
|
Oblique view of horse carpus taken from the back with the x-ray machine positioned away from midline |
Palmaro-Lateral-Dorso-Medial Oblique |
|

|
q |
|
|
3 Goals of obtaining a diagnostic radiograph |
Get an image of the area of interest
Patient safety and welfare
Operator and assistant safety |
|
|
Area of interest should be in ________ _____ |
primary beam |
|
|
Center of X-ray beam centered over _____ of _______ |
area of interest |
|
|
In patient safety and welfare remember.... (7) |
Be patient, can be scary for the animal
Some (most) positions are uncomfortable
Go slowly and quietly
Do not over restrain, especially cats
Be gentle but firm
Desensitize to rotor noise
Get as much preparation done before positioning the patient as possible |
|
|
Some preparation that should be done before positioning the patient (6)
|
Measure patient Setting exposure technique Positioning the cassette Making the label Gathering positional aids Donning protective gear |
|
|
Operator and assistant safety rules (4) |
Distance: Stand back, lean back, look away Shielding: Proper use of PPE, use restraint aids Time: Correct settings(increased mAs will decrease time) and COLLIMATE DO IT RIGHT THE FIRST TIME |
|
|
Patient positioning aids must be made of ________ material if over or under area of interest |
radiolucent |
|
|
Patient positioning aids may be ________ or _________ if placed outside area of interest. |
radiolucent or radio-opaque |
|
|
Some positioning aids may include(7) |
Sandbags, bean bags, compression bands Foam wedges Wood blocks Tape, radiolucent trough Gauze, rope, bungee cords Cloth leashes Chemical restraint |
|
|
Collimation is also known as "_______ _____." |
"coning down" |
|
|
The coal of collimation is to produce ____ _____ ______ and still get ___ ____ _____ in the image |
smallest field possible area of interest |
|
|
How much collimation is enough? |
"goldilocks rule" not to big, not too small, juuuust right. |
|
|
Proper collimation is important to reduce _____ ______ which can reduce _____ _____ and therefor reduce diagnostic value. |
scatter radiation; radiographic contrast |
|
|
Proper collimation makes for a more _____ ____ image and has less ______. |
visually appealing; less |
|
|
The best way to ensure patient welfare and the safety of the operator and assistant is to: |
DO IT RIGHT THE FIRST TIME!!!!!!!!!!!! |
|
|
A radiograph is ___ dimensional representation of a ___ dimensional object |
2;3 |
|
|
Some issues with radiographic views is there is a loss of ____ _______ and objects directly behind another can be ______ by the one in front. |
depth perception; obscured |
|
|
2 views at ______ ______ are required to allow depth perception. This is called _______ views. |
right angles (90°); Orthogonal |
|
|
Limbs generally require ______ views to view all carpal or tarsal bones |
oblique |
|
|
Patient preparation small animal (3) |
Clean patient
Remove collars, halters, etc
Remove bandages and splints if possible |
|
|
Patient preparation horses (4) |
Remove shoes and nails
Clean frog of foot to remove debris
Clean the area well
Pack sole with play-doh (Prevents air artifacts that can be misinterpreted as fractures of hoof wall or coffin bone) |
|
|
When performing radiographic study of limbs it is often a good idea to ____ ______ ___ ___ ________ |
radiograph opposite limb for comparison. |
|
|
Limbs should have the proximal and distal _____ of the area of interest in the view. Sometimes this is not possible in really large animals. |
joints |
|
|
Dividing film in ½ and taking both limbs on same piece of film |
Split views |
|
|
If taking split views area of interest should face ___ _____ in both views |
same direction |
|
|
During abdominal radiology gut should be free of ______ and _______ _______. |
ingesta and fecal material |
|
|
During abdominal radiology image should be taken at _____ _________. |
full expiration |
|
|
Why is an abdominal radiograph taken at full expiration? |
So diaphragm is in dome shape |
|
|
During abdominal radiology ________ and _______ are most commonly taken |
Right lateral and VentroDorsal |
|
|
Thoracic radiographs are generally taken during _____ ________. |
full inspiration |
|
|
On thoracic radiographs expiratory radiographs cause lungs to appear _________. |
pneumonic |
|
|
Occasionally we take expiratory radiographs to evaluate ____ of _______ |
patency of trachea |
|
|
During thoracic radiology traditional radiographic views are the _______ and _____ ________. This is so we see standard views of the _______. |
VD and right lateral; heart |
|
|
During thoracic radiology right lateral allows us to see what is going on in the _____ lung |
left |
|
|
During thoracic radiology if masses are suspected in the right lung, must take a _____ ____ view |
left lateral |
|
|
"_______" is critical for thoracic views |
“Squareness” |
|
|
During thoracic radiology even slight rotation can accentuate_________, __________, and _______ errors |
magnification, elongation, and foreshortening |
|
|
During thoracic radiology magnification, elongation, and foreshortening errors can cause ______ of the ______ to appear distorted leading to misdiagnosis. |
chambers of the heart |
|
|
Radiographic Check List (8) |
Properly labeled, and indicated? Exposure factors? Centered? Borders and collimation? Patient properly positioned? No gloves!!!! Properly processed? Minimal artifacts? |
|
|
Radiograph is a ______ record. |
legal |
|
|
ID must be permanently embedded in _______. “Sharpie” labels not acceptable. |
emulsion |
|
|
Old images must be kept for a minimum of ___ years but better to keep until _______ ______. |
7; animal dies |
|
|
Types of Film/Image Identification (4) |
Clinic/Patient Information
Directional Markers
Special Studies
Gravity Marker |
|
|
Patient Information Label should include (3)
|
Name and address of clinic (name of doctor may be helpful)
Date
Patient ID (Owner name and patient name. age, sex and breed are helpful. Can be an ID number that refers to this information) |
|
|
Clinic/Patient Information Methods (2) |
Add when taking radiograph
Add before processing |
|
|
Methods to add Clinic/Patient Information when taking radiograph(2) |
Lead lettering
Leaded tape(Write on tape with ball-point pen) |
|
|
Methods to add Clinic/Patient Information before processing(1) |
Blocker in film cassette prevents certain area of film from being exposed during radiograph procedure
Flash system – uses unexposed area of film to place information (Some systems must remove film from cassette while some cassettes have a window that opens)
|
|
|
When adding clinic/Patient Information be careful not to.... |
cover up anatomic areas with label |
|
|
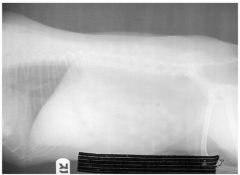
Placement of Patient Information labels: Abdominal views |
Place label towards tail |
|
|
Placement of Patient Information labels: Thorax views |
Place label towards head |
|
|
Placement of Patient Information labels: Limb views |
Place label towards distal end in all views (cranial-causal, lateral or oblique) |
|
|
Types of Directional Markers are ____ _____ indicating position |
lead letters |
|
|
These lead directional letters include (examples) |
Right or Left
Dorsoventral (DV) or Ventrodorsal (VD)
Angle DorsoLateralPalmaroMedial Oblique (DLPaMO) etc. |
|
|
Directional Markers should be used to identify: Skull/trunk |
Left or Right side |
|
|
Directional Markers should be used to identify: Extremities (3) |
Which one (left or right)
Hind or forelimb (Especially important when performing metacarpal, metatarsal, fetlock, pastern or navicular studies on horses)
The view (DMPaLO, PaLDMO, etc) |
|
|
Directional Markers should be used to identify: Abdominal views. where are these ideally placed? |
Lateral; ventrally just cranial to rear legs if possible |
|
|
Directional Markers should be used to identify: Thoracic views. Where are these ideally placed? |
Lateral; ventrally just caudal to front legs if possible |
|
|
Directional Markers should be used to identify: Abdominal and thoracic markers should indicate which side is ____. |
down |
|
|
Directional Markers should be used to identify: Abdomen and thorax (2) |
Dorsal ventral (DV) or Ventral dorsal (VD) views
Marker should indicate which side (right or left) |
|
|
Directional Markers should be used to identify: Abdomen directional markers should be placed ______. |
caudally |
|
|
Directional Markers should be used to identify: Thorax directional markers should be placed ______. |
cranially |
|
|
Directional Markers should be used to identify: Extremities: Cranial-Caudal (CrCd) |
Place marker on Lateral side of limb |
|
|
Directional Markers should be used to identify: Extremities: Lateral
|
Place marker on Cranial or Dorsal side of limb
|
|
|
Directional Markers should be used to identify: Extremities: Oblique |
Place marker on Dorso-lateral side of limb |
|
|
Markers outside of the light field projected by the collimator probably will ____ ____ __. |
not show up |
|
|
In Special Studies film identification sequentially taken radiographs are labeled with ____ _____. Not to be confused with ____ _____. Give examples. |
elapsed time; clock time
T= 0 T= 10 minutes T= 30 minutes T= 1 hour |
|
|
In Gravity Markers film identification markers indicate that patient is _______. |
standing |
|
|
When displaying films they should be viewed in a _______ _____ so film does not appear too light. |
darkened room |
|
|
When displaying films ventro-dorsal and dorso-ventral films should be viewed with ______ towards top of view box/screen and _____ side of body should be on the left. |
head; right |
|
|
When displaying films lateral films should be viewed with the _____ end to the left and ____ end to the top. |
cranial; dorsal |
|
|
Common radiographic distortions (3) |
Foreshortening
Elongation
Magnification |
|
|
Often more than one _______ occurs at the same time. Example |
distortion
Example- craniocaudal view of femur: Magnification and foreshortening of the distal end of the bone |
|
|
_________ is the foreshortening, magnification, or elongation of a body part |
Distortion |
|
|
Distortion is due to angulation of the _____ ____, the ____ _______, or the ______. |
body part, the x-ray receptor, or the tube |
|
|
Distortion can be useful when ..... |
one body part obscures the area of interest |
|
|
Foreshortening is in result of angulation of the ______ ______. |
body part |
|
|
|
x-ray tube, image receptor |
|
|
Magnification of a body part is reduced if the body part is placed ... |
as close as possible to the image receptor |
|

|
Elongation |
|

|
Foreshortening |
|

|
Magnification |
|
Motion during a radiograph results in a ______ image |
blurred |
|
|
Motion during a radiograph which causes a blurred image is referred to as _____ ________. |
geometric unsharpness |
|
|
The following factors can contribute to geometric unsharpness (3) |
Film movement
Patient movement
Tubehead movement |
|
|
Some common error for movement of patient are ______ and __________ movement. |
cardiac and respiratory |
|
|
Cardiac and respiratory movement can be improved with faster _____ _____. |
exposure time |
|

Can be in result of failure to depress exposure button or pedal properly |
Partial or no exposure |
|
|
Partial or no exposure can result in film being too ____ or ___ _____ at all. |
light; no image |
|
Can be in result of operator depresses exposure button more than once |
Double exposure |
|
|
Double exposure can result in _____ _____ on one film. |
two images |
|

Can be in result of operator using nails to grasp film or bending edges of film |
Bent film |
|
|
Bent film from nails will look like a large _____ on the film, otherwise it will appear as a _____ in the film. |
comma; crease |
|
Can be in result of hardware in the primary beam |
Artifacts |
|
|
Artifacts often include things like |
collars and halters, hands/gloves, labels in field of interest. |
|

Can be in result of moving film too quickly across a surface. |
Static electricity |
|
|
Static electricity looks like _______ on the film. |
lightening |
|
|
Other common artifacts: Will appear as grey or white line on film |
hair or dirt |
|
Other common artifacts: Will appear as streaky straight lines on a radiograph |
Grid deterioration |
|
|
Other common artifacts: Appears as a dark line of edge of the film |
Partial exposure of film to light |
|

Other common artifacts: Film will take on an overall grey appearance due to unsuitable storage conditions and exposure of film to light |
Film fog |
|
Other common artifacts: Areas outside of collimation is exposed |
Scatter radiation |
|
Other common artifacts: Film will lack density and must be distinguished from low mAs |
Development problems: weak developer, |
|
|
Other common artifacts: Portion of film not developed; retains color of undeveloped film |
Development problems: incomplete immersion |
|
Other common artifacts: Will appear as dark lines on the film due to improper cleaning of processor |
Roller marks |
|
Other common artifacts: Will appear milky in appearance and turns brown in color over time |
Weak fixer/too short of time in fixer |
|

Other common artifacts: Will appear like crystal on film or water spots |
Rinsing errors: fixer dries on film |
|
|
Technique evaluation: What two main question should we ask ourselves? |
1. Do you like this film?
2. Is there proper penetration of the subject? |
|
|
Do you like this film? If not is it ...... |
too light or too dark? |
|
|
If a film is too light we must.... |
increase either kVp or mAs |
|
|
If a film is too dark we must.... |
decrease either kVp or mAs |
|
|
Is there proper penetration of the subject (can you see through or inside patient)? If penetration is proper we must..... |
Adjust mAs |
|
|
Is there proper penetration of the subject (can you see through or inside patient)? If penetration is NOT proper we must..... |
Adjust kVp |
|

If image is too light, but properly penetrated we must...... |
increase mAs by 30 – 50% |
|
|
If image is too light, but Improperly penetrated we must...... |
Increase kVP by 10 – 15% |
|
|
If the image is too dark, but properly penetrated we must...... |
Decrease mAs by 30 – 50 % |
|

If the film is too dark but Improperly penetrated we must....... |
Decrease kVp by 10 – 15% |