![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
19 Cards in this Set
- Front
- Back
|
Hokett SD, Honey JR, Ruiz F, Baisden MK, Hoen MM. J Am Dent Assoc 2000. |
LatexFinger cots used in conjunction with the standard plastic sheaths to cover DDRsensors were more effective in preventing cross-contamination than plasticsheaths alone. |
|
|
RichardsAG. Dent Radiogr Photogr 1980. |
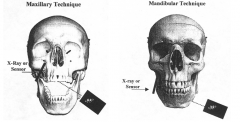
Buccal object rule: When two different radiographs are made of apair of objects, the image of the buccal object moves, relative to the image ofthe lingual object, in the samedirection that the X-ray beam is directed. |
|
|
ForsbergJ. Oral Surg Oral Med OralPathol 1987. |
The parallelingtechnique provides more accurate working length determination than thebisecting-angle technique. Up to 10 degreesof increased angulation with the bisecting-angle technique is as accurate asthe paralleling technique. |
|
|
Forsberg J, Halse A. Int EndodJ 1997. |
The bisecting-angle technique and theparalleling technique provide similar diagnostic results. |
|
|
Newman ME, Friedman S. J Endod 2003 |
|
|
|
Priebe WA, Lazansky JP, Wuehrmann AH. OralSurg Oral Med Oral Pathol 1954. |
Radiographs should not be used to differentiatethe nature of periapical pathosis; a poor correlation exists betweenradiographic and histologic diagnosis. |
|
|
Brynolf I. Swed Dent J 1970. |
Overall diagnosticaccuracy was 78% using one radiograph which increased to 92% using threeradiographs which included an Orthoradial view with 50mm tubular diaphram, aEccentric view and a Orthoradial view with 20mm tubular diaphragm (SO). |
|
|
Tamse A, Kaffe I, Fishel D. Oral Surg Oral Med OralPathol 1980. |
The zygomatic arch interferes with apices of 15- 23.8% of maxillary first molars and 38.7- 48.2% of maxillary second molars. |
|
|
PhillipsJL, Weller RN, Kulild JC. J Endod 1990. (Part 1) |
The most common location of the mental foramenwas inferior to the crown ofthe 2nd premolar and approximately 60% of the distance from the buccal cusp tipof that tooth to the inferior border of the mandible. The mental foramen most commonly exits in aposterior-superior direction 68.7%. The average horizontal dimension was 4.6mm, the average vertical dimension was 3.4 mm. |
|
|
Phillips JL, Weller RN, Kulild JC. J Endod 1992. (Part 2) |
The radiographic size of theforamen was smaller than the anatomical size previously reported. The averageposition of the mental foramen was 2.18 mm mesial and 2.41 mm below theradiographic apex of the second premolar on horizontal PA radiographs. |
|
|
Phillips JL, Weller RN, Kulild JC. J Endod 1992. (Part 3)
|
Theaverage horizontal dimension of the mental foramen was 2.9 mm and vertical 2.5mm.
The average position of the mentalforamen was 0.13 mm mesial and 3.0 mm below the radiographic apex of the 2ndpremolar on a panoramic radiograph. Panoramic radiography resulted in a distal shift of the foramen and a 23% magnification factor |
|
|
Bender IB, Seltzer S. Part I. J Am Dent Assoc 1961
|
Lesions incortical bone can be detected radiographically only if there is perforation ofthe bone cortex, erosion from the inner surface of the bone cortex, orextensive erosion or destruction from the outer surface. Lesions in cancellous bone cannot be detected radiographically.
|
|
|
Bender IB, Seltzer S. Part 2. J Am Dent Assoc 1961 |
Lesions were detected radiographically only whenthey encroached upon the junction of cancellous and cortical bone. Lesionsconfined to cancellous bone could not be detected radiographically. Apices ofanterior and premolar mandibular teeth lie near the buccal cortical plate.First molar apices may be near the buccal, lingual, or lie in cancellous bone.The second molar apices usually lie in cancellous bone or near the lingualplate. |
|
|
Lequire AK, Cunningham CJ, Pelleu GB. J Endod 1977. |
Using high kVp and the long-cone technique, 84%of the artificially produced periapical lesions, confined within the cancellousbone of jaw sections, were visible radiographically. |
|
|
Bender IB. J Endod 1980. |
12.5% bone loss (6.6% mineral bone loss) was the minimumneeded to produce a radiolucency in cortical bone. At 14.3% bone loss (7.1%mineral bone loss) all examiners agreed a radiolucency in cortical bone couldbe seen. Most 1-7 mm lesions in the cancellousbone did not produce a radiolucent area. |
|
|
Lee SJ, Messer HH. Int Endod J 1986. |
Periapical lesionsconfined to cancellous bone were detected radiographically in experimentallycreated ‘halo’ lesions with removal of the lamina dura and simulated scleroticborders. Cortical involvement is not a necessary condition forradiographic identification of periapical lesions. |
|
|
Goldman M, Pearson AH, Darzenta N. Oral Surg Oral Med Oral Pathol1972. |
When interpreting radiographs for success andfailure, examiners agreed on fewer than half of the cases. When asked todetermine only if an area of rarefaction was present on one film, the agreementwas still less than half. The greatestpercentage of disagreement occurred in the maxillary molar region. |
|
|
Goldman M, Pearson AH, Darzenta N. Oral Surg Oral Med Oral Pathol 1974. |
Radiographicinterpretation is a questionable process at best. Examiners evaluated radiographs 6 to 8 monthsafter their initial evaluation. When interpreting radiographs for success andfailure examiners agreed with themselvesfrom 72% to 88% of the time. |
|
|
KaffeI, Gratt BM. J Endod 1988. |
The mostconsistent radiographic features aiding in the diagnosis of the periradicularconditions were: 1) continuity and shape of the lamina dura and 2) width andshape of the PDL. |