![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
128 Cards in this Set
- Front
- Back

|
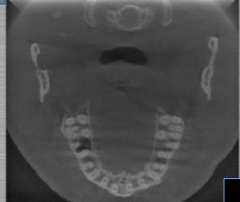
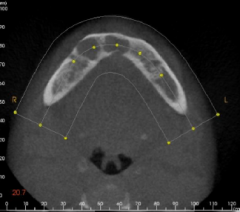
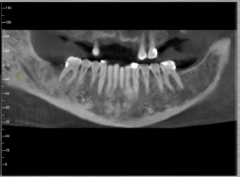
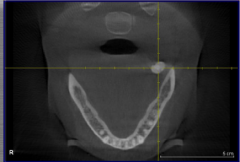
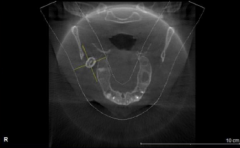
CBCT axial mandible |
|

|
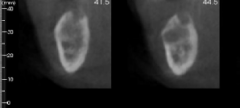
CBCT coronal |
|
|
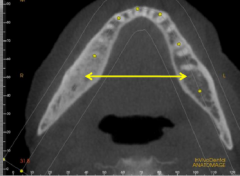
CBCT axial maxilla |
|
|
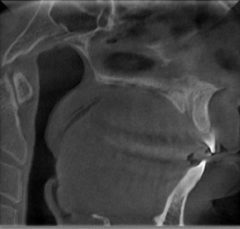
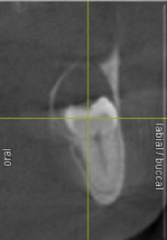
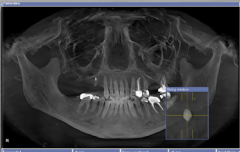
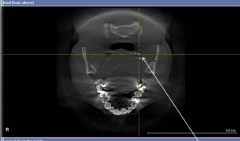
CBCT sagittal |
|
|
Orthogonal planes and anatomical terms: axial |
posterior, anterior, R, L |
|
|
Orthogonal planes and anatomical terms: sagittal |
superior, inferior, ant, post |
|
|
Orthogonal planes and anatomical terms: coronal |
superior, inferior, R, L |
|
|
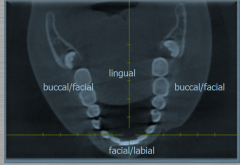
location terms in axial slice |
|
|

|
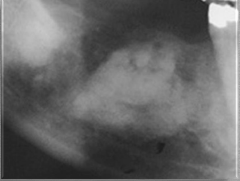
Nasopalatine duct cyst |
|

|
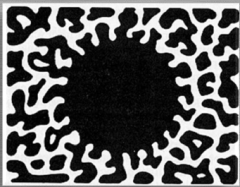
Paget's |
|

|
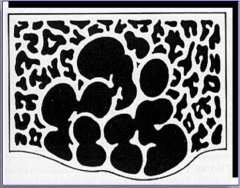
fibrous dysplasia |
|
|
What is DMSLSIE? |
He says he uses "LESION" L - location E - edge S- size I - internal architecture O - other structures N - number (unilateral/bilateral)
it really stands for d- density m- margin s- size l- location s- shape i- internal architecture e- effects on surrounding structure |
|
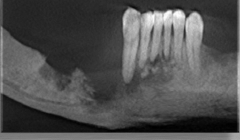
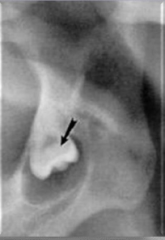
what is this problem? |
staphne bony defect |
|

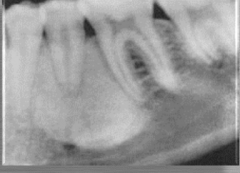
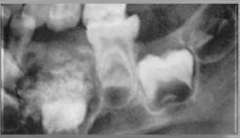
describe lesion |
unilocular radiolucent lesion with corticated borders *you lose cortication a little on the L side of abscess |
|

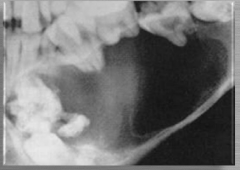
describe lesion |
unilocular radiolucent lesion with corticated borders |
|

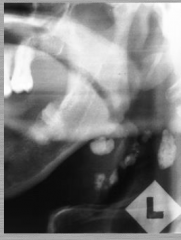
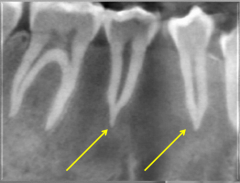
describe lesion |
unilocular r-lucency with non-corticated borders |
|

describe lesion |
unilocular r-lucency with non-corticated borders |
|
describe lesion |
unilocular r-lucency with non-corticated borders *example: periapical abscess
non-corticated = infection spread |
|

describe lesion |
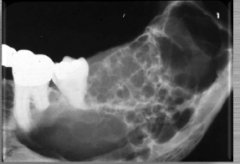
multilocular r-lucent lesions |
|
describe lesion |
multilocular r-lucent lesion *examples: ameloblastoma, KOT |
|
describe lesion |
multilocular r-lucent lesion |
|

describe lesion |
multilocular r-lucency |
|
describe lesion |
multilocular r-lucency |
|

describe lesion |
multi-FOCAL r-lucencies *note they are well-defined, but NOT corticated
(multilocular are usually corticated) |
|
|
Name a time where you have multi-focal r-lucencies |
PA osseous dysplasia (POD) |
|

|
multifocal lesions *florid dysplasia dysplasia (no tx) |
|
|
multifocal -florid dysplasia |
|
|
multifocal -florid dysplasia (lesions coalesce and come together) |
|

|
moth-eaten |
|
|
moth-eaten |
|

|
moth-eaten |
|
|
Examples where you see moth-eaten? |
these have irregular shape/border -osteomyelitis -malignancies -most common: bisphosphonate related |
|

|
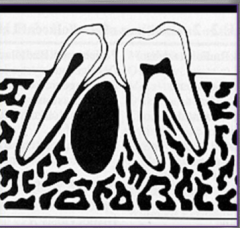
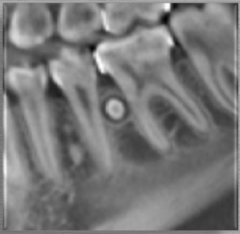
unilocular corticated w/ inter-radicular location |
|
|
unilocular corticated w/ inter-radicular location *see in periodontal cyst |
|

|
unilocular corticated r-lucent lesion in a PERICORONAL location *dentigerous cyst (will push tooth down) |
|
|
unilocular corticated r-lucent lesion with PERICORONAL location -CEJ to CEJ -*dentigerous cyst (will push tooth down) |
|
|
unilocular corticated r-lucent lesion with PERICORONAL location -CEJ to CEJ -*dentigerous cyst (will push tooth down) |
|

|
r-opaque lesion of jaws -will cause tooth to erupt -ex: fibrous dysplasia, DBI (dense bony island)
|
|

|
r-opaque lesion of jaws -will cause tooth to erupt -ex: fibrous dysplasia, DBI (dense bony island) |
|
|
r-opaque lesion terminology: focal opacity |
|

|
r-opaque lesion terminology: focal opacity |
|

|
r-opaque lesion terminology: focal opacity
|
|
|
Where do you see focal opacity? |
eg: DBI (enostosis--meaning inside bone), focal osteosclerosis -no tx |
|

describe lesion |
(r-opacity surrounded by r-lucency) r-opacity: target lesion |
|
describe lesion |
r-opacity: target lesion (r-opacity surrounded by r-lucency) |
|
|
Where do you see target lesions? |
-odontoma -PA osseous dysplasia |
|
describe lesion |
multifocal confluent radiopactiy -florid osseous dysplasia |
|

describe lesion |
irregular and ill-defined r-opacity *be suspicious of osteomyelitis or malignancy |
|
describe lesion |
irregular and ill-defined r-opacity *be suspicious of osteomyelitis or malignancy |
|
describe lesion |
irregular and ill-defined r-opacity *be suspicious of osteomyelitis or malignancy |
|

describe lesion |
ground glass -think fibrous dysplasia*
|
|

describe lesion |
ground glass -think fibrous dysplasia*
|
|

describe lesion |
mixed density -lesion is producing something -sometimes infection, but it's some kind of calcification -if it's multiclocular, there will be septations--that's not mixed density
|
|

describe lesion |
mixed density -lesion is producing something -sometimes infection, but it's some kind of calcification -if it's multiclocular, there will be septations-- that's not mixed density |
|

describe |
mixed density -mostly cystic with flecks of calcification |
|

|
mixed lucent-opaque lesion in PERICORONAL location -AOT/CCOT/Gorlin's cyst |
|

|
mixed-lucent opaque lesion in PERICORONAL location -AOT/CCOT/Gorlin's cyst |
|

|
mixed density lesion in zygoma and maxilla |
|
|
mixed density lesion in zygoma and maxilla |
|
describe |
mixed lucent-opaque in pericoronal -AOT |
|
describe |
mixed -could be odontoma
|
|

|
soft tissue opacity
|
|

|
soft tissue opacity |
|
|
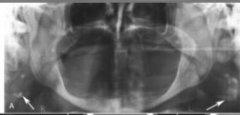
Most common soft tissue opacities? |
-calcified LN -sialoliths -tonsiliths -phleboliths (calcified blood clots) -calcified carotid atheromas |
|
|
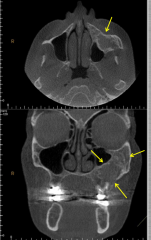
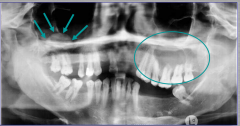
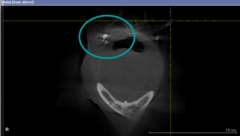
soft tissue opacity arrows = r-opacity, mucus retention cyst aka antral pseudocyst (bc in maxillary antrum) circle = septations in maxillary sinus |
|
|
If infection is coming from the tooth/odontogenic? |
CORTICATED BORDER |
|

|
mucus retention cyst/antral pseudocyst -no corticated border; it's in maxillary sinus |
|

|
mucus retention cyst/antral pseudocyst -no corticated border; it's in maxillary sinus |
|
|
calcified LN |
|

|
calcified LN |
|

|
calcified LN |
|
|
calcified LN |
|
|
calcified LN |
|
|
sialolith |
|
|
sialolith |
|

|
sialolith |
|
|
tonsolith -most common calcification (may be a cause of halitosis as well) |
|
|
phlebolith |
|
|
phlebolith |
|
|
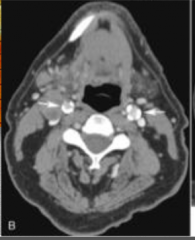
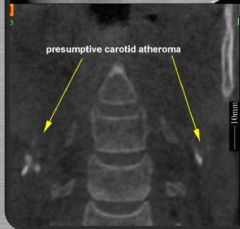
calcified carotid atheroma -from c2 to c5 -calcium deposits in blood vessels exactly at bifurcation of internal and external carotid
*can cause stroke, refer! *SOFT TISSUE WINDOW see tissue/muscles easily (with contrast' use to see anything related to BV because problem gets lighted up) |
|
|
calcified carotid atheroma -from c2 to c5 -calcium deposits in blood vessels exactly at bifurcation of internal and external carotid
|
|

|
calcified carotid atheroma -from c2 to c5 -calcium deposits in blood vessels exactly at bifurcation of internal and external carotid
-soft tissue window |
|
|
ground glass -think fibrous dysplasia*
|
|
|
What will be the shape of calcified carotid atheroma? |
ALWAYS IRREGULAR |
|
|
Rx Signs: Density for benign |
-Rlucent -mixed -septations, loculations |
|
|
bony window, coronal calc. carotid atheroma |
|

|
bony window, axial -calc. carotid atheroma |
|
|
Rx signs: density in malignant |
-ALWAYS RLUCENT **except: mets in breast and prostate cancer and osteogenic sarcoma |
|
|
Rx signs: margins in benign |
-well-defined (narrow zone of transition) -slow growing -smooth, regular -corticated! |
|
|
Rx signs: margins in malignant |
-ill defined (wide zone of transition) -ragged -moth eaten |
|
|
Rx Shape: benign vs malignant |
benign - round/oval malignant - irregular |
|
|
Two things that cause irregular borders? |
1. inflammation 2. malignancy |
|

|
multilocular |
|
|
unilocular |
|
|
Effects on cortical bone benign vs malignant |
benign --> expansion, thinning, aggressive benign may erode
malignant --> erosion, destruction |
|

|
undulated |
|
|
examples of multilocular lesions |
ameloblastoma, KOT, myxoma |
|
|
multilocular/soap bubble |
|

|
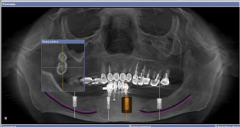
nasopalatine cyst (over 6 mm) |
|
|
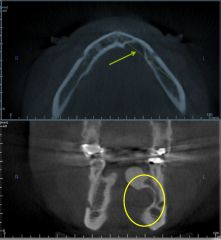
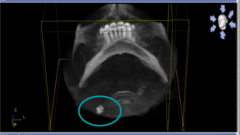
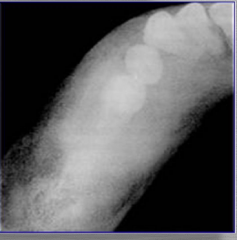
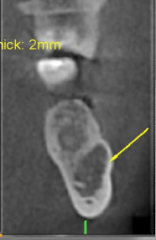
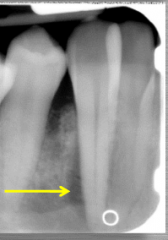
If lesion is below IAN, then it is considered to be... |
NON-ODONTOGENIC in orgin -not dental related origin
eg: staphne bony defect |
|

|
staphne bony defect |
|

What do you see in upper R and middle L? |
Benign effects on cortical bone R = thinning --> charac. of benign L = erosion |
|
|
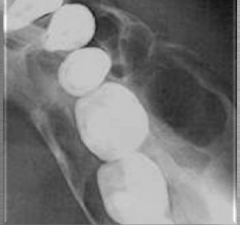
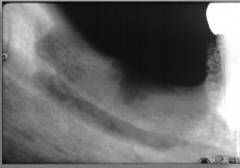
Benign effects on maxillary sinus |
displacement; it will push |
|
|
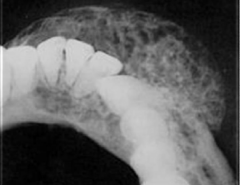
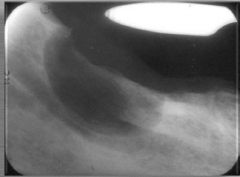
Malignant effects on maxillary sinus? |
Destruction |
|

|
benign effect on mx sinus; just pushing posterior border up |
|

|
malignant effect on mx sinus; soft tissue has grown in and you can't see border of max sinus anymore on one side
-lymphoma |
|
|
Malignant effects on IAN |
invasion and destruction of canal -anesthesia/paresthesia |
|
|
Benign effects on IAN |
-displacement of mn canal -no neuro-sensory deficits |
|
|
malignant; going through the IAN canal -SCCa |
|
|
benign; just pushing down on IAN canal -ameloblastoma |
|
|
Benign tumor and tooth position |
-displacement -may prevent eruption |
|
|
Malignant tumor and tooth position |
-"floating teeth" |
|
|
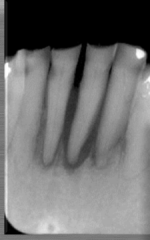
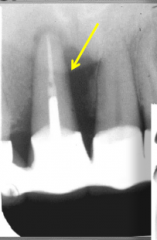
malignant -assym. widening of pdl space
*FIRST AND FOREMOST SIGN OF MALIGNANCY! |
|

|
malignant; floating teeth |
|

|
benign; just displacing teeth (hemangioma) |
|
|
Benign vs malignant tumors and root resorption |
benign - tend to cause root resorption (uniform) (horizontal/near horizontal)
malignant - sometimes none, or sometimes SPIKED (vertical) |
|
|
If see horizontal/diagonal root resorption, it's most likely: |
ameloblastoma |
|
|
malignancy; spiked roots |
|

|
spiked roots; malignancy |
|

|
horizontal resorption; benign |
|

|
benign |
|
|
Assymetrical widening of the pdl suggests? |
MALIGNANCY -osteosarcoma -chondrosarcoma -lymhpoma
*could also be caused by scleroderma, root fracture, ortho mvmt |
|
|
assym. widening of pdl |
|
|
assym. widening of pdl |
|
|
What should you know about lymphoma? |
Bimodal (kids to adults) |
|
|
Scleroderma |
-loss of angle of mn bc masseter muscle |
|

What do you see under 29? |
Ground glass -characteristic of dysplasias |
|

What does this pt have? |
Florid osseous dysplasia -r-opacities |