Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
64 Cards in this Set
- Front
- Back
|
Cytokines released by T-cells leading to further joint inflammation in RA
|
TNF, interleukins
|
|
|
Disadvantage of using NSAIDs
|
Don't alter the disease course
|
|
|
Flector Patch
|

Diclofenac
RA q12h |
|
|
Pennsaid
|

Diclofenac solution
For knees only |
|
|
Lidone (XL)
|
Etodolac
600mg-1200mg/d in bid or qid |
|
|
Indocin (SR)
|
Indomethacin
PO IV Supp 100-200mg/d Can cause more headaches |
|
|
Felafen
|
Nabumetone
NSAID |
|
|
Tolectin
|
Tolmetin
NSAID |
|
|
Clinoril
|
Sulindac
NSAID |
|
|
Ibuprofen
|
Max 3200mg/d in tid-qid
|
|
|
Orudis
|
Ketoprofen
Max 300mg/d in tid-qid |
|
|
Oruvail
|
Ketoprofen SR
100-200mg/d qd |
|
|
Naprosyn
|
Naproxen
500-1500mg/d in bid tid |
|
|
Feldene
|
Piroxicam
10-20mg/d qd bid |
|
|
Celebrex
|
Celecoxib
200-400mg/d qd bid |
|
|
Mobic
|
Meloxicam
|
|
|
If pt is on high dose of NSAIDs think about giving this medication
|
PPI, H2RA, misoprostol
|
|
|
NSAIDS with high ulcer risk
|
Piroxicam
|
|
|
NSAID ADR
|
Ulcers
Hepatic failure Renal blood flow decrease |
|
|
What allergies must Celebrex be avoided in?
|
Sulfa
|
|
|
Advantages of using DMARD
|
Preserve joint integrity and function
|
|
|
Monotherapy for all categories of RA
|
Methotrexate, Leflunomide
|
|
|
Plaquenil
|
Hydroxycloroquine
Decreases interleukin-1 from monocytes 200mg bid |
|
|
Myochrisine
|
Gold sodium thimalate
|
|
|
Minocin
|
Minocycline
|
|
|
MTX sig DDI
|
Bactrim (can cause added hematologic abnormalities)
NSAID and ASA can increase concentration |
|
|
Folic Acid recommended doses for pt on MTX
|
max 3mg/day
|
|
|
All pts on DMARDs should recieve ___ prior to DMARD initiation
|
vaccines
|
|
|
MTX dose
|
7.5-25.0mg po qwk
|
|
|
Avara
|

Pregnancy category X
If wish to get pregnany must follow drug elmination protocol |
|
|
Avara ADR
|
Diarrhea, LFT, alopecia, hypertension and rash.
|
|
|
Avara DDI
|
Increased liver tox when used in conjunction with MTX
|
|
|
Avara elimination protocol
|
8g of Questran tid for 11 days;
plasma levels of M1 > 0.02mg/L verified on 2 occasion 2 weeks apart. |
|
|
Avara dosing
|
100mg qd x3days, 20mg qday
|
|
|
Cuprimine
|
D-penicillamine
Thrombocytopenia Proteinuria Rash Stomatitis |
|
|
Cuprimine administration
|
TAKE ON EMPTY STOMACH
|
|
|
Gold ADR
|
RASH
sun sensitivity Protein/hema-uria Leukopenia |
|
|
anti-TNF therapy for RA
|
Enbrel
Remicade Adalimumab |
|
|
Anti-TNF ADR
|
INFECTIONS (no live vaccines)
Rash Nausea Cough |
|
|
Enbrel
|

|
|
|
Kineret
|
100mg sc qd
|
|
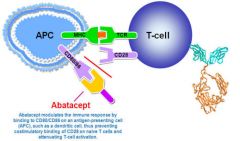
Orencia
|

CI with other DMARDs
CI Live vaccines |
|
Rituxan
|
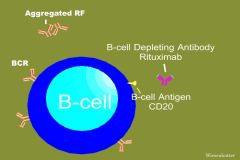
Last line therapy
Pre-medicate with glucocorticoid 1000mg q 2wk |
|

Imuran
|
Azothiaprine
50-150mg/d po qd bid CBC, creatinine, lft DDI with allopurinol |
|
|
|
Hypertension
Nephrotoxicity Glucose intolerance Hepatoxicity |
|

|
Hypertension
Nephrotoxicity Glucose intolerance Hepatoxicity |
|
|
Pt on chronic glucocorticoid should recieve
|
1500mg elemental calcium and 400-800IU of vitamin D/day
|
|
|
Lifestyle modification in RA
|
increase protein intake
|
|
|
DOA for OA
|
APAP
|
|
|
Ultram (ER)
|
400mg/day
Don't take with MAOI Constipation/ n/v, sz, and withdrawal sx |
|
|
Chondroitin and Glucosamine DDI
|
Warfain
May increase risk of bleeding |
|
|
Colchicine for RA dose
|
1.2mg po then 0.6mg 1hr later. Max 1.8mg over 1 hr.
IV PO Dose renally Most effective when given within 12-36 hours of attack |
|
|
Colchicine indication
|
chronic suppressive therapy for gout
|
|
|
Colchicine ADR
|
NVD, bloating.
Bone marrow suppresion Extravasation Don't give in PUD |
|
|
Benemid
|
Probenecid
Blocks uric acid uptake in proximal tubule |
|
|
Benemid counseling
|
Drink plenty of water to prevent stones
Don't use in gouty attack b/c it may exacerbate it. |
|
|
Benemid DDI
|
NTF decreased efficacy
Penicillin increased efficacy May increase [sulfonylurea] |
|
|
During gouty attack what meds to give and which to avoid
|
give: NSAIDs, Colchicine
avoid: probenecid |
|
|
Benemid dose
|
250-500 mg po bid
|
|
|
Zyloprim
|
Allopurinol
300mg po qd Rash |
|
|
Uloric
|
Febuxostat (Zyloprim like agent)
|
|
|
Elitek
|
Rasburicase (don't use in pt with G6PD)
|
|
|
antiphosphoslid antibody (from SLE) increases the risk of ___
|
Stroke
|
|
|
Treatment of SLE
|
Hydroxychloroquine
Glucocorticoid cyclophosphamide NSAIDs |