![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
23 Cards in this Set
- Front
- Back
|
What is the most common treatment of RA? |
Methotrexate +/- NSAID and corticosteroid |
|
|
What is the treatment for MILDER cases of RA? |
Hydroxychloroquine (lower toxicity) |
|
|
If there is initial treatment failure in RA, what is the next approach (first-line biological agents)? |
Etancept Infliximab Adalimumab Golimumab Certolizumab |
|
|
If there is an inadequate response to the TNF-alpha inhibitor, what other non TNF-alpha drugs could be used? |
Anakinra Rituximab Toclizumab |
|
Was there a difference between the two arms? Was there a difference in secondary outcomes, such as radiographic progression, pain, health relate quality of life or adverse outcomes? |
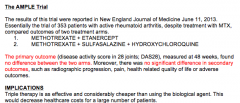
Triple therapy is cheaper and as effective use it! |
|
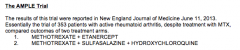
What was the result of this trial? |
Initial MTX therapy with option to step-up to combination therapy results in similar outcomes to immediate combination therapy! |
|
|
What are the four DMARD drugs?
What is the general mechanism? |
Methotrexate Hydroxychloroquine Leflunomide Sulfasalazine
Ability to improve inflammatory symptoms and slow the progression of joint erosions |
|
|
What is the mechanism of methotrexate? |
Inhibition of AICAR transformylase => AICA riboside accumulation -> inhibits adenosine deaminase => increased adenosine concentrations => inhibits lymphocyte proliferation and suppresses IL-1, INF-gamma, and TNF, increases IL-4, impairs release of histamine and decreases neutrophil chemotaxis |
|
|
What is the metabolism and elimination of methotrexate? |
Polyglutatamation = drug retained intracellularly Kidney elimination (caution in renal failure, involves tubular secretion)
Hepatic metabolism (think liver conditions) |
|
|
What are two primary AEs to methotrexate?
is it teratogenic? Should you get a vaccination while on methotrexate? |
Immunosuppression, pulmonary toxicity (interstitial pneumonitis and pulmonary fibrosis)
Yes! No! |
|
|
What parameters should you monitor with methotrexate? |
CBC, LFTs, serum creatinine/BUN, serum uric acid |
|
|
Sulfasalazine: When is it used?
Mechanism of action: LIKE A COMPLICATED NSAID! |
When patients have not responded to salicylates or NSAIDS
Metabolized => sulfapyridine and mesalamine by colon bacteria
Sulfapyridine absorbed and hydroxylated in liver (think about patients with poor acetylation status)
Inhibits PG and LT production |
|
|
How is sulfasalazine eliminated?
Can accumulation occur with repeated dosing? |
Renally (caution with renal dysfunction) => accumulation can occur with repeated dosing |
|
|
What are the contraindications of sulfasalazine? |
Hypersensitivity to 5-aminosalicylate, salicylate, or sulfonamide drugs |
|
|
What is the MAJOR ADVERSE EFFECT of sulfasalazine?
What parameters should you monitor? |
Fatal blood dyscrasias
CBC, LFTs, creat/BUN, urinalysis |
|
|
Leflunomide: What is the mechanism? (cytostatic of cytotoxic) |
Active metabolite A77 1726 => inhibits dihydroorotate dehydrogenase (DHODH), enzyme involved in cell mitochondria that catalyzes key step in de novo pyrimidine synthesis
T and B lymphocyte, immunoglobulan cell progression arrested (cytostatic) |
|
|
What is the elimination of leflunomide? Is hepatoxicity associated with chronic use of the drug? |
Uricosuric effect (feces and urine)
Yes (caution with alcoholics) |
|
|
What patients should not take Leflunomide? (think about its actions...it's an immunosuppressive drug)
Is this Leflunomide a teratogen? |
Severe immunodeficient, bone marrow displasia, or uncontrolled infection
Category X drug |
|
|
Hydroxychloroquine
What is it used for?
Is it fast or slow? |
Malaria prophylaxis (also SLE and RA)
Slow |
|
|
What is the mechanism of hydroxychloroquine? |
Increases intracellular vacuole pH => alters protein degradation
Diminishes formation of peptide-MHC protein complexes required to stimulate CD4+ T cells => down-regulation of immune response against auto antigenic properties |
|
|
How is hydroxychoroquine eliminated? |
Slow renal elimination following hepatic metabolism |
|
|
In what diseases if hydroxychloroquine contraindicated?
What are some AEs? |
Ocular disease (can cause eye problems)
Hepatic disease or alcoholism (concentrates in liver)
Blood dyscrasias
CNS toxicity |
|
|
What should you monitor in patients taking hydroxychloroquine? |
CBCs, opthalmalogic exam |