![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
30 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
What are some risk factors for PE? |
Age >40 Surgery, esp hip, knee, cancer Surgery >30min Trauma Malignancy Chronic disease (CCF, COPD) Thrombophilias Immobilisation Long distance travel Pregnancy Smoking OC and HRT |
|
|
|
What is the highest risk in terms of thrombophilias |
Multiple coexisting defects |
|
|
|
Which thrombophilia is most concerning in terms of PE risk? |
Factor V Leiden homozygotes, heterozygotes may have slightly increased risk. It is a condition of hypercoagulability. It is the most commonest thrombophilia in the community. |
|
|
|
What is the normal background VTE risk for thrombophiliacs? And what age do they usually present? |
1-2 per 1000 Age 50-60 |
|
|
|
Name some inherited thrombophilias |
Rare Abnormalities of antithrombin Protein C and S deficiency Common Factor V Leiden Activated plasma C (APC) resistance Very rare Severe homocysteinuria |
|
|
|
Name some acquired thrombophilias |
Activated phospholipase antibodies
Mild homocysteinuria (common) |
|
|
|
Is the absolute risk of OCs high or low? |
Low |
|
|
|
When are OCs contraindicated? |
In cases of known family hx of Factor v Leiden or other prothrombotic state |
|
|
|
Are 2nd generation OCs lower risk? |
Yes, because of low dose oestrogen release |
|
|
|
Why does pregnancy increase the chance of DVT? |
Multifactorial. There is a clotting predisposition in preparation for placental separation. The placenta itself is a big vascular bed that needs to clot after delivery. Also, expansion of uterus, compression of major vessels, leading to backup pressure in lower limbs. |
|
|
|
What is a DVT? (roughly) |
A thrombus in deep veins of the leg. Can be above or below level of knee A thrombus that extends or originates in iliac veins/iliofemoral circulation |
|
|
|
What investigations can we use to detect DVT? |
Venography (gold standard) 123 I-fibrinogen (good for calf, unreliable for proximal DVT) Compression US (poor in iliac, sup fem v) Duplex B-mode ultrasound (realtime US + Doppler - very good, this is the most often used) Impedance plethysmography (IPG) |
|
|
|
What diagnostic tests can we run? |
Lung perfusion (V/Q scans) CTPA |
|
|
|
What are the clinical features of a PE? |
Dyspnoea Tachypnoea Tachycardia Small peripheral PE with infarct: Pleuritic pain, cough, haemoptysis Massive PE: Syncope Hypotension Cyanosis Right heart dysfunction |
|
|
|
What do we expect to see on FBC? |
High WCC (>20,000 not uncommon) |
|
|
|
What do you expect see on D-dimers? |
Elevated Should be ordered in all cases of suspected PE |
|
|
|
What do you expect to see on ABG? |
Hypoxia and hypocapnia (low pO2 and pCO2) Widened A-a gradient (20mmHg or more) ABG findings are only suggestive/not suggestive of PE and not diagnostic on their own. |
|
|
|
What do you expect to see on CXR? |
Possible atelectasis Elevation of hemidiaphragm Prominent central pulmonary artery (Fleischner sign) Decreased blood at site of embolism (Westermark sign) Findings only suggestive and not diagnostic |
|
|
|
What do you expect to see on ECG? |
Most commonly, sinus tachycardia S1Q3T3 (McGinn-White sign) - Deep S wave in lead 1, Q wave and inverted T wave in lead 3 - but only in 10-20% PE pts - indicates acute cor pulmonale (RV failure due to pulmonary HTN) Other ECG findings include: Tall P waves in lead 2 R axis deviation RBBB Atrial fibrillation These signs all have low sens and spec. |
|
|
|
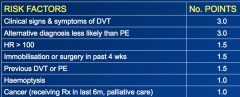
What are the interpretations of the Wells score, and what are the cutoffs? |
Traditional interpretation >6.0 — High 2.0 to 6.0 — Moderate <2.0 — Low Alternative interpretation >4 — PE likely. Consider diagnostic imaging. 4 or less — PE unlikely. Consider D-dimer to rule out PE. |
|
|
|
What are some of the risk factor domains of the Wells score? (Not that critical to know) |
|
|
|
|
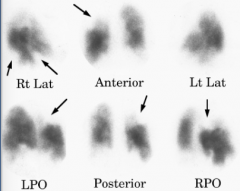
What do you "want" to see in a V/Q scan that is high probable for a PE? (see hint) |
- A lack of perfusion in ventilated areas of lung - Multiple, bilateral, segmental V/Q mismatch |
|
|
|
What do you "want" to see in a CT scan that is high probable for a PE? (see hint) |
Marked filling defect in pulmonary arteries Pulmonary artery obstruction due to a clot |

|
|
|
What clinical signs might you see at the bedside? |
- Calf swelling - Leg oedema - Superficial thrombophlebitis - Homan's sign - leg extended, passive flexion of ankle induces pain at clot location |
|
|
|
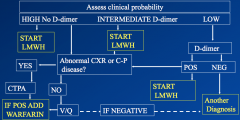
The lecture mentions British Thoracic Society (BTS) guidelines for PE management and diagnosis. Try to describe this if you can. (Diagram on hint side) |
First you assess clinical probability for PE, as high, intermediate, low, using a score such as Wells. Run D-dimer for low and inter, no need in high. For low, if D-dimer is raised, start LMWH and go for CXR, if not, consider another diagnosis. For inter, start LMWH regardless of D-dimer, then CXR. For high, don't do D-dimer, start LMWH. You can get a CXR if indicated. For CXR, if abnormal, do CTPA, if not, do V/Q scan. If either positive, add warfarin. If negative, other diagnosis. |
|
|
|
What is the mainstay of treatment for PE? Which agents would you use? What are the pertinent points regarding their use? |
Anticoagulant therapy. LMWH is preferable to UFH (RR reduction 40% accr to Cochrane) Warfarin needs frequent dose adjustment and monitoring of INR. If more episodes of PE occur while warfarinised, INR window usually increased (e.g. 2-5-3.5) Warfarin is teratogenic. For pregnany women, use LMWH until at least 6w post delivery. Warfarin is usually continued for 3-6m and can be lifelong. This is usually determined by D-dimer levels at end of treatment, esp in pts with a first episode PE. |
|
|
|
What INRs are ideal in PE? |
Between 2.0 and 3.0 |
|
|
|
Other than anticoagulation, what other treatment options are there? What are the indications? |
Thrombolysis Indication: Massive PE (shock/hypotension, SBP<90, or pressure drop >40 for >15min, not of cardiac/volaemic/septic cause) IVC filter Indication: if anticoagulants are contraindicated (e.g. post major op) Prevents new emboli from entering pulm art. Remove as soon as safe to anticoagulate. Surgery such as pulmonary thrombectomy is now uncommon and abandoned. |
|
|
|
What options are there for DVT/VTE prophylaxis? |
TEDs. NO BED REST! Exercise as tolerated. Intermittent pneumatic compression Hydration |
|
|
|
What is the summary evidence given in the lecture for anticoagulation, LMWH prophylaxis and aspirin & TEDs? |
Anticoagulation: Warfarin for 6m after first PE reduced VTE LMWH prophylaxis: Reduces VTE in major orthopaedic surgeries Aspirin and TEDs: As prophylaxis, reduced VTE in orthopaedic surgery TEDs reduced DVT in long haul travel |
|