![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
121 Cards in this Set
- Front
- Back
|
What is pneumonia? |
Acute resp. illness with radiological pulm. shadowing (segmental / lobar / multilobar) |
|
|
Pneumonia can be divided into? |
1. community acquired pneumonia (CAP) 2. hospital acquired pneumonia (HAP) / nosocomial pneumonia 3. atypical pneumonia |
|
|
CAP typically caused by? |
Strep. pneumoniae |
|
|
Other causes of CAP? |
- H. influenza (rare) - S. aureus - G- rods * E. coli * Pseudomonas * Klebsiella |
|
|
Differences between CAP & nosocomial pneumonia? |
1. CAP - NO contact with medical place 2. HAP - at least 2 days after admission |
|
|
Patients with CAP may come with these symptoms? |
- fever - rigors / chills - productive cough - mucopurulent sputum - pleuritic chest pain - dyspnea - vomit / LOA - headache |
|
|
Pleuritic chest pain is? |
Pain that may occur on shoulder / anterior abdomen |
|
|
On examinations, what can we obtain from the patients? |
- fever / tachypnea / tachycardia - PE * crackles * increase fremitus * dull percussion * bronchial breathing |
|
|
How can we diagnose CAP? |
1. CXR - lobar consolidation 2. Sputum G stain + culture 3. CURB-65 4. PE |
|
|
What is CURB-65? |
To decide pt. admission C - confusion U - urea > 7mmol/L R - RR > 30/min B - BP <90 sBP, <60 dBP 65 - age >65y.o. |
|
|
What can we decide from CURB-65? |
1. if 1<, - can be treated at home 2. if 2, - treated at hospital 3. if >3 - treated at hospital as severe pneumonia |
|
|
How can we manage CAP? |
1. O2 - to make sure; - PaO2 >8kPa - SaO2 >92% 2. Fluid balance - give IV fluid if dehydration / shock 3. ATB tx - if uncomplicated = amoxicillin - if allergic to PNC = clarithromycin, erythromycin 4. Tx pleural pain - paracetamol - NSAIDs - opiates |
|
|
Complications of CAP? |
- pleural effusions - pleural empyema - acute resp. failure |
|
|
What can we do for pleural effusions as complication of CAP? |
1. Usually resolve as pneumonia is treated with ATB 2. If larger, may need pleural tap (culture of fluid as well) |
|
|
Predisposing factor of CAP? |
- smoking - URTI - alcohol - CS therapy - old age - pre-existing lung dis. |
|
|
Most common pathogens of HAP (nosocomial pneumonia)? |
- G- rods * Klebsiella * E. coli * Enterobacter * Pseudomonas - S. aureus (MRSA) |
|
|
Clinical presentations of HAP? |
- similar to CAP - but may be complicated with comorbidities & drug-resistant |
|
|
Predisposing factors of HAP? |
- reduce host defence against bacteria - aspiration of nasopharyngeal / gastric secretion - bacteria to LRT - bacteremia |
|
|
What may differentiate CAP & HAP (other than contact with medical place)? |
HAP - worsening oxygenation - increase tracheal secretion - new radiology infiltration (than CXR on admission) |
|
|
How can we treat HAP? |
1. if NOT MRSA? - ceftriaxone - ciprofloxacin - ampicillin 2. if YES MRSA? - IV vancomycin - cefepime - ciprofloxacin / levofloxacin - gentamicin |
|
|
How about atypical pneumonia - it can be caused by? |
- typically Mycoplasma pneumoniae - can also be: * Chlamydia pneumonia * Legionella |
|
|
Clinical presentations of atypical pneumonia - that may differentiate it with other pneumonia? |
Presence of: - headache - pharyngitis - fatigue (flu-like sx.) |
|
|
What is COPD? |
Chronic obstructive pulmonary disease (or COAD - chronic obstructive airway disease) |
|
|
Characteristics of COPD? - COPD is combination of? |
- chronic bronchitis - emphysema ** usually coexist! |
|
|
What can be seen roughly in patients with chronic bronchitis? |
- chronic productive cough - for at least 3months/year - for at least 2 consecutive years |
|
|
What happens in emphysema? |
Permanent enlargement of air spaces distal to terminal bronchioles - due to destruction of alveolar walls |
|
|
What can trigger COPD? |
- smoking (tobacco) - alpha 1 antitrypsin deficiency - environmental pollutants |
|
|
How to differentiate etiology of COPD and types of emphysema? |

1. Smoking - 90% of cases - centrilobular emphysema 2. Alpha 1 antitrypsin deficiency - panlobular emphysema |
|
|
General pathophysiology of chronic bronchitis What happens in chronic bronchitis? |
Airways inflamed →hypertrophy of mucous gl. & smooth m. → excess mucous production → airways obstruction |
|
|
General pathophysiology of emphysema What happens in emphysema? |
Smoking irritates lungs → activate neutrophils, macrophages → release elastase → destruct alveolar walls |
|
|
Functions of alpha 1 antitrypsin? |
INHIBITS destruction of walls by elastase & free radicals |
|
|
Patients with COPD may come with? COMBINATION of manifestations of emphysema & chr. bronchitis |
EMPHYSEMA - dyspnea on exertion** / rest - tachypnea - barrel chest ('stuck' in inspiration phase) CHR. BRONCHITIS - cyanosis - due to respiratory insufficiency - chronic productive cough** - expiratory wheezing |
|
|
How to diagnose COPD? |
1. Pulm. Fx Test (spirometry) - ↓ FEV1 (means obstructive pathways) - ↑ TLC, RV (lots of air remained in lungs) - ↓ VC vital capacity (less air in & out) 2. CXR - hyperinflation - flattened diaphragm |
|
|
What need to add into diagnostic approach for children with sign of COPD? |
Alpha 1 antitrypsin deficiency - may need measurement |
|
|
How to manage COPD? (medications) |
1. Inhaled B2 agonist - albuterol, salmeterol - as bronchodilator ** in MYS - seretide accuhaler 2. Inhaled anti-cholinergic drugs - ipratropium bromide (muscarinic) ** in MYS - Spiriva 3. Mucolytic agents - to relieve mucous secretion - theophylline (↑ mucociliary clearance) ** in MYS - Bisolvon |
|
|
Drugs used for COPD in MYS? |
1. Neb Combivent (albuterol + ipra. bromide) 2. Bisolvon (mucolytic agent) |
|
|
What can we ask the COPD to change about lifestyle? |
- STOP smoking |
|
|
When to use O2 therapy in COPD patients? |
In pt. with advanced disease & hypoxemia - to improve life quality & survival |
|
|
If COPD is not well treated, it can lead to? (complications) |
1. Pulm. HTN & cor pulmonale - ↑ pulm. resistance → affect RV → RVF 2. 2° polycythemia - ↑ Ht, Hb, RBC 3. Acute exacerbation (AECOPD) |
|
|
What is acute exacerbation of COPD? (AECOPD) |
COPD pt. have LOW resp. reserve - we need to aware that small problem can lead to resp. failure - eg:- pulm. infection (pneumonia) |
|
|
How to manage AECOPD? |
1. Bronchodilators / systemic CS - hydrocortisone - prednisolone ** to ↓ immunity for chr. bronchitis 2. Broad spectrum ATB - IV unasyn (ampicillin + sulbactam) - azithromycin ** to treat bronchitis 3. O2 supply - for long standing hypoxia - to keep SaO2 >90% - if critical, may need CPAP / intubation 4. Monitor ABG - PaO2 > 8kPa - paCO2 < 6kPa |
|
|
What is asthma bronchiale? ** BA |
Chronic inflammation of airways - assoc. with airway hyper-responsiveness ** known as BA (bronchial asthma) |
|
|
Patients with bronchial asthma may come with? |
Recurrent episodes of: - wheezing - dyspnea - chest tightness - coughing |
|
|
What causes bronchial asthma? |
- allergens (outdoor / indoor) - air pollution - resp. tract infection |
|
|
What happens in BA? (pathophysiology) |
Narrowing of airways - how? - constriction of bronchial m. - edema of bronchial mucosa - mucous hypersecretion & plug formation ** eventually airway wall re-modelling (irreversible!) |
|
|
Patients with BA may complain? |
1. Episodic dyspnea & wheezing (not progressive) - but worsen at night 2. Coughing during asthma attack 3. SOB on exertion 4. Chest tightness |
|
|
What makes difficult to diagnose pt. with BA? |
Clinical signs may appear ONLY during attacks - PE is NORMAL between attacks |
|
|
How can we diagnose BA? |
1. Clinical signs 2. Spirometry (but bronchial obstruction may absent) 3. Broncho-provocation test - give histamine / metacholine to pt. - may evoke asthmatic pathogenesis - then, measure FEV1 (>20% ↓ is +ve) |
|
|
How to differentiate obstructive & restrictive problems from FEV1? |
1. If FEV1 ↓ - obstruction * air cannot escape the lungs 2. If FEV1 = FVC - restrictive * fibrosis / lung pathology (↓ compliance to inspire / expire) |
|
|
How to differentiate COPD & BA? |
COPD - neutrophils (CD8) - onset > 40 y.o. - smoking BA - eosinophils (CD4) - onset < 20 y.o. - atopy |
|
|
Why do we need to treat BA? |
- to control symptoms - to ↓ exacerbations - to ↓ SE |
|
|
How can we manage BA? * depends on severity |
1. Inhaled bronchodilator (SABA) 2. Low dose inhaled CS (ICS) 3. Low dose ICS + LABA 4. Medium / high dose ICS + LABA 5. Systemic CS |
|
|
Functions of medications in BA? - Beta agonist - CS |
Beta agonist - bronchodilator CS - to reduce inflammation |
|
|
Dyspnea is also known as? * define |
Shortness of breath (SOB) - unpleasant breathing - worsened with exercise |
|
|
SOB can be caused by? |
1. Heart disease 2. Airway obstruction 3. Diffuse parenchymal lung disease 4. Pulmonary embolism 5. Disease of chest wall / resp. muscles |
|
|
How dyspnea / SOB may occur? |
- due to ↑ pulm. capillary pressure - can also be due to fatigue of resp. m. - ↓ vital capacity & lung compliance - ↑ airway resistance |
|
|
How is appearance of SOB in heart disease? |
1. Exertional breathlessness → orthopnea → PND + dyspnea at rest 2. Need to check heart diseases |
|
|
Symptoms that may appear with dyspnea in heart disease? |
- hx of MI (ECG changes) - presence of S3 / S4 - murmurs - cardiomegaly - JV distention - hepatomegaly - peripheral edema |
|
|
How to diagnose heart diseases with dyspnea? |
1. Clinical signs - symptoms WORSEN gradually 2. ECG - to check conduction in heart 3. ECHO - to check ventricular fx |
|
|
In which parts of airways may be obstructed in pt. with dyspnea (WITHOUT heart symptoms)? |
ANYWHERE - from extrathoracic airways - to lung periphery |
|
|
How to differentiate acute vs chronic dyspnea (with airway obstruction)? |
ACUTE - difficulty inhaling (URT obstruction) - intermittent with expiratory wheezing (asthma) CHRONIC - slowly progressive exertional dyspnea (emphysema, CHF) - chronic cough with sputum (chr. bronchitis & bronchiectasis) |
|
|
How to differentiate upper tract obstruction and asthma? |
Upper tract obstruction - difficulty inhaling Asthma - intermittent with expiratory wheezing |
|
|
How to diagnose dyspnea with pulm. embolism? |
Sudden SOB with chest pain - tachypnea - inspiratory rales - may check D-dimers |
|
|
Examples of diseases of chest wall & resp. m. than can cause dyspnea? |
- kyphoscoliosis - bilateral diaphragmatic palsy |
|
|
Diagnostic approaches of dyspnea? - with suspection of... |
1. General appearance - can speak in complete sentences - use of accessory m. 2. Vital signs (VS) - RR - O2 3. Chest exam - wheeze, rales - ↓ breath sounds - barrel chest - CXR 4. Heart exam - ECG - JVP - murmurs 5. Limbs - edema, cyanosis |
|
|
What need to be noted on CXR with pt. with dyspnea? |
- cardiac size (cardiomegaly) - evidence of CHF - pneumonia - intersititial / diffuse parenchymal lung dis. - pleural effusions |
|
|
What is orthopnea? |
Dyspnea when lying flat - need more pillows / sit on chair |
|
|
How to differentiate cardiac dyspnea VS pulmonary dyspnea? |
HEART - less gradual onset - nocturnal exacerbation - dyspnea on exertion - ↑ BNP - ↓ LV ejection fraction at rest/exertion LUNG - more gradual onset - nocturnal exacerbation - normal BNP - ↓ FEV1, FEV1/FVC, TLC - dyspnea on exertion |
|
|
What is pleural effusion? |
Excess fluid accumulated in pleural space |
|
|
What is normal value of pleural fluid? ** anatomy? ** composition? |
10-20ml of pleural fluid - similar composition with plasma (but ↓ protein, <1.5g/dL) |
|
|
How pleural fluid may accumulate more than normal? |
- ↑ formation of pleural fluid - ↓ fluid removal by pleural lymphatics ** in 25% cases - unknown causes (maybe viral etiology) |
|
|
How to classify pleural effusions? |
EXUDATES - resemble plasma TRANSUDATES - effusions with normal pleura - ultrafiltrates of plasma |
|
|
Symptoms of pleural effusions? |
May be ASYMPTOMATIC But, if symptomatic: - pleuritic chest pain - dry, nonproductive cough - dyspnea - orthopnea |
|
|
On physical exams, pleural effusions may appear as? |
- ↓ chest expansion at affected side - flat percussion - ↓ vesicular breathing - presence of rubs - ↓ fremitus |
|
|
How to diagnose pleural effusions? |
- PEx - CXR - pleural tap - pleural fluid analysis |
|
|
How CXR of pleural effusions look like? |
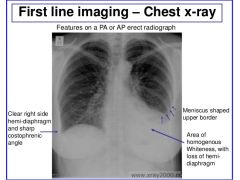
- loss of sharp costophrenic angle - loss of hemidiaphragm |
|
|
Functions of pleural fluid analysis? |
- to check if pleural effusions are exudates OR transudates - to see etiology is due to pleural disease OR others |
|
|
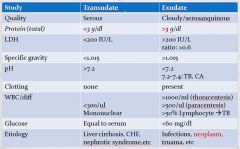
Criteria of exudates? |
At least one of these: - high total fluid / serum protein ratio (>0.5) - pleural fluid LDH >2/3 of normal - pleural / serum LDH ratio (>0.6) |
|
|
Mechanism of formation of exudates & transudates? |
EXUDATES - exudation of fluid, protein, cells, others TRANSUDATES - ↑ hydrostatic pressure - ↓ plasma oncotic pressure |
|
|
Which of exudates & transudates usually occur unilateral / bilateral? |
Exudates - unilateral Transudates - bilateral |
|
|
How to differentiate exudates & transudates based on lab test? |
Check: - RBC - pH - glucose - amylase - specific protein |
|
|
Etiology of transudates? |
Transudates - congestive HF (most common) - liver cirrhosis (with ascites) - nephrotic sy. (hypoalbuminemia) - pulm. embolism - SVC obstruction - peritoneal dialysis |
|
|
Etiology of exudates? |
Exudates - pneumonia - cancer / malignancy - pulm. embolism - viral inf. - TB (pleuritis) - rheumatoid arthritis - chylothorax / hemothorax |
|
|
In pneumonia, when tube thoracostomy with drainage of all fluid is indicated? |
- G+ stained - presence of gross pus - ↓ pleural fluid glucose |
|
|
Why ↓ pleural fluid glucose in exudates? |
Inflammation - glucose is taken by bacteria |
|
|
Which cancers can cause pleural effusions (exudates)? |
- lung cancer - breast cancer - lymphoma |
|
|
In pulmonary embolism, effusions can be? |
Either exudates or transudates |
|
|
What can be seen in effusion of TB pleuritis? |
Exudates - predominant lymphycytosis |
|
|
How to confirm TB pleuritis? |
- PCR for TB - Mycobacterium TB (MTB) culture from fluid |
|
|
How chylothorax may cause pleural effusions? |
Due to trauma to thoracic duct / mediastinal tumor - lymphomatous damage - SVC syndrome |
|
|
How hemothorax may occur? |
- trauma - malignancy |
|
|
Other signs of malignancy related to pleural effusions? |
- cachexia - clubbing - lymphadenopathy - radiation marks - mastectomy scars |
|
|
How to manage pleural effusions? |
Depends on underlying causes 1. Drainage 2. Pleurodesis |
|
|
How to remove / drainage pleural effusions? |
- best removed slowly (<2L/24h) - insertion of chest drain * safe triangle * 4th-6th ICS, ant. to mid axillary line |
|
|
What is pleurodesis? |
- with TTC, bleomycin, talc - for recurrent pleural effusions |
|
|
Which management is good for: - malignant effusions? - empyema? |
Malignant effusions - thoracoscopic talc pleurodesis Empyema - drainage with chest drain |
|
|
Which diagnostic markers may show empyema / TB in pleural effusions? |
- glucose < 3.3mmol/L - pH < 7.2 - LDH ↑ |
|
|
Which diagnostic markers may show rheumatoid arthritis in pleural effusions? |
- glucose < 3.3mmol/L - pH < 7.2 - LDH ↑ - rheumatoid factors - ↓ complement levels |
|
|
Which diagnostic markers may show SLE in pleural effusions? |
- glucose < 3.3mmol/L - pH < 7.2 - LDH ↑ - antinuclear Ab - ↓ complement levels |
|
|
What is pneumothorax? (PNTX) |
Free air in pleural space |
|
|
Pneumothorax can be classified into? |
1. Traumatic PNTX 2. Spontaneous PNTX - primary - secondary |
|
|
1° spontaneous PNTX may occur in which patients? |
- pt. w/out any u/l lung disease - tall, lean young men |
|
|
What causes 1° spontaneous PNTX? |
Spontaneous rupture of subpleural blebs at apex of lungs → air from lung escape into pleural space → lung collapse |
|
|
Why there is NO respiratory distress in1° spontaneous PNTX? |
There is sufficient respiratory reserve |
|
|
Can 1° spontaneous PNTX reoccur? |
Yes - 50% in 2 years |
|
|
2° spontaneous PNTX occur due to? |
- COPD - interstitial lung dis. - CF - TB |
|
|
Why 2° spontaneous PNTX may be potentially life-threatening? |
Due to lack of respiratory reserve - may lead to resp. distress |
|
|
Clinical signs of spontaneous PNTX? |
Usually ASYMPTOMATIC But, if symptomatic; - dyspnea - pleuritic chest pain (ipsilateral) * usually sudden onset |
|
|
How to diagnose spontaneous PNTX? |
1. PEx (on affected side) - ↓ chest expansion - ↓ breath sound - hyperresonance percussion 2. CXR - to confirm dx. - in tension PNTX = mediastinal shifted away from PNTX |
|
|
Difference between spontaneous VS tension PNTX? |
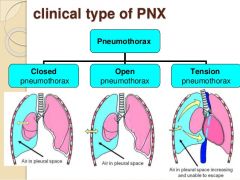
SPONTANEOUS - no mediastinal shift - means air is not accumulated in pleural space TENSION - air accumulated and cannot escape from pleura |
|
|
What causes tension PNTX? |
- barotrauma 2° to mechanical ventilation (changes in air pressure) - CPR - chest trauma |
|
|
How tension PNTX occur? |
Injury to pleural layer: →causes entry to pleural cavity as one-way valve → it allows air to enter BUT not to leave cavity →air accumulated under +ve pressure in cavity →ipsilateral lung collapse → mediastinal shift to healthy side |
|
|
How tension PNTX manifestations may different than spontaneous PNTX? |
In tension PNTX, pt. may have: - hypotension, tachycardia - JV distension - resp. distress On chest exam: - ↓ breath sound - hyperresonance percussion over PNTX side |
|
|
Do we need CXR of pt. with tension PNTX? |
NO! - tension PNTX needs IMMEDIATE relief! * make use of clinical signs of tension PNTX? |
|
|
Why tension PNTX need immediate relief? |
Air accumulated in pleural space cannot leave the cavity - mediastinum is pushed to opposite hemithorax → kinking & compressing great veins - if air is not removed, may cause cardioresp. arrest |
|
|
How to diagnose tension PNTX? |
Same as in spontaneous PNTX 1. PEx (on affected side) - ↓ chest expansion - ↓ breath sound - hyperresonance percussion 2. CXR - to confirm dx. - mediastinal shifted away from PNTX |
|
|
How to manage 1° spontaneous PNTX? |
Check if pt. SOB & rim of air > 2cm on CXR - if no, consider discharge - if yes, try aspiration - consider aspiration 2x before proceed with chest drain - if aspiration success, may discharge pt. |
|
|
How to manage 2° spontaneous PNTX? |
Check if pt. SOB, age > 50 & rim of air > 2cm on CXR - if no, try aspiration → if success, admit for 24h - if yes, proceed with chest drain |
|
|
How to remove air in tension PNTX? |
1. Insert large-bore needle with syringe - partially filled with 0.9% saline into 2nd ICS in midclavicular line of affected side 2. Remove plunger - allow trapped air to bubble through syringe (with saline as water seal) 3. Then, insert chest drainage tube |
|
|
Why management of PNTX is done during; - expiration - Valsalva manoeuvre? |
To make sure high pressure in thorax outwards(?) |
|
|
What should we do in case of persistent air leak? |
1. Ask specialist advice 2. May need suction (high volume, low pressure systems) ** -10 to -20cmH2O 3. Or surgical intervention |