Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
103 Cards in this Set
- Front
- Back
|
What is the most infectious disease in the world?
|
Anxiety
- Survival instinct |
|
|
What are the physiological effects of anxiety?
|
- Fear
- Breathlessness - Choking sensation - Palpations of the heart - Restlessness - Increased muscular tension |
|
|
Which parts of the brain mediates anxiety?
|
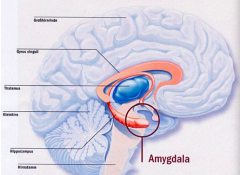
Amygdala - when it senses something is awry or that you should pay attention to a stimuli it starts to fire (gets more blood flow)
|
|
|
What is the fear of dogs?
|
Cynophobia
|
|
|
What is the fear of needles?
|
Aichmophobia
|
|
|
What is the fear of speaking in public?
|
Social Phobia / Anxiety
|
|
|
What is the fear of dead things?
|
Necrophobia
|
|
|
What is the fear of clowns and dolls?
|
- Clowns: Coulrophobia
- Dolls: Pediophobia |
|
|
What is the fear of heights?
|
Acrophobia
|
|
|
What is the fear of flying?
|
Aviophobia or Aviatophobia
|
|
|
What is the fear of germs?
|
Misophobia or Mysophobia
|
|
|
What is the fear of closed or open spaces?
|
- Closed spaces: Claustrophobia
- Open spaces: Agoraphobia |
|
|
What is the fear of spiders / snakes?
|
- Spiders: Arachnophobia
- Snakes: Ophidiophobia |
|
|
When is a fear considered an anxiety disorder?
|
When the fear rules and disrupts life
|
|
|
What are the types of anxiety disorders?
|
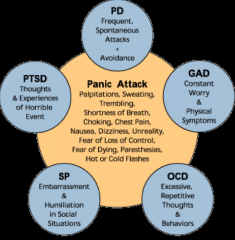
- PD: Panic Disorder
- GAD: Generalized Anxiety Disorder - OCD: Obsessive-Compulsive Disorder - SP: Social Phobia - PTSD: Post-Traumatic Stress Disorder |
|
|
What are characteristics of Panic Disorder (PD)?
|
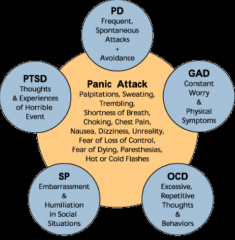
- Frequent spontaneous attacks
- Avoidance of situations |
|
|
What are characteristics of General Anxiety Disorder (GAD)?
|
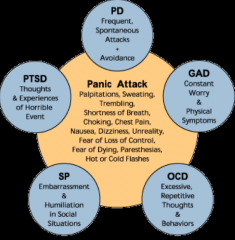
- Constant worry
- Physical symptoms |
|
|
What are characteristics of Obsessive-Compulsive Disorder?
|
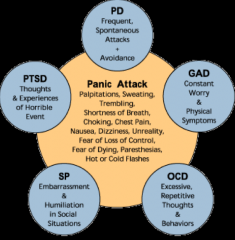
Excessive repetitive thoughts and behaviors
|
|
|
What are characteristics of Social Phobia?
|
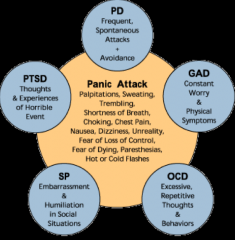
- Embarrassment
- Humiliation in social situations |
|
|
What are characteristics of Post Traumatic Stress Disorder (PTSD)?
|
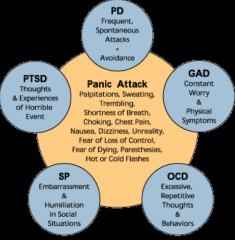
Thoughts and experiences of horrible event
|
|
|
What are the symptoms of a panic attack? What are they a feature of?
|
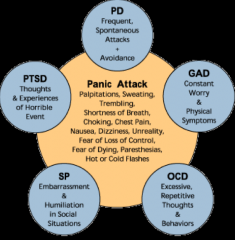
Everything is firing at once (these can occur in any anxiety disorder)
- Palpitations - Sweating - Trembling - Shortness of breath - Choking - Chest pain - Nausea, Dizziness, Unreality - Fear of loss of control - Fear of dying, paresthesias - Hot or cold flashes |
|
|
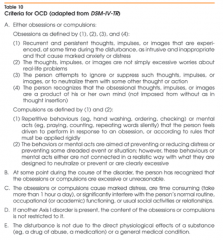
What are the criteria for Generalized Anxiety Disorder (GAD)?
|
- Excessive anxiety & worry (apprehensive expectation), occurs more days than not for >6 months, about a number of events or activities (such as work or school performance)
- Difficult to control worry - Anxiety and worry are associated with ≥ 3 of 6 symptoms: a) restlessness or feeling keyed up or on edge b) being easily fatigued c) difficulty concentrating or mind goes blank d) irritability e) muscle tension f) sleep disturbance - Focus of anxiety and worry not confined to features of an Axis I disorder - Anxiety, worry, or physical sx cause clinically significant distress or impairment in social, occupational, or other important areas - Disturbance is not d/t direct physiological effects of a substance or a general medical condition and does not occur exclusively during a mood disorder, psychotic disorder, or pervasive developmental disorder |
|
|
Generalized Anxiety Disorder (GAD) must have how many symptoms for past 6 months (more days than not)?
|
3+ of the following:
a) restlessness or feeling keyed up or on edge b) being easily fatigued c) difficulty concentrating or mind goes blank d) irritability e) muscle tension f) sleep disturbance |
|
|
What are the criteria for Obsessive Compulsive Disorder (OCD)?
|
- Either obsessions or compulsions (O/C) - see criteria
- At some point during the course of the disorder, person has recognized that the O/C are excessive or unreasonable - O/C cause marked distress, are time consuming (>1 hour/day), or significantly interfere with person's normal routine, occupational or academic functioning, or usual social activities - If another Axis I disorder is present, the content of O/C is not restricted to it - Disturbance is not d/t direct physiological effects of a substance or general medical condition |
|
|
What are the characteristics of Obsessions (that meet criteria for OCD)?
|
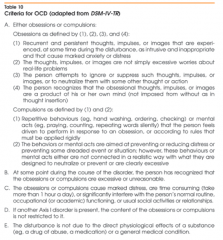
Obsessions:
a) recurrent and persistent thoughts, impulses, or images that are experienced, at some time during the disturbance, as intrusive and inappropriate and that cause marked anxiety or distress b) thoughts, impulses, or images not simply excessive worries about real-life problems c) person attempts to ignore or suppress such thoughts, impulses, or images, or to neutralize them with some other thought or action d) person recognizes that the obsessional thoughts, impulses, or images are a product of his or her own mind (not imposed from without as in thought insertion) |
|
|
What are the characteristics of Compulsions (that meet criteria for OCD)?
|
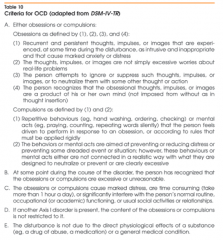
Compulsions:
a) repetitive behaviors or mental acts that the person feels driven to perform in response to an obsession, or according to rules that must be applied rigidly b) behaviors or mental acts are aimed at preventing or reducing distress or preventing some dreaded event or situation; however these behaviors or mental acts either are not connected in a realistic way with what they are designed to neutralize or prevent or are clearly excessive |
|
|
What disorder can cause OCD like symptoms in a child who is sick?
|
PANDAS: Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections
- Rapid onset of obsessive-compulsive disorder (OCD) and/or tic disorders - These symptoms are caused by group A beta-hemolytic streptococcal (GABHS) infections |
|
|
What psychiatric disorder should you consider in a patient you suspect has OCD?
|
Schizophrenia
|
|
|
What developmental disorders should you consider in a patient you suspect has OCD?
|
Autism spectrum disorders (they can have many O/C traits)
|
|
|
What are the criteria for Social Anxiety Disorder?
|
- Marked and persistent fear of ≥1 social or performance situations (unfamiliar people or possible scrutiny by others); fears they will act in a way (or show anxiety sx) that will be humiliating/embarrassing
- Exposure to situation invariable provokes anxiety, may be situationally bound or predisposed panic attack - Recognition of fear being excessive or unreasonable - Avoids feared social or performance situations or endures them with intense anxiety or distress - Avoidance, anxious anticipation, or distress in feared social or performance situation(s) interferes w/ normal routine, functioning, or social activities / relationships (or marked distress about having phobia) - Fear of avoidance is not d/t direct physiological effects of a substance or a general medical condition and is not better accounted for by another mental disorder |
|
|
How can you treat anxiety disorders?
|

Socialpsychobio Model:
- Social treatments - Psychological treatment (diaphragmatic breathing and guided imagery) - Pharmacological therapy |
|
|
What are the anxiolytics to know?
|
- Alprazolam
- Buspirone - Clonazepam - Chlordizepoxide - Diazepam - Flumazenil - Lorazepam |
|
|
What are the muscle relaxants to know?
|
- Baclofen
- Tizanidine |
|
|
What are the hypnotics to know?
|
- Chloral hydrate
- Eszopiclone - Flurazepam - Pentobarbital - Remelteon - Traizolam - Zaleplon - Zolpidem |
|
|
How common are anxiety disorders in lifetime? in 1 year? Severe in 1 year?
|
- Lifetime prevalence: 29%
- 12-month prevalence: 18% - 12-month prevalence of severe: 4% |
|
|
Which age groups have more anxiety disorders?
|
- 18-29: 30%
- 30-44: 35% - 45-59: 31% - >60: 15% |
|
|
How do you characterize Generalized Anxiety Disorder?
|
• Generalized persistent anxiety for > 1 months duration
• Absence of the specific symptoms and patterns that characterize other anxiety disorders such as phobias, panic attacks or obsessive-compulsive disorder • Psychological correlates include apprehensive expectation with worry fear and anticipation of misfortune to self and others, hyperattentiveness, distractibility, difficulty in concentrating, insomnia, feeling on edge and impatience |
|
|
What are the somatic correlates of anxiety?
|
ANS arousal:
- Sweating - Tachycardia - Palpitations - Cold clammy hands - Dry mouth and lump in throat - GI upset - Frequent urination and diarrhea Voluntary muscle activation: - Jitteriness and an inability to relax |
|
|
What are the potential complications of anxiety?
|
Abuse of:
- Alcohol - Sedatives - Anti-anxiety medications |
|
|
Which NT is involved in slow-wave sleep?
|
Serotonin
|
|
|
Which NT is involved in REM sleep?
|
Norepinephrine
|
|
|
What is insomnia?
|
Disorder of initiating and maintaing sleep
|
|
|
What is hypersomnia?
|
Disorders of excessive sleep or sleepiness
|
|
|
The benzodiazepine receptor is associated with a receptor complex for which neurotransmitter?
a) Acetylcholine b) Dopamine c) GABA d) Glutamate e) Serotonin |
GABA
|
|
|
How is GABA synthesized? From what?
|

Glutamate → GABA
by GAD (Glutamic Acid Decarboxylase) |
|
|
What is the primary excitatory NT? inhibitory NT?
|
- Excitatory: Glutamate
- Inhibitory: GABA (interesting because GABA is made form Glutamate) |
|
|
How is GABA metabolized?
|

GABA Transaminase enzyme catalyzes the conversion of into Succinic Semialdehyde (SSA) and glutamate
|
|
|
Where is GABA localized in the brain?
|
- Substantia nigra
- Globus pallidus - Hippocampus - Limbic structures: amygdala - Hypothalamus - Spinal cord |
|
|
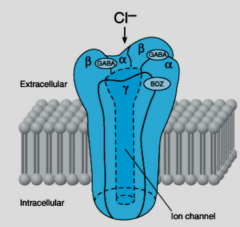
How does GABA mediate its effects?
|
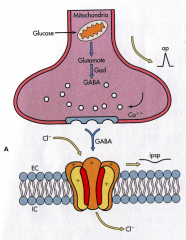
- Released from neuron
- Binds to GABA/Benzodiazepine receptor - Cl- flows through channel which hyperpolarizes the cell (inhibition) |
|
|
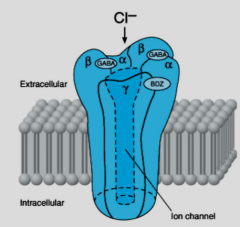
What receptor does GABA bind to? Structure?
|

GABA/Benzodiazepine Receptor
- 5 similar (but not identical) subunits - Each subunit has 4 transmembrane regions - α, β, and γ subunits (at least 1 of each, the other 2 can vary) |
|
|
What are the binding sites on the GABA/Benzodiazepine Receptor?
|
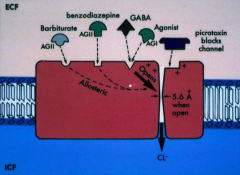
- GABA sites / receptor
- Benzodiazepine site / receptor - Barbiturate site / receptor |
|
|
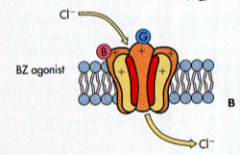
What is the effect of Benzodiazepines and Barbiturates on the GABA / BDZ receptor?
|
- Benzos enhance the action of GABA on this channel, allowing more Cl- to flow through for the same amount of GABA
- You still need GABA for this channel to work |
|
|
What ligands can bind to the benzodiazepine receptor?
|
- Agonists
- Antagonists - Inverse agonists |
|
What agonists bind to the benzodiazepine receptor?
|
Clinically useful benzodiazepines:
- Diazepam - Zolpidem - Other hypnotics |
|
|
What antagonists bind to the benzodiazepine receptor? Action?
|
Block action of Benzodiazepines at receptor
- Flumazenil |
|
|
What is the action of inverse agonists that bind to the benzodiazepine receptor?
|
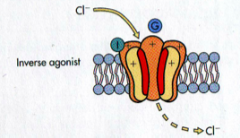
Block the action of benzodiazepines and can be anxiogenic
|
|
|
What is the mechanism of Buspirone?
|
- Partial agonist for 5-HT1A → inhibits AC → opens K+ channel
- Also binds to dopamine receptors |
|
|
Which benzodiazepines can treat anxiety?
|
- Diazepam
- Chlordiazepoxide - Alprazolam - Lorazepam - Clonazepam |
|
|
Which benzodiazepines be used as hypnotics?
|
- Flurazepam
- Triazolam - Lorazepam |
|
|
Which new drugs can be used as hypnotics?
|
- Zolpidem
- Zaleplon - Eszopiclone |
|
|
Which benzodiazepine used as a hypnotic has a longer duration of action? Shorter?
|
- Long duration: Flurazepam
- Ultra-short duration: Triazolam |
|
|
What is the role of lipophilicity in benzodiazepines?
|
Diazepam
- Highly lipid soluble: rapid absorption / fast onset and entry into brain - Rapid distribution after a single dose - Active metabolites change this in multiple dose situation Lorazepam - Less lipid soluble: slower absorption / onset of action - Longer duration of action - No active metabolites |
|
|
Which benzo has quick vs slow onset?
|
- Quick: Diazepam
- Slow: Lorazepam |
|
|
Which benzo has active metabolites vs none?
|
- Active metabolites: Diazepam
- No active metabolites: Lorazepam |
|
|
What are the CNS effects of benzodiazepines?
|
• Decreased Anxiety
• Sedation • Hypnosis • Muscle Relaxation • Anterograde Amnesia - IV administration • Anticonvulsant Action • Minimal CV and respiratory actions at therapeutic doses |
|
|
What are the drug interactions of benzodiazepines?
|
- Produce additive CNS depression w/ most other depressant drugs such as ethanol, other sedative hypnotics, and sedating anti-histamines
- Drugs that affect hepatic metabolism such as cimetidine |
|
|
What are the clinical uses of benzodiazepines?
|
- Anxiety states
- Sleep disorders - Muscle relaxant (diazepam) - Seizure treatment - IV sedation and anesthesia - Alcohol withdrawal (chlordiazepoxide) - Acute manic episodes (clonazepam) |
|
|
Which benzo can be used as a muscle relaxant?
|
Diazepam
|
|
|
Which benzo can be used for alcohol withdrawal?
|
Chlordiazepoxide
|
|
|
Which benzo can be used for acute manic episodes?
|
Clonazepam
|
|
|
What are the symptoms of benzodiazepine withdrawal?
|
- Anxiety
- Insomnia - Irritability - Headache - Hyperacusis (over-sensitivity to certain frequency and volume ranges of sound) - Hallucinations - Seizures |
|
|
How do you treat abuse of benzodiazepines?
|
- Gradual dose reduction
- Switch to longer acting drugs (eg, Lorazepam) |
|
|
What are the daytime sequelae of insomnia?
|
- Tired
- Fatigued - Sleepy - Anxious - Depressed |
|
|
What happens to the sleep cycles in patients taking benzodiazepines?
|
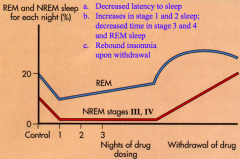
- Decreased latency to sleep
- Increases in stage 1 and 2 sleep, decreased time in stage 3 and 4 and REM sleep - Rebound insomnia upon withdrawal (rebound REM - get more REM sleep) |
|
|
What are the adverse effects of benzodiazepines for insomnia?
|
- Daytime sedation
- Ataxia - Rebound insomnia - Tolerance and dependence - Occasional idiosyncratic excitement and stimulation - Increased death rate associated with use?? |
|
|
What is the mechanism of Zolpidem and Zaleplon?
|
- Non-benzodiazepines
- Binds to BDZ (benzo) receptor on GABA receptor complex |
|
|
What are the uses of Zolpidem and Zaleplon?
|
- Weak anxiolytic
- Muscle relaxant - Anti-convulsant at hypnotic dose |
|
|
What are the effects of Zolpidem and Zaleplon on sleep?
|
- Stage 3 & 4 sleep preserved
- Minor effects on REM sleep |
|
|
What is the duration of Zolpidem and Zaleplon? Route of admin?
|
Zolpidem:
- Duration: 5-6 hours - Sustained released prep duration: 7-8 hours - Also as oral spray for problems with sleep initiation - Also as sublingual tablet for middle of the night waking Zaleplon: - Faster onset of action (better for problems with sleep initiation) - Shorter terminal elimination half-life |
|
|
What is the mechanism of Eszopiclone?
|
Interacts with GABA-receptor complex at binding domains located close to or allosterically coupled to Benzo receptor
|
|
|
Which drug is approved for use for six months? Dependence? Withdrawal?
|
Eszopiclone - low likelihood of dependence and withdrawal
|
|
|
What is the mechanism of Ramelteon?
|
Melatonin MT1 and MT2 receptor agonist
|
|
|
What is Ramelteon indicated for?
|
Treatment of insomnia characterized by difficulty in falling asleep, not a controlled substance
|
|
|
Which barbiturate is used as a hypnotic?
|
Phenobarbital
Pentobarbital |
|
|
What are the characteristics of Phenobarbital and Pentobarbital metabolism / pharmacokinetics?
|
• Rapidly absorbed and distributed.
• Highly lipid soluble compounds such as thiopental distribute rapidly to brain. Action terminated by redistribution, • Can induce own metabolism and that of other drugs. • Eliminated primarily by renal excretion. |
|
|
What are the adverse effects of Phenobarbital and Pentobarbital?
|
- General CNS depression
a) sedation b) hypnotic action c) anesthesia - Anticonvulsant - Respiratory depression - CV effects minimal w/ hypnotic doses, but high doses can decrease mean arterial and pulse pressure - Induce hepatic drug metabolism - Exacerbates acute intermittent porphyria - Tolerance: both metabolic and pharmacodynamic |
|
|
Do Phenobarbital and Pentobarbital cause physical dependence? Implications?
|
Repeated use of barbiturates may result in withdrawal symptoms upon cessation of use, including:
- Anxiety - Agitation - Insomnia - Tremor Life threatening seizures may occur *Abrupt withdrawal in chronic users is contra-indicated* |
|
|
What can occur with acute poisoning of Phenobarbital and Pentobarbital? How do you treat?
|
- Stupor
- Coma - Respiratory depression - Treatment involves removing any unabsorbed drug, supporting respiration, and preventing complications |
|
|
What drugs can Phenobarbital and Pentobarbital interact with?
|
Other CNS depressants
- Alcohol - Sedative hypnotics - Anti-histamines Drugs that affect microsomal drug metabolism |
|
|
How do barbiturates compare to benzodiazepines for the amount of CNS effects?
|
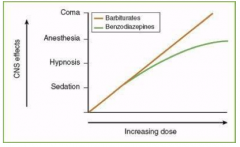
Barbiturates cause more CNS effects at increased dose
|
|
|
What is the function of skeletal muscle relaxants?
|
Drugs used to reduce muscle tone associated with spasticity related to multiple sclerosis injuries and other muscular skeletal disorders
|
|
|
What drugs are skeletal muscle relaxants?
|
- Diazepam
- Baclofen - Tizanidine |
|
|
How does Diazepam act as skeletal muscle relaxants? Uses?
|
- Reduces spasticity is at least partly mediated in the spinal cord
- Can be used for muscle spasms of almost any origin (including trauma) - Produces sedation in most patients at the doses required to reduce muscle effect |
|
|
How does Baclofen act as skeletal muscle relaxants? Uses?
|
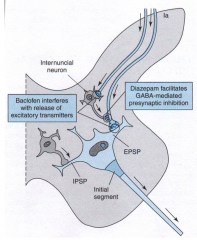
- GABA-mimetic agent that works at GABA-b receptors
- This results in hyperpolarization, causing presynaptic inhibition - This can result in decreased release of excitatory transmitters such as glutamate - As effective as Diazepam but is better because it produces much less sedation |
|
|
How does Diazepam compare to Baclofen in utility?
|
They are equally useful, but Baclofen produces much less sedation
|
|
|
How does Tizanidine act as skeletal muscle relaxants? Uses?
|
- α2-adrenergic agonist that is related to clonidine
- May enhance presynaptic and postsynaptic inhibition - Similar efficacy as diazepam and baclofen in relieving muscle spasm |
|
|
What are the side effects of Tizanidine? Drug interactions?
|
- Drowsiness
- Hypotension - Dry mouth - Asthenia - Interacts with Ciprofloxacin and Fluvxoamine (CYP1A2) |
|
|
28 yo woman has suicide attempt. Took bottle of pills for nervousness and insomnia. She appears lethargic but responsive to pain. HR, BP, and SaO2 normal. Pupils normal. Given IV dextrose.
What drug do you think that she took? a) Alprazolam b) Sertraline c) Lorazepam d) Oxycodone e) Zolpidem |
Lorazepam (this is the only benzo that works for both relieving anxiety and hypnosis)
|
|
|
28 yo woman has suicide attempt. Took bottle of pills for nervousness and insomnia. She appears lethargic but responsive to pain. HR, BP, and SaO2 normal. Pupils normal. Given IV dextrose.
What drugs might have exacerbated her overdose situation? a) Alcohol b) Cimetidine c) Cocaine d) Methamphetamine e) Phenelzine |
Alcohol
|
|
|
28 yo woman has suicide attempt. Took bottle of pills for nervousness and insomnia. She appears lethargic but responsive to pain. HR, BP, and SaO2 normal. Pupils normal. Given IV dextrose.
What is a specific antidote for the drug she overdosed on? a) Eszopiclone b) Flumazenil c) Flurazepam d) Naltrexone e) Paroxetine |
Flumazenil
|
|
|
2 yo college senior presents w/ chest pain, increased HR, sweating, SOB. Thinks a heart attack. No history of heart disease. Physical exam within normal limits, except tachycardia.
What is the likely diagnosis? a) Acute stress disorder b) Generalized anxiety disorder c) Hypochondriasis (Illness anxiety behavior) d) Panic disorder e) Post traumatic stress disorder |
Panic Disorder / Panic Attack
|
|
|
22 yo college senior presents w/ chest pain, increased HR, sweating, SOB. Thinks a heart attack. No history of heart disease. Physical exam within normal limits, except tachycardia.
Which of the following is likely to be most effective immediately? a) Antidepressant b) Antipsychotic c) Benzodiazepine d) Beta-blocker e) Buspirone (Buspar) |
Benzodiazepine
|
|
|
22 yo college senior presents w/ chest pain, increased HR, sweating, SOB. Thinks a heart attack. No history of heart disease. Physical exam within normal limits, except tachycardia.
Which of the following is likely to be most effective in the long term? a) Antidepressant b) Antipsychotic c) Benzodiazepine d) Beta-blocker e) Buspirone (Buspar) |
Anti-Depressant
(for panic disorder, some anti-depressants are very effective: SSRIs, TCAs - but these meds take 4-6 weeks to work) (Buspirone - is only used for GAD |