![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
43 Cards in this Set
- Front
- Back
|
What 7 factors contributed to the growth of cognitive therapy? |
1) dissatisfaction with current conceptualization of learning and entering of CT into animal learning : expectancies, learned helplessness, meaning of stimuli to rat 2) dissatisfaction of conditioning explanations of behavioural treatments. Things like SD were considered to work bc of their learning (but not true since SD works without UR or heirarchy) 3) We need to use cog variables to explain conditioning in humans- Greenspoon effect, LOC 4) Growth of cog-based theories of personality- Social learning theory, personal constructs 5) Use of cognitive variables to explain emotionality- Lazarus theory or appraisals 6) renewed interest in mental imagery, consciousness form a scientific perspective 7) interest in role of language as it effects overt behaviour- stress inoculation, self-instructional training |
|
|
What is Bolles contrast effect? Seligman's learned Helplessness? |
BOLLES: degradation in performance when a less-valuedreward is suddenly introduced after initial learning with amore valued reinforcer- explained it with expectations - btwn discriminative stimulus and reward, and between the response and reward SELIGMAN: animal cant avoid the pain so learns to not even try. Side note: you can get resistance to this is you first TRAIN them to be passive to escape= omission training there fore what is important in the paradigm is not the learned motor behaviour but the cognitive strategy |
|
|
What is the Greenspoon Effect? The LOC? What do these illustrate? |
GREENSPOON: group results show conditioning withoutawareness in a fashion similar to animal learningwhereas an analysisof individual subjects reveals a very different non-animal process, that isan active, searching and then willing participation in thelearning process. giving subtle cues to condition ppl) ROTTERS Locus of Control: a generalized expectancy regarding the persons belief in the connection between their behaviour and outcomes. You can have an internal LOC (strong respons-outcome ass- you think you control everything) or an external one (weak association, you think things come from world) ** this shows why in a perceived skill task, initial continuous reinforcement causes high resistance to extinction BOTH of these show the modulating effect of cognitive variables on the learning principles in humans |
|
|
Social learning theory (Rotter); Theory of personal Constructs (George Kelly) |
ROTTER: the probability of any behaviour is a function of a) belief that a behaviour will yield the reinforcement + b) the value of the reward for the person. The theory states that the LOC is important in determining this relationship. Some people have questioned whether LOC is so general or if it caries across life contexts ; KELLY: constructs are internal representations that construct experiences. for ex. what is dif between mom and sister? good mental health involves the ability to test out such constructs and identify them |
|
|
Describe Lazarus' theory of primary and secondary appraisal |
A theory that explains emotions cognitively! primary appraisal- you walk in and quickly judge or appraise situationSee threat (or not). Then there is secondary appraisal AKA COPING. this can modulate the sensations of the threat or change the meaning of the situation, or you do something behaviorally. The emergent emotion is the product of the interaction of initial reaction to situation, attempts at changing aspects of the situation, as well as changing the meaning of the emotional response |
|
|
Meichenbaum's self-instructional training & stress inoculation (4) |
Primary sensation is like light or sound or emotionality. Secondary is like meaning of words, internal voice. Self instruction take young kids and teaches them to respond to secondary and not primary cues, by speaking out loud. He then applied this to adults with stress inoculations: 1) instruction in conceptualization of stress- it is an interaction not environmental variable 2) acquisition of coping skills 3) training in self-camling 4) practice guided by appropriate self-talk |
|
|
What are the two classes of cognitive variables? |
Products: - expectations - automatic thoughts - beliefs/attitudes - philosophies - propositional knowledge (if X then Y) - schemas: guide perception, behaviour, memory Processes: - attention (think in anxiety, sex) - attribution/explanatory style - problem-solving |
|
|
3 types of expectancies |
1) Generalized expectancy, Rotter's locus of control“efforts and hard work rarely help in anything” says the agoraphobic 2) Outcome prediction in a specific situation eg optimism in situation X“I’ll probably panic in the metro” …. 3) Personal abilities in specific situations (Bandura's self-efficacy)- What you believe you are capable of doing |
|
|
What experimental evidence supports the utility of schemas? (2) How can a clinician discover schemas? |
-Studies that reveal longer processing times for verbal material semanticallyassociated with the putative schema. IE. longerreaction times to colour name depression-relevant words in the Stroop Testcompared to the RT for non-schema related or neutral words. -A more recent experimental test involves the brain’s evoked potentialresponse (P 300) to novel stimuli or stimuli with salient information.Hardi et al ( 2007) have shown that depressed subjects had an augmentedP300 wave response to verbal material that was negatively charged. How can a clinician discover schemas? DOWNWARD ARROW: look at a statement, and see what is the implication of that statement, getting at the core meaning the person has about the world to say that |
|
|
Attribution styles |
the process involved: #1 Self-observation of a behaviour#2 Determination of causality. People can explain according to : inside the person or in the environment, something that is stable versus temporary something that is specific versus global but there are also others like gamblers attribute failures to "near wins" instead of signs of stopping |
|
|
Define problem solving in CBT. Who is the forerunner in this research? Explain the process. Give examples of how to use it in CBT |
attempts to develop effective or adaptive solutions to stressfulproblems in living where no immediate coping response is automaticallyavailable. ARTHUR NEZU The cognitive process can be broken down into : 1) problem orientation: accept problems as part of life, boosts self-efficacy and persistence 2) Problem-solving process: - define problem - generate solutions and alternatives - decision-making - organize pros and cons against values - implementation and evaluation * the first question to ask is "what do you want out of this" look also at visualization of problem, simplification Can be used to increase adherence for a medical program (how can I remember my meds), addressing relapse, or stress from conflicts |
|
|
Rational Emotive Therapy (Albert Ellis) |
- one of the first applications of cognitive variables in therapy - involves an ABC model but a different one Eliciting event (antecedent) -- first belief -- emotion--second belief (react to the emotion, beliefs about having the emotion) - often the problematic response to a situationbecomes itself the problem. - Ellis says people are so irrational because of our tendency to be self-blaming and self-depreciating -a trend reinforcedby our culture. |
|
|
What are the general qualities of the CT approach? |
1) Psychoeducation - teach them the cog model: thinking produces feelings - Watsons selection tasks shows us that sometimes we seek things that confirm our beliefs instead of looking for disconfirming evidence 2) therapy processes where we change the thoughts - Using thought records (evidence that supports thought, evidence that does not, alternative view) - downward arrow - socratic dialogue (asking deeper questions to probe self-knowledge) - cognitive restructuring - how can we spin this differently? - actually doing behavioural experiments with them! (this is what you expect to happen lets do it and see) |
|
|
What is some criticism of cognitive approach? (4) |
- cognitions are not causal, we still have to explain cognitions (skinner) - is it valid? do specific beliefs specific risk factors to later troubles? time-lagged structural equation modeling studies will helpanswer this question. - uses self report to assess similar variables in same person at same time - developmental/constructivists think that not all emotionality is post-cognitive and one needs to intervene at a higher level of conceptualization |
|
|
Discuss attitudes around addiction and alcohol |
- word addiction comes from latin "addioo" meaning giving over, in a positive sense it means devotion. The word was not always negative - Rev. Wayne Oates coin the term Workalcholic - Temperance movement was by wives who thought their husbands were indulging too much on alcohol to the detriment of the family, an afterwards abstinence was promoted and excessive drinking mixed with religion became sinful |
|
|
What does the effect of a drug depend on? (6) |
- type of drug - dose - dose scheduling (fixed or when you want it) - pharmacokinetic factors (what the body does to the drug) - pharmacodynamic factors (what the drug does to the body- biochem and phys) - psychosocial factors like environment, cultural norms, expectations, drug-seeking behaviour |
|
|
What are some pharmacokinetic factors? pharmacodynamic? |
- distribution - transformation - mostly by the liver, often into so-called active metabolites - Excretion - Diffusion across protective membranes - action on receptor site- either agonists (morphine) or antagonists (naloxone) - mode of action - blocking ion channels, inhibiting or stimulating enzyme, etc. |
|
|
Discuss AA or medical model of alcoholism vs the CBT model of alcohol abuse in terms of: Nature of the disorder, course of disorder, therapy delivered, advantages and disadvantages of each model |
Nature of the disorder: AA sees it as a disease, genetic vs cbt which sees it as changeable Course of disorder: AA sees it as lifelong- you are always an alcoholic. CBT sees it as something you overcome Therapy delivered: AA has 12-step process that focuses on self-disclosure and abstinence. CBT looks at changing your behaviour and thoughts to make them more adaptive. AA is in a group and CBT is usually one on one with therapist. Approach: AA focuses on religion, whereas CBT focuses on self-efficacy. AA uses same 12 steps for everyone, while CBT focuses on heterogeneity and deals with each case differently Advantages of each: - CBT allows for social drinking in some patients after, is not religious, and improves self- control by anticipating likely problems and identifying high risk situations - AA uses a group/community setting which is helpful, and has 12 steps that are explicit . There is also always help available and it is free. For some people, abstinence is the best thing Disadvantages: -CBT: have to work on generalization, doesn't involve a community in the same way as AA - AA: the use of religion promotes a lack of self-efficacy and responsibility for actions. Abstinence may not be realistic. |
|
|
Typically, withdrawal symptoms are opposite that produced by the drug. Discuss this for ETOH, Bzs, cocaine, amphetamines |
|
|
|
Describe tolerance |
- means you get a progressive loss in potency of a drug with repeated administrations - LD50 means lethal dose is 50 mg - tolerance can be pharmacological ( drug more quickly metabolized or there is increased enzyme degradation it can also be behavioural (person learns to do the task which was once impaired by the drug in another way |
|
|
According to WHO what is alcoholism? (3) What are some specific risk factors for abuse |
According to the World Health Organization, alcoholism is based on threequalities: 1) Excessive indulgence 2) Psychological dependency 3) Life disruption. risk factors: male 30-55 occupations like construction trait of sensation seeking having a father who drank early drinking |
|
|
Wernike-Korsakoff syndrome |
Starts with Wernike disease (consisting of ocular paralysis, ataxiaOr problems with balance and confusion with speechcharacterized by lack of meaning.) If the patient survives, the condition progresses to Korsakoffstate that is marked by severe retrograde and anterograde amnesia.Symptoms of the latter are reflected in the patients’ meagerconversational content, apathy and confabulation. |
|
|
The "sleeper" in alcohol abuse |
The "sleeper" in alcohol abuse is tobacco, since a recent study showed that51% of the deaths in a sample of 853 alcoholics treated for their substanceabuse were related to tobacco. |
|
|
briefly, hat are some physical, cognitive, psychosocial effects of abuse? |
physical: G-I defects, hangover, cirrhosis Cognitive: seizures, alcohol dementia, problem solving impairments, Wernike Psychosocial: crime, missing work, lack of motivation |
|
|
What are some possible causes or maintaining factors of alcohol abuse? (6) |
1) environmental stimuli/ availability - price elasticity of alcohol, being able to get it easily online everyone around you doing it 2) modelling- culture, family, social sphere restricted by drinking to people who drink 3) reinforcement 4) classical conditioning- the drug response can be conditioned (environ cues), the craving can be, AND opponent process conditioning 5) cognitive factors- self efficacy low, people believe it makes them more funny etc. 6) availability of alternate reinforcers: substitutes- decreasing cost of valium decreases heroin consumption, and Complementary: alcohol access increases cigarette consumption |
|
|
What is opponent process conditioning? |
You always take the certain amount of heroin in the same environment. Then you go to a new environment and tak ethe same amount you may die. In the old environment there is an anti-drug homeostatic conditioned process that maks your tolerance higher. This shows that classical conditioning has occurred, and these visual cues are linked to your drug craving and drug taking behaviour |
|
|
What are examples of primary and secondary positive and negative reinforcers for alcohol abuse6 |
Primary Positive: euphoria, high Primary Negative: escape from withdrawal or biological unpleasantness Secondary Positive: drug taking becomes a culture, social norms, Secondary Negative: escape from social unpleasantness or anxiety for ex. |
|
|
Describe a vicious cycle with alcoholism |
lack of effective coping with stressleads to alcohol intake to reduce anxiety which only reducesone's capacity to cope while increasing exposure to thosewho abuse and augmenting the difficulties which need to becoped with. a specific behavioural deficit like lack of expression of feelings combines with cognition that drinking will help produces the powerful negative reinforcement of drinking |
|
|
Describe the Integrated Cognitive- Behavioural treatment model |
- first a basic assessment which looks at psychosocial-legal history, a functional behavioural assessment, measure of frequency of drug use, medical assessment - then assessment of readiness to change - key aspect is that the motivation to use is a behaviour and can be changed - uses motivational interviewing - uses specific interventions with a tailored approach to increase competency, change beliefs, and examine cues - also prepares people for relapse - telling them that this might happen and its okay, this is how we will deal with it |
|
|
How do you ass readiness to change? |
People can be in different stages: Pre contemplation- denial Contemplation- -admits to the problem however the desire to quit isoften expressed as "yes, but" that is, there is stillstrong ambivalence Determination- more motivated to take action Preparation- still drinking! but has attempted to stop Action- modifies behaviours Maintenance |
|
|
FRAMES acronym of motivational interviewing |
FEEDBACK- personalized, ie level of liver enzymes RESPONSIBILITY- shift to client ADVICE MULTIPLE options for goals and solutions EMPATHETIC SELF-EFFICACY- encourage it |
|
|
Abstinence Violation Effect; What might relapse prevention therapy involve? |
that once you have the initial breakfrom abstinence then you are “screwed” – so if you do then it gives you an excuse to keepgoing You build into CBT strategies for abstinence violation. There are decisions allthe way along the line, if you break it once then you have the opportunity to makeanother decision –you can stop. RP may involve: - identify high risk situations - coping training - develop specific strategies - view lapses as learning experiences |
|
|
What are 3 major areas of disagreement between CBT and AA? |
- predisposing alcoholic or addictive personality- lack of evidence from many studies of any "alcoholicpersonality"(eg,Vaillant's study) - physiologically-based loss of control?-belief in loss of control produces loss of control. - value of controlled drinking (CBT believes this) as a desiredoutcomefor some problem -drinkers in contrast to AA assertionthat the only treatment for anyone is abstinence. Whowould benefit from what approach?-not all abstinence treatments achieve abstinence |
|
|
Who were the early forerunners of modern Social skills training? (3) |
Salter, conditioned reflex therapy developed in 1949 to decrease socialanxiety through skill development. Mowrer, the originator of the two-factor theory of avoidance learning, alsodeveloped an unusual form of therapy which he referred to as integritytherapy - a therapy to encourage self-disclosure of moral transgressions. Kelly George, fixed role therapy, encourages patients to test-out their ownpersonal constructs as well as other constructs by engaging in various rolesboth in and outside therapy. |
|
|
Define social competence; What is Assertion? |
social competence: the net impact of the person's social skills actingon his or her interpersonal field or environment to achieveadaptive instrumental or affective goals. Assertion is self-direction, following your own agenda (while still being honest and respecting others). It excludes agression, submission, disrespect, manipulaton |
|
|
What are the underlying assumptions of SST? |
- angry feelings are OK - honest about feelings is the best policy - tries to teach i-talk, where people are encouraged to express feelings in a non-blaming way |
|
|
What are the 3 models of causality in SST? |
1) requisite skil deficiency- individual lacks the ability to express an appropriate social response 2) Skill exists but is not displayed due to a) faulty discrimination of situation (person doesnt read situation as calling for assertion) or b) Suppression of assertive behaviour (by anger or anxiety) 3) behaviour exists and is displayed, but person judges it to be unacceptable |
|
|
Describe the model of social skills by Liberman and Wallace |
convinced therapists to go beyond just expressive training to look at perceptual and cognitive processes involved |
|
|
Assessment in SST |
- first a functional analysis, where specific deficit is described - then you quantify the behavioural deficiency, perhaps by questionnaires (basic social competence= Morningside scale; formal shyness= Rathus assertion inventory), or maybe by having them role-play a situation |
|
|
How is SST carried out? |
- assessment - format training (individual vs group, weekly vs massed session, using co-therapist,ect) - preparation: teach about SSY assumptions, define assertion etc., stress mode of causality (ie lack of experience not underlying unconscious problems), explain techniques - select targets (look at common situations or themes) - describe behaviour: cognitive, behavioural, affective domains - Modelling - role-play or behaviour rehearsal, along with coaching and feedback (non-judgemental, concrete, positive before negative) - cognitive interventions - Promoting generalizations - homework |
|
|
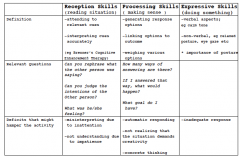
Cognitive interventions in SST |
- discuss faulty cognitions serving as blocks to performance like shame connected to poor social performance, exaggerated belief that assertion will lead to conflict, thinking others are more powerful, etc. - remediation of basic cognitive prerequisites - ie. if you cant remember what a person just said in a convo its awkward, so memory is a prerequisite. - remediation of receptive and processing deficits- can you identify the emotion expressed in this video, develop alternative courses of action - teaching a cognitive strategy: dont just focus on specific situations and responses, train more broad things like how to deal with conflict |
|
|
What factors facilitate modelling (5) (Bandura) ? |
1) attention: what important aspects are being attended to 2) representation: capacity to encode and remember the models behaviour 3) Motivation: Was the model relevant to the person and their situation 4) Reproduction: can the behaviour be copied? 5) Identification: does person identify with model demographic features, and can they see the dif between their actions and the models? |
|
|
how can you promote generalizations in SST? |
- loose training, eg spontaneously generated topics, no formaltarget setting etc - multiple and even unfamiliar training confederates - naturalistic training situations - role-plays with unanticipated outcomes versus those which providedlittle resistance in early stages of therapy |