![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
946 Cards in this Set
- Front
- Back
|
What is the cell membrane? |
Composed of a phospholipid bilayer
Lipid-soluble molecules and gases diffuse through readily
Water-soluble molecules cannot cross without help such as polar molecules and proteins
Impermeable to organic anions such as proteins
Permeability depends on molecular size, lipid solubility and charge |
|
|
What does the permeability of a cell membrane depend on? |
Molecule size, lipid solubility and charge |
|
|
What is simple diffusion? |
Small, lipid-soluble molecules and gases pass either directly through the phospholipid bilayer or through pores Movement of substrate down its concentration gradient Relative rate of diffusion is roughly proportional to the concentration gradient across the membrane Passive (no energy input required from ATP) |
|
|
What is facilitated diffusion? |
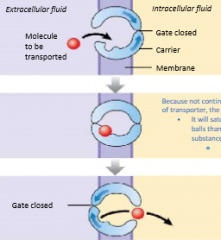
Process of diffusion where molecules diffuse across membrane with the assistance of carrier proteins Movement of substrate down its concentration gradient Energy comes from the concentration gradient of the solute Passive Because not continual passage and a finite amount of transporters, the system will saturate eventually when soluble molecules exceed transporter molecules |
|
|
What are carrier proteins? |
They aid in the movement of polar molecules across the cell membrane |
|
|
What is active transport? |
Mechanism to move selected molecules across cell membranes, against their concentration gradient Substrate binds to protein carrier that changes conformation to move substrate across the membrane Active (requires energy from ATP hydrolysis like ATPase which is a Na+/K+ pump) |
|
|
Why does active transport require energy? |
Going against the concentration gradient |
|
|
What is secondary active transport? |
When a substance is carried up its concentration gradient without ATP catabolism Kinetic energy of movement of one substance down its concentration gradient powers the simultaneous transport of another up its concentration gradient It rides on the 'coat-tails' of primary active transport and do not themselves require ATP Sequential binding of a substrate and ions to specific sites in the transport protein induces a conformational change in the protein Powered by the chemical energy in the ion diffusing down its concentration gradient and this energy is used to 'push' some solutes against its concentration gradient |
|
|
What powers secondary active transport? |
The chemical energy in the ion diffusing down its concentration gradient and this energy is used to 'push' some solutes against its concentration gradient |
|
|
What are poor loops in channels? |
Molecules that dangle inside the channel They give physical properties for specific and selectivity filtering These 'pores' are called membrane channels |
|
|
What are gated channels? |
Holes in the membrane that can be opened or closed |
|
|
What are ligand gated channels? |
Binding of chemical agents Cell membrane receptors are part of the body's chemical signaling system The binding of a receptor with its ligand usually triggers events at the membrane such as activation of an enzyme |
|
|
What are voltage gated channels? |
Voltage across the membrane Membrane channels that are sensitive to potential difference across the membrane where changes the conformation of the channel subunits causing a diffusion pore to be created |
|
|
Do all cells generate a membrane potential? |
Yes where inside is more negative than outside usually All cells poses a non-zero membrane potential |
|
|
What is the S4 protein in the voltage gated channel |
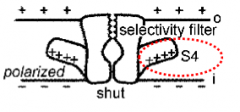
Voltage sensing mechanism. The 4th transmembrane domain of the protein. Are positively charged Stick out the side of the protein Natural position of the S4 is up towards outer surface of the cell membrane but when membrane is polarized, positively charged S4 is attracted downwards to the negatively charged inner surface of the membrane, shutting the game. When depolarized, the membrane at ~-50mV, no lover provides sufficient electrical attraction to hold S4 downwards, it will migrate back up causing the pore to open allowing ions to diffuse through |
|
|
What is endocytosis? |
Inward 'pinching' of membrane to create a vesicle Usually receptor-mediated to capture proteins, from outside to inside |
|
|
What is exocytosis? |
Partial or complete fusion of vesicles with cell membrane for bulk trans-membrane transport of specific molecules, from inside to outside There are two types: 1) Exocytosis 1: The more rapid mechanism is dubbed the 'Kiss and Run' 2) Exocytosis 2: Full exocytosis |
|
|
What is exocytosis 1? |

Kiss and Run The secretory vesicles dock and fuse with the plasma membrane at specific locations called 'fusion pores' Happens in a transient matter Vesicle can connect and disconnect several times before contents are emptied Generally, only part of the vesicle contents diffuse into the interstital fluid, used for low rate of signaling |
|
|
What is exocytosis 2? |
Full exocytosis This involves complete fusion of the vesicle with the membrane, leading to total release of vesicle contents at once Necessary for delivery of membrane proteins and high levels of signaling Must be counterbalanced by endocytosis to stabilize the membrane surface area |
|
|
What are the two conditions to generate membrane potential (MP)? |
1) Create a concnetration gradient: an enzyme ion pump (functions as an ATPase) must actively transport certain ion species across the membrane to create a concentration gradient 2) Semi-permeable membrane: allows one ion species to diffuse across the membrane more than others Diffusion of that ion species down its concentration gradient creates an electrical gradient |
|
|
What is the Na+/K+ pump? |
All cell membrane is loaded with Na+/K+ pumps, that is the staple of all living cells Na+, K+ - dependent ATPase is enzyme that moves Na+ out of the cell and K+ into the cell by breaking down ATP For each ATP molecule broken down, 3 Na+ ions are pumped out and 2 K+ pumped in to create a concentration gradient Consumes 1/3 of energy needs of body Na/K inequality greater potential difference of -10mV because both are cations and as this pumping process occurs, the inside becomes more negative |
|
|
Is our resting Mp roughly -10mV? |
No, the actual resting MP in neurons is closer to -70mV |
|
|
Explain resting membrane potential |
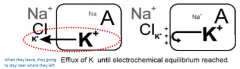
Since our resting MP is closer to -70mV, this is due to diffusion of K+ ions outwards The 'resting' membrane is most permeable to K+ ions K+ diffuse out of the cell, down the concentration gradient via K+ channels while Na will do nothing so the membrane potential will slowly keep going down Cations accumulate on the outside of the membrane, leaving a net negativity inside membrane This efflux will occur until there is a such a build up of "+" charge on the outside of the membrane that further diffusion of K+ is repelled by the electromagnetic force (causing a reach of equilibrium) |
|
|
Explain K+ channels |
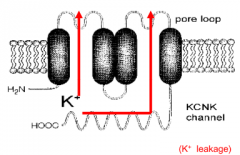
There are 2 pores within the structure through which only K ions can pass There will be K+ leakage at all times |
|
|
What is Nernest equation? |

Can be used to calculate the equilibrium potential Describes the balance between the chemical work of diffusion with electrical work of repulsion The equation gives the potential difference across the membrane, inside with respect to outside, at equilibrium The result is valid if and only if one ion species is diffusion across the membrane |
|
|
Explain Na+ equilibrium potential |
Under certain circumstances, permeability of Na+ can be dominant and much more than the K+ ion and MP can change drastically If membrane properties change to make the membrane most permeable to Na+, then there is a net Na+ current inward Membrane potential is positive inside with respect to outside: ENa+ = +60mV |
|
|
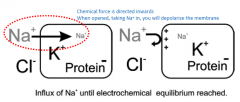
In the sense of membrane potential, what is the purpose of Cl- ions? |
Inside the cell, we have large proteins (which are basically trapped, they can only get across the outside using exocitosis) and since they tend to have "-" charges, the Cl- ion is pushed out of the cell
Therefore, the Cl- ions tend to be more concentrated on the outside in the extracellular space This is due to anion proteins present on the inside and not due to active pump You will find more Cl- on the outside and less on the inside |
|
|
Explain Na+ channels |

To generate a signal, membrane increases its conductance by opening a channel permeable only to Na+ ions
This is a voltage-gated Na+ channel
In normal resting MP, this Na+ channel is shut
To open this Na+ channel, we need to depolarize (removing the polarization) the membrane by a certain amount (from about -70mV to ~-55mV)
Na+ channel only opened by depolarizing the membrane to a threshold potential of about -55mV
Theoretically, Na+ channels cannot go above +60mV but before getting to that, at about +30mV, the inactivation gate closes (and it will stayed closed unless it goes below -55mV to be reactivated again) |
|
|
What is action potential? |
AP is essentially an impulse, a very short lived change in the MP, an AP is used as a signal (like a flux) You can only produce an AP in membrane that contains the voltage-gated Na+ channels By definition, the presence of voltage-gated Na+ channel make the membrane 'excitable' Na+ inactivation leaves K+ leakage as main current, and resting potential is restored (when between -55 and -70, K is dominant but when above -55, Na will be dominant) |
|

Fill in this chart: |
1) Resting membrane potential 2) Depolarizing stimulus 3) Membrane depolarizes to threshold. Voltage-gated Na+ and K+ channels begin to open 4) Rapid Na+ entry depolarizes cell 5) Na+ channels close and slower K+ channels open 6) K+ moves from cell to extracellular fluid 7) K+ channels remain open and additional K+ leaves cell, hyperpolarizing it 8) Voltage-gated K+ channels close, less K+ leaks out of cell 9) Cell returns to resting ion permeability and resting membrane potential |
|
|
What causes blimps in action potential? |
A depolarizing below threshold (a subthreshold) |
|
|
Define threshold in the aspect of action potential |
Minimum depolarization necessary to induce the regenerative mechanism for opening of Na+ channels |
|
|
At what voltage starts an action potential? |
-55mV |
|
|
What is supra-threshold and what does it cause? |
Huge jump in voltage and cause an action potential Action potential from threshold and supra-threshold stimulus have the same magnitude |
|
|
How is information from a stimulus intensity coded? |
By changes in the frequency of the action potential (frequency coding) |
|
|
What are refractory periods (RP)? |
After we generate an AP and inactive the Na+ channels, we have a period in which all or some Na+ channels are inactivated
Na+ channels remain inactivated until membrane potential drops below 'threshold', then channels reconfigure to their original state and membrane becomes excitable again
There are two types of RP: Absolute and Relative
Absolute RP is none of the channels are reconfigured. When a channel is inactivated, you cannot fire an action potential
Relative RP: Some but not all of the channels are reconfigured. You can actually generate a smaller action potential during the relative RP |
|
|
How can you completely block the membrane from producing an AP? |
By keeping the membrane depolarized using an depolarization block. If you permanently depolarize the membrane, you keep it at 20mV (above threshold), the Na+ channels will be permanently inactivated and you will not be able to generate another AP |
|
|
How can you keep the membrane depolarized? |
By destroying the concentration gradient for K+ by introducing more K+ in the extracellular space (example: KCl injection) This will result in permanent Na+ inactivation and the membrane will remain in absolute refractory state and the membrane becomes in-excitable |
|
|
What is after-hyperpolarization? |
Due to the presence of this "extra" K+ channels, in conjunction with the leakage of K+ channels, we have much greater outward K+ current This results in the MP to be more polarized than normal Thus, the voltage-gated K+ channels cause hyperpolarization after the AP So instead of the MP being repolarized to -70mV, the MP might be repolarized to -80mV |
|
|
What is impulse conduction? |
When a patch of excitable membrane generates an action potential, this causes an influx of Na+ and reverses the potential difference across the membrane The local reversal in potential temporarily goes from "-" on the inside to "+" on the inside The local reversal in potential serves as the source of depolarizing current for adjacent membrane Na+ channels open in adjacent membrane Therefore, once started, an AP will propagate from its origin across the rest of the cell |
|
|
What is an axon? |
A long extension of the cell body (like a wire) that carry AP away to some other location You will find a lot of voltage gated-channels here. The action potential will propagate towards the end/axon terminal Only neurons with long axons and muscle cells generate propagating action potentials |
|
|
What is a synapse? |
The region where an axon terminal communicates with its postsynaptic target cell |
|
|
In cable properties, what is "length constant" (lambda) used to measure and what is it? |

It is used to measure how quickly a potential differences disappears (decays to zero) as a function of distance Thus, the conduction velocity of an AP along an axon depends on the membrane length constant, lambda Length constant is defined with internal resistance, extracellular fluid resistance and membrane resistance Since the extracellular fluid resistance is not adjustable and is relatively low, it drops from the equation and we're left with internal resistance and membrane resistance Ideally, you want to increase the length constant as much as possible so that the depolarzing current will spread a great distance |
|
|
What happens if you increase the length constant by increasing the diameter of an axon/cable? |
The larger the diameter = less internal resistance = less voltage is lost across that resistance as the current travels down the membrane |
|
|
What happens if you increase the length constant by increasing the membrane resistance of an axon/cable? |
The higher the membrane resistance = less current is leaked out = current is forced down the membrane |
|
|
What is myelination? |
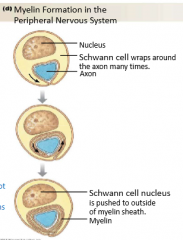
Increasing membrane resistance is the most efficient means of increasing conduction velocity 'Glial' cells are cells that assist the nervous system, they are required for nutrition and increase membrane resistance Specialized 'glial' cells (schwann cells of the PNS or olgodendrocytes within the CNS) wrap around successive sections of an axon for myelin sheath (Glial cells are sponsible for myelination) It does 50-100 layers wrapping around the axon which greatly increases the membrane resistance causing reduced leaked of current out of the membrane The negative aspect of this is it takes a lot of space causing it to be bulkier which means you cannot myelinated all axons There are small gaps left between adjacent portions of the myelin sheath (a glial cell will wrap one section and next glial cell will wrap another section. These gaps are called the Node of Ranvier |
|
|
What are glial cells? |
Cells that assist the nervous system They are required for nutrition and increased membrane resistance (myelination) |
|
|
What are Schwann cells? |
Glial cells in the PSN that wrap around successive sections of the axon to create a myelin sheath (myelination) Schwann cells wrap around a single portion of the one axon (cytoplasm is all squeezed-out) Participate in repair process after injury Can be stained by 1E8 and Herp |
|
|
What are Oligodendrocytes? |
Glial cells in the CNS that wrap around successive sections of the axon to create a myelin sheath (myelination) Oligodendrocyte has a number of processes that streaks out line an octopus and wraps a whole bunch of axons individually Provide structural framework can be stained by CNPase |
|
|
What is the down side to myelination and why can you not do it to all axons? |
Takes of a lot of space causing it to be bulkier
|
|
|
What are the Node of Ranvier? |
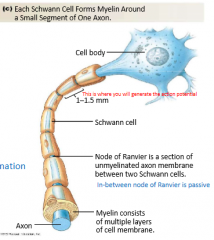
Small gaps left between adjacent glial cells on the axon. They are a section of unmyelinated axon membrane between Schwann/glial cells. It is passive |
|
|
What causes Multiple sclerosis (MS)? |
Loss of myelination causing messages not get transmitted well |
|
|
What are saltatory conduction? |
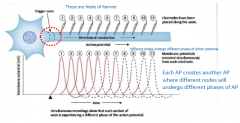
Saltatory conduction is the 'jumping' mode of condution In myelinated axons, only the membrane exposed at the nodes is excitable Because the APs are only generated at these nodes, it means that the AP will 'jump' from one place to the next and in-between, you are not generating any AP Thus, if have an AP on one node, the depolarizing current that is generated at the site is strong enough and will travel down the axon for many nodes (5-10), there is sufficient strength to bring all the following nodes to threshold potential Therefore, AP at one node will bring all the next 5-10 nodes to -50mV to generate APs on all the next nodes simultaneously and passive spread of depolarizing current occurs between the nodes (myelinated portion) Each AP creates another AP where different nodes will undergo different phases of AP You could poison some of the nodes and the depolarizing current will just skip past that and move onto the next healthy patch of membrane As long as one AP fire and reach the last one, it will transmit the message |
|
|
What does the myelin prevent? |
Leakage of current across membrane between nodes |
|
|
What happens if you poison some nodes in an axon? |
Because of saltatory conduction, the depolarizing current will just skip past those nodes and move onto the next healthy patch of the membrane. As long as one action potential fire and reach the last one, it will transmit the message |
|
|
How does myelination improve length constant? |
Depolarizing current spread further down the axon (prevent current leakage) |
|
|
How does increase diameter of an axon increase length constant? |
Depolarization current spread further as the inter-nodal distance is increase proportionately |
|
|
What are unmyelinated axons? |
Axons that have not been myelinated They do not have this extensive wrapping around the outside which means you get lots of current leakage and slows down the conductance velocity Majority of axons are unmyelinated |
|
|
Do unmyelinated axons have insulation? |
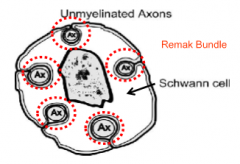
Yes The schwann cells and oligodendrocyte engulf the axon (5-30 axons) without winding to create a "Remak Bundle" |
|
|
What are axon terminals? |
AP will be conducted along the membrane right to the end of the cell where at the end of the cell, AP is still generating depolarizing currents AP cannot turn around and re-propagate in direction it came from because of refractory period, the voltage-gated Na+ channels are inactivated So at the end of the axon (the axon terminal), the AP dies out |
|
|
What are electrical synpases? |
Electrical signal is being transmitted by physical connection and does not require neurotransmitters It is bidirectional An electrotonic synpase (gap junctions) adjacent membranes are about 35A apart Gap junction bridge by connexins which allow small ions (and depolarization) to cross |
|
|
What are chemical synpases? |
The transmitter is released into the extracellular space which exists between adjacent cells The synpase is defined by the presynaptic surface (the bouton which contains the vesicles) and the postsynpatic membrane (which is the membrane of the adjacent neuron) Synpatic cleft (the space) is about 200A wide The synpatic cleft is very specialized due to existence of postsynaptic membrane, which contain specific protein receptors which will bind that transmitter molecule after its released This is all located at the axon terminal where the axons end in 'boutons' filled with vesicles. These vesicles are tiny organelles which contain neurotransmitters which is released into the extracellular fluid |
|

Fill in this chart: |
1) An action potential depolarizes the axon terminal 2) The depolarization opens voltage-gated Ca2+ channels, the Ca2+ enters the cell 3) Calcium entry triggers the exocytosis of synpatic vesicle contents 4) Neurotransmitters diffuse across the synpatic clef and bind with receptors on the postsynaptic cell 5) Neurotransmitters binding initiates a response in the postsynpatic cell |
|
|
How do we get Ca++ ions into the bouton/axon terminal? |
Bouton membrane contains voltage-gated Ca++ channels which open when depolarized by AP current AP depolarizes the bouton membrane and when reaches threshold for opening voltage-gated Ca++ channels at -50mV, Ca++ diffuses into bouton and triggers cascade of reaction which result in vesicle exocytosis |
|
|
What are post synpatic receptors? |
Transmitter agent diffuses across synapses and binds to specific site on a receptor protein embedded in postsynpatic membrane Binding of transmitter causes a change in shape of the receptor protein It does not depend on the transmitter but rather the receptor that binds to the molecule There are two types of receptors: 1) Ionotropic (directly opens channels) 2) Metabotropic (initiates a metabolistic cascade to activate enzymes) |
|
|
What are ionotropic effects? |
Ligand binding opens an ion channel (ionotropic) Binding of the transmitter to the post-synpatic membrane results in the change in the post-synpatic membrane potential, this is called the post-synaptic potential (PSP) The duration of PSP is about 20-40ms Ion channel may be specific for cations (Na+, K+) are EPSP (depolarizing, excitatory) Ion channels that may be specific for Cl- or K+ ion are IPSP (hyperpoloarizing, inhibitory, making more negative) More so immediate effects |
|
|
What are nicotinic receptors for? |
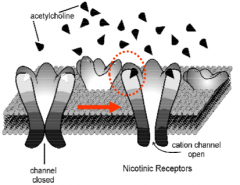
Acetylcholine and nicotine Allows passage of cations in a fast process where it binds and opens |
|
|
What is botox used for? (Biologically, not cosmetically) |
Used to kill of the neurotransmitters which prevent the release of acetylcholine which is the message molecule that is needed to contract |
|
|
What does GABA generally generate? |
An inhibitory neurotransmitter |
|
|
The ligands for the ionotropic receptor are principally: |
Acetylcholine (Ach) Glutamate GABA Glycine |
|
|
What are metabotropic effects? |
Binding of the ligand in the post-synpatic metabotropic receptor activates an enzyme that is usually G-protein coupled The enzyme facilitation will result in increased production or destruction of second messengers Metabotropic receptor activation take take If you influence an ion channel through the metabolic effect, the change in MP will develop slowly Change is slow because of it has to go through all the enzyme activity first before influence the ion channels |
|
|
What are 2nd messengers? |
Are either cAMP, cGMP or InP3 Activates other enzymes like phosphokinases which phosphorylate membrane proteins or other proteins in the cytoplasm If you phosphorylate membrane proteins (like ion channels), you result in moedulation of ion currents |
|
|
What does phosphokinase do? |
Phosphorylate membrane proteins or other proteins in the cytoplasm |
|
|
Why are metabotropic effects slow? |
Because it has to go through all the enzyme activity first before influence the ion channels |
|
|
What is a beta-adrenoreceptor or beta-receptor? |
A beta-receptor is a metabolic receptor for Noradrenalin (NA). Involved in G-protein couple enzymatic pathway Binding of NA to beta-receptor activates adenylyl cyclase via G-protein alteration Adenyl cyclase increases production of cAMP (a second messenger) cAMP then activates kinases which phosphorylate membrane Ca++ channels This phorphorylation of the Ca++ channel causes increase in Cal++ influx (increase contractility in the heart) |
|
|
What are beta-blockers? |
Causes disallowing excessive activity to the heart Can be used to calm someone down |
|
|
Why are Ca++ influx important in the heart?
|
Increase contractility in the heart muscle In the heart, these calcium channels are important because more calcium allow greater and faster contractility |
|
|
What are some ligands for metabotropic receptors? |
ACh Peptides Catecholamines Serotonin Purines Gases |
|
|
Where are PSPs generated? |
In inexcitable membrane such as neuronal dendrites and cells bodies because these areas do not have high density of voltage-gated Na+ channels (they cannot initiate AP) PSP must spread through passive conduction across the membrane to get to the initial segment of the axon to create an AP |
|
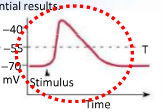
Explain what is going on here where this is in the cell body: |

Thispositive deflection is not an action potential because there are very fewvoltage gated channels but rather this is a graded potential as the sodium isstill coming in making more positive |
|
|
Where is the first place you general an action potential? |
At the trigger zone |
|
|
What is the process of PSP Summation? |
Need lots of EPSP added together to depolarize the trigger zone to -50mV Hoping a conjugation of EPSP will create a combined effect called Summation to have a -50mV by the time it reaches the trigger zone There are two types of Summation: 1) Spatial summation (minimum of 10-30 synchronous EPSP in dendritic tree, each generated at different synapse) 2) Temporal summation (only a few active synapses, but each generating EPSP at high frequency; summated potentials reach threshold over a period of time) |
|
|
What is spatial summation? |
Minimum of 10-30 synchronous EPSP in dendritic tree, each generated at different synapse Large number of EPSPs in synchrony |
|
|
What is temporal summation? |

Only a few active synapses, but each generating EPSP at high frequency; summated potentials reach threshold over a period of time EPSPs last for about 30-40ms in duration before dying out, thus, successive inputs on any given synapse generates subsequent EPSPs that add onto the pre-existing EPSPs You are giving an additive staircase effect by having firing another potential before the one before dies off till it reaches -55mV |
|
|
What are IPSPs? |
Inhibitory Post-Synaptic Potential IPSPs tend to be preferentially located on the cell soma, interposed 1/2 way between the site where EPSP is generated and the trigger zone IPSPs have strategic advantage due to its location close to the trigger zone, it can shunt depolarizing EPSP currents out of the cell |
|
|
How can IPSPs shunt depolarizing EPSP currents? |
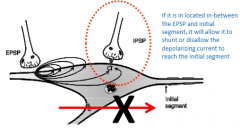
If itis in located in-between the EPSP and initial segment, it will allow it toshunt or disallow the depolarizing current to reach the initial segment |
|
|
Explain the involvement of IPSP in the opening of Cl- channels |
The equilibrium potential for Cl- is very close to the resting MP (-70mV) Therefore at rest, opening of the Cl- channel would result in little change However, when the membrane is depolarized, opening of the Cl- channel will bring the MP back down to -70mV The net affect of Cl- is basically to 'clamp' the MP, which is preventing excitation, thus preventing depolarization of inhibitory effect These IPSPs are very strategically located and they completely block any signal coming from EPSPs simply by positioning right on the soma IPSPsin general in the Nervous System, are more important than EPSPs |
|
|
What happens when you have a very powerful synaptic input to the post-synaptic neuron persisting in time lasting up to 500ms? |
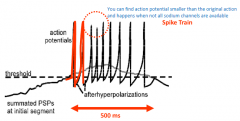
Depolarizing the trigger zone to threshold and sustain that depolarization for 500ms, you want that powerful input to be translated into continuous streams of APs. This is called the 'Spike Train' If we depolarize the membrane above threshold and keep it there, you'll get one AP and the voltage-gated Na+ channels will inactivate (RP) and you cannot get another AP until the membrane repolarizes Therefore, after each 'spike' we need to get the membrane 'hyperpolarized' to restore the Na+ channels to re-open them for the next one Inorder to make a continuous action potential, we are going to have to usepotassium voltage gated channels where it will quickly bring down belowthreshold so it can fire another action potential |
|
|
Explain the after-hyperpolarization of a spike train |
Voltage-gated K+ channels at trigger zone cause after-hyperpolarizations Hyperpolarization after each spike ensures that Na+ channels reconfigure, the membrane excitability is restore After the hyperpolarization fades away (voltage-gated K+ channels will close when the membrane is repolarized), the MP will be able to shoot right back up where EPSP is taking it and cross the threshold again and a whole new spike and this will repeat until the EPSP fades away |
|
|
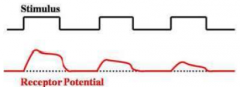
What is receptor potential? |
Change in the MP due to receipt of signal from exterior sensory cue The energy from the environment will react with membrane proteins and in general, this will cause depolarization (exception: photoreceptors hyperpolarize) Similar to PSP, the receptor proteins are embedded in sensory cell membrane The receptor proteins of the sensory cells will change shape when specific energy is received When receptor proteins change shape, it can either: 1) Directly open ion channels 2) Enzyme is activated via G-protein coupling leading to production of 2nd messengers to amplify the signal |
|
|
Explain the process of post-synaptic receptors |
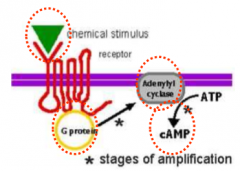
1) Chemical stimulus binds to specific metabotropic receptor (G-protein coupled) 2) Activation of G-protein 3) Activate adjacent enzyme (adenyl cyclase) 4) Produces 2nd messenger (cAMP) 5) cAMP activates kinases which directly interact with ion channels or phosphorylate other proteins |
|
|
What are the two stages of amplification? |
1) G-protein can activate a number of different enzyme molecules 2) Each of these enzyme molecules will produce lots of 2nd messengers (cAMP) |
|
|
What are the two categories of sensory cell transmission |
1) Sensory cell generates an action potential at a spike-generating zone 2) Sensory cell releases vesicles when depolarized; impulses generated in post-synaptic neuron |
|
|
Explain the transmission of a signal by AP |
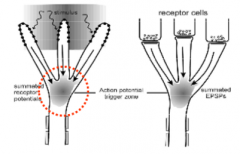
Located at the axon terminal, first patch of excitable membrane will generally be at the branch point, thus, the receptor potential will have to travel and generate summation at a branch point to reach threshold to get an AP |
|
|
Explain the process the olfactory receptor goes through when encountering an odorant |

The depolarizing current has to travel down the membrane and down to the trigger zone of the axion 1) Specific receptor proteins bind specific odorant 2) Activate G-protein 3) Activate adynyl cyclase 4) Production of cAMP 5) cAMP directly binds to ion channels 6) Allow cations (Na+ and Ca++) to go through 7) Depolarization of the membrane |
|
|
Explain transmission of signal by vesicles |
1) Depolarizing current don't produce AP 2) Travel throughout the membrane and at the other end 3) They depolarize the membrane sufficiently 4) Influx of Ca++ ions and trigger exocitosis vesicles 5) Sensory cell is releasing vesicles and not producing an AP |
|
|
In the aspect of MP, what is adaptation? |
MP can decay over time leading to Adaptation The original voltage is sustained and its dropped over time, even though the stimulus may be constant Two types: Slowly and Rapidly |
|
|
What is slow adaptation in the aspect of MP? |
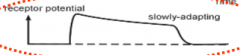
Receptor potential sustained for duration of stimulus Interested in overall magnitude of the stimulus Though it decays, as long as it there, you get a stimulus |
|
|
What is rapid adaptation in the aspect of MP? |
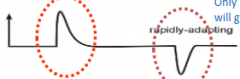
Receptor potential elicited by change in stimulus energy, decays to zero when stimulus is constant Interested in how quickly the stimulus is being delivered, the velocity of stimulus being delivered Only interested in momentary changes and will go to zero if constant stimulus |
|
|
What is habituation in the aspect of MP? |
Habituation is the response to successive stimuli in time Repeated stimuli (identical) in succession elicit progressively weaker responses Habituation responses depend on the cell, some will show large degree and some won't |
|
|
What the two strategies to code for the strength of the stimulus? |
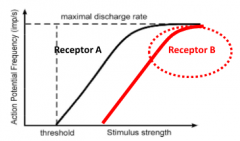
1) Increase frequency of AP at excitable membrane (increase intensity of stimulus = increase frequency of AP on receptor A) 2) With increasing stimulus strength, we recruit an additional receptor B, which has a higher threshold |
|
|
What is population code/coding? |
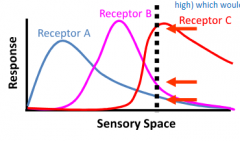
Population coding is coding using the ratio of activity from a restricted number of different receptor types Specific stimulus is coded by ratio of activity across the population of receptors A given receptor (A) type will respond to a wide range, but it has a peak and that is different from others Thus, any given stimulus (dotted line) will activate one receptor (C) very strongly but others (A, B) more weakly |
|
|
What is receptive field? |

Each sensory neuron is going to respond to a particular spatial area called a receptive field
Receptive field of a given sensory neuron is the territory in which you could activate that neuron
Receptive field is always defined in relation to a given sensory neuron, each sensory neuron will have a different receptive field
One sensory neuron may cover a lot of area or just one small area
Receptive field in cutaneous sensory neuron is the skin territory in which adequate stimulation elicits a response and is generally about 10-20mm across
Stimulation in any place in this receptive field will generate receptor potential
Receptive field is not uniform |
|
|
What is axon reflex? |
AP can be initiated at the 'branch point' on one part of the sensory axon terminal to be carried to the CNS However, at the branch point, the AP can travel backwards back to the adjacent terminals by the axon reflex This conduction of AP backwards is known as antidromic conductance (away from CNS) Stimulation of the sensory neuron in the skin will cause antidromic AP to reach the adjacent terminals At the terminal, the pain receptors in skin will release substance P which trigger vasodilation |
|
|
What is orthodromic? |
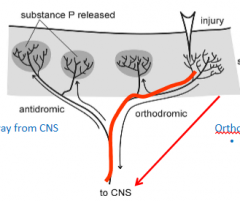
Normal conduction Towards CNS You cannot get backwards because going under absolute refractory period |
|
|
What is the blood-brain barrier? |
The brain and the spinal cord are protected from the general circulation and the body The ionic composition of the extracellular fluid around the neuron must be carefully controlled: 1) Cannot change the excitability of the membrane 2) Cannot have neurotransmitters floating around for no reason Thus, the extracellular fluid in the neuronal environment (brain and spinal cord) are carefully regulated through the Blood-Brain Barrier (BBB) In the brain, endothelial cells are tightly bound leaving no gaps where everything has to be transported |
|
|
What happens when you get a KCl injection? |
1) Decreased K+ concentration gradient 2) Depolarization 3) Inactivation of Na+ channel 4) No more AP produced |
|
|
What causes Parkinson's disease? |
There is a lack of dopamine and problems in the receptor which causes muscle contraction You cannot inject dopamine as it cannot cross the BBB |
|
|
What is dopamine? |
It is a reward neurotransmitter People who lack this become more addicted |
|
|
What areas in the brain are lacking a BBB? |
Hypothalamus where essential for neurons to communicate freely with blood stream Pituitary gland for releasing hormones and is directly connected to the hypothalamus Cicumventiruclar organs (around 3rd ventricle) has a broken BBB so neurons can sense specific chemicals Generally, BBB is broken in areas that interact with endocrine system or require sensitivity to metabolites in plasma |
|
|
What is the brain encased by? |
The skull and the meninges |
|
|
What is the meninges? |
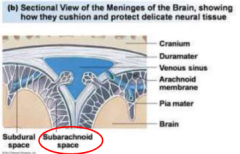
Dura mater (very touch membrane, sac containing the brain and the spinal cord) Arachnoid membrane (much more delicate tissue) Pia mater (lies right on top of the brain; tether to Arachnoid by Arachnoid 'Trabeculae') Between the arachnoid membrane and the Pia matter, Subarachoid space (filled with CSF) brain floats to protect from mechanical stress |
|
|
What is the reticular formation? |
This is an area that connects the brain to the spinal cord The reason why sports players wear mouth guards is not to protect the teeth but rather to prevent the mouth jaw bone to vibrate causes the wearer to lose conscious temporary Key organized of behavioural patterns of the body and consists of a network of cell bodies and interconnected axons Reticular formation projects to centromedian nucleus of thalamus |
|
|
What are fenestrations? |
The endothelial lining of the BV, mostly contain large gaps (called fenestrations) through which molecules can pass |
|
|
What are astrocytes? |
Provide a bridge between neurons and blood vessels
It would pick up nutrients and bring it to the synpases
They have two functions: 1) Remove neurotransmitters 2) Provide energy substrates for neurons and more
They are following and latching onto BV (some end feet latched onto the BC and the others with neurons)
Astrocytes also regulate local blood flow
Provide structural support
Regualte ion, nutrient, and dissolved gas concentrations
Absorb and recycle neurotransmitters
Form scar tissue after injury
Can be stained by GFAP
Found in the CSN
Astrocytes surrounding neurons determine how you breath in and out, how you main autonomic functions |
|
|
How do astrocytes regulate local blood flow? |
Astrocytes are already bridging the gap between BV and neurons, so they are in a good spot to signal BV when to dilate and constrict (increase or decrease blood flow)
Astrocytes have connection with the neuron at the synapse and when they detect increased signaling, they can send a metabolic signal outward to BC (opposite to nutrient flow), signaling neuronal activity level
Glutamate in synapses trigger Ca++ release within astrocytes where Ca++ wave travels through astrocytes and trigger prostagladin (PGE2) release at end foot |
|
|
What is PGE2? |
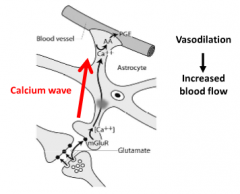
Prostagladin Released by astrocytes Caused vasodilation (increased blood flow) |
|
|
What are ventricles? |

Ventricles are cavities deep inside the brane A large curving Lateral Ventricle (LV) inside each cerebral hemisphere, a paired structure across the midline The LV empties into the 3rd ventricle, right in the middle, deep in the brain under the cerebral hemisphere The 3rd ventricle communicates via a channel called "Aqueduct of Sylvius" to the 4th ventricle From the 4th ventricle, we have a canal, "Central Canal", which goes in the middle of the spinal cord All these ventricles are filled with CSF which is the bathing medium of the brain (highly regulated ionic content, few macromolecules) which eventually drains into the venous system |
|
|
Where is CSF produced? |
From plasma by 'choroid plexus', which lines the ventricles |
|
|
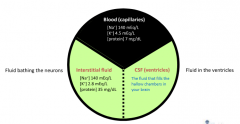
What is CSF? |
Cerebrospinal fluid CSF produced by 'choroid plexus' in ventricles CSF filled ventricles and the subarachnoid space CSF has same osmolarity and [Na+] as blood Greatly reduced [K+], [Ca2+] and [Mg2+] Total volume on an average person is 215mL Most of the CSF is in subarachnoid space, serving as cushion |
|
|
What is adult neurogenesis? |
Production of new neurons into adulthood Memory formed during childhood (brain is still developing and making connections) are permanent (hard-wired, built into structure/motherboard) |
|
|
What did Kuhn et al showed in 1996? |
They showed the first unambiguous evidence for neurogensis in the dentate gyrus using the thymidine analog: bromodeoxyuridine (BrdU) |
|
|
What is the hippocampus? |
Explicit memories (declaritive) and semantic facts Memory for meaning, concepts and facts about the world Episodic events such as memory for events that occur in the context of a specific time, place and circumstance and autobiographical |
|
|
What are the negative regulators of adult neurogenesis? |
Aging Stress (glucocorticoids) Inflammation Methamphetamine/opiates Nitric oxide Interleukin-6 (from activated microglia) Irradiation Antimitotic agents (MAM) |
|
|
What are positive regulators of adult neurogenesis? |
Enriched environment Antidepressants Caloric restrictions Growth factors (BDNF, BEGF, FGF) Pregnancy (prolactin) Electroconvulsive shock therapy Learning Physical activity (running) |
|
|
What is the CNS? |
Central nervous system (the spinal cord and the brain) Protected by bone of skull and vertebrae & BBB Only in certain vertebrae species such as goldfish can they repair the CSN while humans cannot |
|
|
What is the PNS? |
Peripheral nervous system (efferent system)
All the axons and somata not protected by bone, nor by the BBB
Capable of regeneration and repair |
|
|
What are satellite cells? |
Found in the PNS Surround neuron cell bodies in ganglia Regulate O2, CO2, nutrient and neutrotransmitter levels around neurons in ganglia Can be stained using Glutamin Systenase (GS+) |
|
|
What is GS+? |
Glutamin systenase, used to stain satellite cells |
|
|
What are microglia cells? |
Remove cell debris, wastes and pathogens by phagocytosis Stained by CDSS which is an immune marker Found in the CNS |
|
|
What are Ependymal cells? |
Found in the CNS Line ventricles (brain) and central canal (spinal cord) Assist in producing, circulating and monitoring of cerebrospinal fluid |
|
|
What is the axon bundle called in the CNS and PNS? |
CNS: tract PSN: Nerve |
|
|
What is a group of somata called in the CNS and PNS? |
CNS: Nucleus PNS: Ganglion |
|
|
What is a myelin forming glia called in the CNS and PNS? |
CNS: Oligodendrocyte PNS: Schwann cell |
|
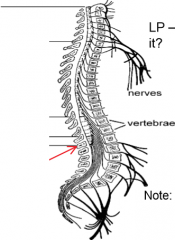
What are the four sections in the spinal cord? Label them: |
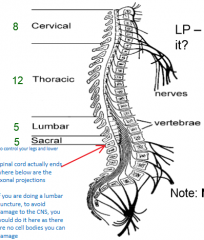
Cervical, thoracic, lumbar and sacral |
|
|
Where does the spin cord actually end? |
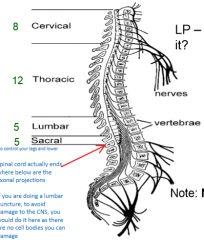
Spinal cord ends below the axonal projections, in the bottom of the lumbar region (red arrow) |
|
|
Where do you puncture if you are doing a lumbar puncture? |
To avoid damaging the CNS, you would do it at the end of the spinal cord where there are no cell bodies you can damage |
|
|
What is the dorsal horn in the spinal cord? |
Where you will get sensory signals/information coming in |
|
|
What happens in the intermediate zone in the spinal cord? |
Some basic processing of sensory information will occur and something analogies will occur in the brain stem
|
|
|
What is the ventral horn in the spinal chord? |
The motor neuron are found in the ventral horn where it contains efferent signals |
|
|
What is the ventral funiculus in the spinal cord? |

Efferent output is usually in the form of a motor neuron (the white circles) which leave through the ventral horn |
|
|
What is white matter in the spinal cord? |
Myelinated and unmyelinated axons Divided into six columns (funiculi) containing tracts: i) Ascending tracts relay information from the spinal cord to the brain ii) Descending tracts carry information from the brain to the spinal cord |
|
|
What is grey matter in the spinal cord? |
Cell bodies, unmyelinated axons and neuroglia (divisions in grey) |
|
|
What are horns in the spinal cord? |
Horns are projections of grey matter toward outer surface of cord |
|
|
What are the corticospinal and rubrospinal? |
They are only excitatory In cervical region bilateral, later ipsilateral and predominantly excitatory. They are responbiel for head stability and antigravity and postural support If you send information from the cortex, you will most likely find it in the lateral region of the spinal cord (the corticospinal tract) |
|
|
What are the reticulospinal and vestibulospinal? |
From brainstem (pons, medulla) reticular formation Project to motor nuclei and intermediate zones on both sides of SC Both inhibitory and excitatory |
|
|
The brain stem is composed of what three parts? |
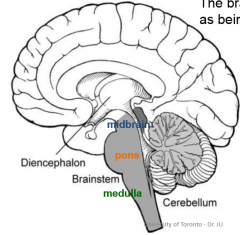
Brainstem (which can subdivide into midbrain, pons and medulla) Cerebral cortex Cerebellum |
|
|
What is the function of the thalamus? |
Relay station (all different nuclei in here act as a relay station between braistem, spinal cord and cortex) |
|
|
What is the function of the hypothalamus? |
Cannot survive without this very long
It flavours/contextual memory
In charge of Homeostatic control
Interface between endocrine and nervous system |
|
|
What is the medulla? |
Connects the brain with the spinal cord and all communication with the cortex goes through this region of the CNS This region contains important relay stations and reflex centers The types of important things in the brianstem are: 1) Autonomic nuclei controlling visceral activity important for survival 2) Sensory and motor nuclei of 5 cranial nerves 3) Relay station for both sensory and motor pathways |
|
|
Explain shifts in the medullary nuclei |
Brainstem is merely a continuation of the spinal cord (SC) Many of the SC structures have analogous structures within the brainstem Analogs of the dorsal horn are the cranial sensory nuclei, these are often very long, continuous sensory nuclei |
|
|
What is hypoglossal N. (cranial nerve XII)? |
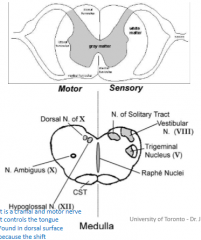
It is a cranial and motor nerve It controls the tongue |
|
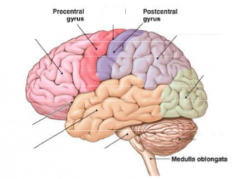
Label the missing parts of the brain |
|
|
|
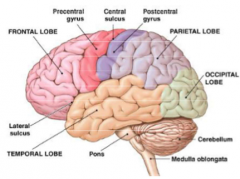
What is the function of the frontal lobe? |
Voluntary motor
It is also involved in discussions making and complex behaviours |
|
|
What is the function of the parietal lobe? |
Touch, pressure, pain perception |
|
|
What is the function of the occipital lobe? |
Conscious visual perception |
|
|
What is the function of the temporal lobe? |
Conscious auditory and olfactory perception |
|
|
What is the function of the central sulcus? |
Differentiate from frontal and parietal lobe |
|
|
What is the function of the lateral sulcus? |
Differentiate from frontal and temporal lobe |
|
|
Explain the cellular cortical organization: |
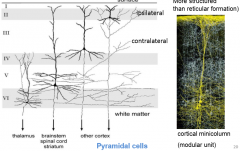
Each layer has a different function in the cellular cortical organization Cells in region 4 are called the large pyramidal cells - Their shape is typically triangular - They are typically large and going out to other regions of the cortex The cells in layer 5 send out to brainstem and spinal cord and striatum Cells in layer 6 goes out to the thalamus and other diencephalon area |
|
|
What are cortical mini-columns |

Concept of common receptive fields and functional groupings of neurons One thalamic axon can innervate many of these mini-columns |
|
|
What does the cerebrum consist of? |
Cortex (grey and white where brain sends white matter down to grey) Nuclei (basal ganglia) |
|
|
What does the basal ganglia consist of? |
Caudata putamen Globus pallidus Amygdala |
|
|
What function is involved with the amygdala? |
Fear |
|
|
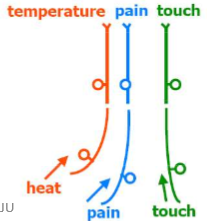
What is Muller's law of specificity? |
Sensory receptors can be divided into five major categories: 1) Chemoreceptors 2) Photoreceptors 3) Nociceptors 4) thermoreceptors 5) Mechanoreceptors These all respond, as expected to very specific type of stimulus Muller's law states that sensory perception is defined by which sensory pathway is being stimulated |
|
|
What is sensory transduction?
|
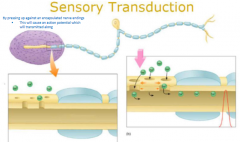
Once a stimulus activates a sensory receptor, that must be converted into a signal that can be recognized by the nervous system
Example) by pressing up against an encapsulated nerve ending, this will cause an AP which will be transmitted along |
|
|
What is stimulus encoding? |
Once the stimulus has been encoded into an electrical signal, it can encode for different properties (duration, intensity, and location)
There is often some overlap at discriminating sensory modalities
Each receptor type is most sensitive to a particular type of stimulus. The brain thus associates a signal coming from a specific group of receptors with a specific modality
This direct association between a receptor and sensation is called the labeled line coding
Patch of skin is innervated by many different types of nerve endings.
Sensory neurons project in both directions (to skin and send afferents to the brain)
Sensory signals from the skin have the property of decuassation |
|
|
What is decuassation? |
Some signals go from one side of body to another, some cross over while decussationis the crossing over of signals |
|
|
Explain the dorsal root ganglia in sensation |

T-Junction division of pseudo-unipolar ganglion cell neuron Cation channels that are found at the receptor end (in the skin for example) that allow for production of a generator potential If the generator potential produces enough of a depolarization, it will open voltage-dependent Na+ channels and allow action potentials to be propagated along the axon It will become electrically active and if it reaches the axon, it will regenerate an action potential The signal will go through to dorsal region to activate this specific spinal cord |
|
|
What are mechanoreceptors? |

Somatosensory receptors are a class of mechanoreceptors There are two broad cateogires: 1) Cutaneous receptors (on skin which detects pressure and stress) 2) Proprioceptors (which detect forces in muscles and joints and tendon) Some receptor endings are free and some are encapsulated |
|
|
What is the A(alpha)-(beta) cutaneous receptor? |
Large diameter Myelinated Only mechanoreceptive (50m/s) Typically encapsulated receptor |
|
|
What is A(delta) cutaneous receptor? |
Small diameter
Myelinated; mechano-,thermo, and nociceptors (10m/s)
Typically the receptor is a "naked" (just under epidermal lining) or free nerve ending |
|
|
What is the C cutaneous receptor? |
Small dimater Unmyelinated (1m/s), mechano-, thermo- and nociceptor Transmit at an extremely slow rate |
|
|
What is the pacinian corpuscle? |
Largest cutaneous receptor (A alpha) (transmits information extremely fast) Huge receptive field. One is enough to innovate a huge region of your palm of your hand Located deep in dermal layers; hands, feet Rapidly-adapting; responds best to skin vibration at 200Hz Very sensitive (threshold of about 0.5um) The pancinian coruscles do not enter the S1 because their receptive fields are too large |
|
|
What are Merkel disks? |
They are encapsulated by one large disk This receptor type is slowly adaptive. Threshold response to skin indentations of 20 microns Stimulation of axon gives sensation of leaf pressing against RF Move innervation of the fingertips Greater spatial acuity in smaller fingers; higher density of Markel cells and smaller RF of afferent Women generally have smaller fingertips than men, hence they perceive finer surface detail |
|
|
What are thermoreceptors? |
Generally slowly adapting Typically free or bare nerve endings Warm (group C) which respond to skin temperatures from 25-45C, anything above 45 you would feel pain Cool (group A delta) responds to skin temperatures from 10-28C, anything below 10C you would activate polymorphic sensory and stimulate pain Receptor proteins are 'TRP' cation channels (transient receptor potential) - non-selective allowing Na+/Ca++ influx As soon as you stimulate these, there would be a burst of phasic activity then goes into rhythmic activity of adaptation |
|
|
What are nociceptors? |
The "pain" receptors in your skin Group A(delta): cool thermoreceptors • high-threshold mechano-receptor • 'pricking' pain Group C: (un-myelinated - only ones) warm 1)Polymodal nociceptors • respond to tissue injury • 'burning' pain • very slow speed at 1m/s 2) 'Sleeping' nociceptors • mechano-insensitive • no response what so ever to mechanical response • Some respond to histamine to mediate itch |
|
|
What gets activated when you have tissue damage? |
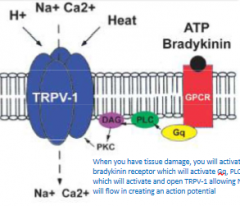
When you have tissue damage, you will activate a bradykinin receptor which willactivate Gq, PLC and DAC which will activate and open TRPV-1 allowing Na and Ca will flow in creating an action potential |
|
|
What are mechano-heat nociception? |
A(delta) and C-fibre nociceptors A(delta) nociceptors respond to noxious mechanical stimuli and cold (below freezing) Polymodal C-fibre nociceptors comprise half of all C-type Respond to mechanical injury, cold and noxious heat |
|
|
What are proprioceptors? |
Receptors located in muscles, tendons and joints (not skin) This system lets you stand up, know where your joints are in space Includes muscle spindle, golgi tendon organ, and joint receptors |
|
|
What are muscle spindal?
|
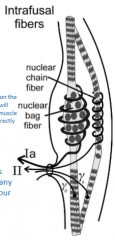
Adequate stimulus is passive stretch (group 1a afferents)
Consist of specialized 'intrafusal' muscle fiber serving as a sensory organ
Central zone, containing nuclei, wrapped by group 1a sensory axon
Largest diameter, fastest-conducting sensory axon
Slowly-adapting
Stretch of the intrafusal fibres excites spind;e afferents
If you pull on the muscle, it will stimualte muscle spindles directly |
|
|
What is golgi tendon organ? |
Adequate stimulus is active force (group 1b afferents) |
|
|
What is joint receptors? |
Detect orthogonal (paciniform) or tangential (Ruffini receptors) force in joint capsule (group II) |
|
|
What is group 1 proprioceptor? |
Large diameter, myelinated 1a (muscle spindle) has speed up to 75m/s in humans (fastest nervous system response) 1b (golgi tendon organ) |
|
|
What is group 2 proprioceptor? |
Medium diameter, myelinated Joint afferents, muscle spindles |
|
|
What is group 3 proprioceptor?
|
Small diameter, myelinated |
|
|
What is group 4 proprioceptor? |
Small diameter, unmyelinated |
|
|
What happens when you put an unknown weight on an muscle? |
Because it is an unknown weight, the muscle would stretch causing a pulled and applied stretch which sends a stretch signal back to get a stretch response
When this happens, the muscle contracts back causing the muscle to become shorter
Re-sensitization through the gamma fibre causing it to be pulled tight causing the interfusal fibre to also contract |
|
|
What happens when a muscle is stretched? |
When a muscle is stretched, primary sensory fibers (1a) of the muscle spindle responds to both the velocity and the degree of stretch Sensory information sent to spinal cord Secondary sensory fibers (II) detect and send information about the degree of stretch (but not the velocity) |
|
|
What are joint receptors? |
Attach to capsule enveloping the joint that can help tell where your muscle/joints are in space
Group 2 and 3 sensory axons
Golgi-Mazzoni corpuscles (paciniform) respond to orthgonal forces (compression)
Ruffini endings respond to capsule strain (i.e. bending of the joint or of muscle pulling on the joint to determine if being put under heavier stress) |
|
|
What are the three pathways to the brain? |
Dorsal columns/medial leminscus, spinothalamic tract, spinoreticulothalamic |
|
|
What is the dorsal column/medial leminscus? |
Fast and solely mechanoreceptive
Small RF (PC exception which has large RF) |
|
|
What is the spinothalamic tract? |
Many modalities, 'wide dynamic range' neurons; polymodal Pain-, itch-, temperature- and some touch-specific neurons (affective sensations) The lateral spinothalamic tract transmit pain and temperature The anterior spinothalamic tract (or ventral spinothalamic tract) transmit light touch and pressure |
|
|
What is the spinoreticulothalamic? |
Slowest, mixed modalities (many synapses)
Pain-related neurons |
|
|
What is the dorsal (posterior) columns? |

Conveys only mechano-receptive information Groups 1, 2 and A(alpha)-beta Want to preserve as much information as possible in these large diameter afferents Somatotopic organization Segregation of cutaneous (superficial) and proprioceptive (deep) afferents Separation of slowly and rapidly adapting afferents |
|
|
What is the S1 (3B) area of the somatasensory coretx? |

Highly segregated information (spatial and modality)
S1 or area 3 is divided into 2 parts: 3a) Proprioceptive map of the body 3b) Cutaneous map of the body
ON and OFF response to stimulation of receptive field
In order for your to differentiate different mechanical touches, you need an area 3B somatosensory cortex where the information will be sent to different places in the cortex
It has topographic organization. "Somatatopic" representation of the skin surface in area 3b where large foci (areas) devoted to the most densely innervated regions (some areas more sensitive to others)
It also has hypercolumn organization: Functional unit of the cerebral cortex particularly when dealing with somatosensory information. It is a block of cortex containing all the neurons responsive to the same point on the skin. Hypercolumns are arranged mainly in somatotopic order |
|
|
What is area 3b topographic organization? |
"Somatatopic" representation of the skin surface in area 3b where large foci (areas) devoted to the most densely innervated regions (some areas more sensitive to others) |
|
|
What is area 3b hypercolumn organization? |
Functional unit of the cerebral cortex particularly when dealing with somatosensory information. It is a block of cortex containing all the neurons responsive to the same point on the skin. Hypercolumns are arranged mainly in somatotopic order |
|
|
What is area 2 and 5 of the brain? |
The postural neuron Neurons respond to postural configurations of limbs or to specific vectors of limb motion Representation of 'body image' Common theme where surrounding cortical areas process information and have complex behaviours |
|
|
What are the two different ways to the thalamus? |
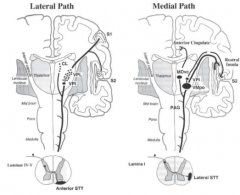
Synapses in either lamina 1 of the dorsal horn or in deep layers of the dorsal horn (layer V) Lamina 1 contains projection neurons specific for pain, itch and temperature Pain neurons project in a distinct tract via contralateral cord to thalamus Medial Path/C fibres, lateral STT vs C/A(delta)/A(beta) fibres use Anterior STT tract Deep STT neurons are commonly "wide dynamic range" neurons |
|
|
What are wide dynamic range neurons? |
Respond to both light and intense stimuli Common type of spinothalamic neuron Convergent inputs from low threshold mechanoreceptors (direct stimulation) and high threshold nociceptors (via interneurons) RF for light touch is much smaller than RF for noxious stimuli |
|
|
What is referred pain? |
Is the result of an artifact of convergence of visceral nociceptors onto spinothalamic (and spinoreticulothalamic) neurons Some projection neuron receives nociceptor input from several body loci Brain interprets signal as coming from locus which is most often injured When your kidney is in pain, you feel pain in another patch of skin. This referred pain is due to convergence of nociceptive fibers onto a single ascending tract |
|
|
What is mechanical gating/control of pain? |
Large mechanoreceptor afferents presynaptically inhibit small nociceptor afferents
Inhibitory interneurons located in substantia gelatinosa (SG) of doral horn
Mechanism of massage therapy
As you mechanical stimulate what you are damaged, you activated A(beta) and send that new signal in and turn off the pain signal a bit. |
|
|
What is the lacrimal gland? |
In the orbit above the lateral end of the eye
It secrets tears |
|
|
What is the lacrimal secretion? |
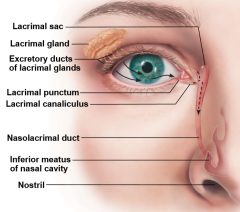
Tears Dilute saline solution containing mucus, antibodies, and lysozyme (protects against bacterial infections) Blinking spreads tears towards medial commissure (tears form on lateral ends of eyes) Tears enter paired lacrimal cancliculi via lacrimal puncta then drain into lacrimal sac and nasolacrimal duct |
|
|
Where is the visual process occurs? |
Approximately half of it is processed by the cerebral cortex |
|
|
Explain the concept of extrinsic eye muscles? |
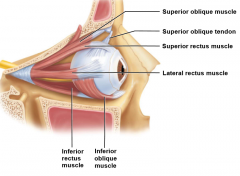
Six straplike extrinsic eye muscles which originate from body orbit (insert on eyeball) and enable eye to following moving objects (maintain shape of eyeball and hold in orbit) Four rectus muscles originate from common tendinous rings; names indicate movement: - Superior, inferior, lateral, medial rectus muscle Two oblique muscles move eye into vertical plane and rotate eyeball (in order to see things in 3D): - Superior and inferior oblique muscles |
|
|
What does the lateral recuts muscle control? |
Moves eye laterally Controlled by cranial nerve VI (abducens) |
|
|
What does the medial rectus muscle control?
|
Moves eyes medially Controlled by cranial nerve III (oculomotor) |
|
|
What does superior rectus muscle control?
|
Elevates eye and turns it medially Controlled by cranial nerve III (oculomotor) |
|
|
What does the inferior rectus muscle control? |
Depresses eye and turns it medially
Controlled by cranial nerve III (oculomotor) |
|
|
What does the inferior oblique muscle control?
|
Elevates eye and turns it laterally Controlled by cranial nerve III (oculomotor) |
|
|
What does superior oblique muscle control? |
Depresses eye and turns it laterally
Controlled by cranial nerve IV (trochlear) |
|
|
In the structure of the eyeball, the internal cavity filled with fluids is called the: |
Humors |
|
|
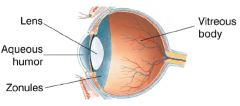
Explain the lens in the eyeball |
The lens is a transparent disk that focuses light. It is suspended by ligaments called zonules. In front of the lens is the anterior chamber, filled with aqueous humor, a low-protein plasma-like fluid. Behind the lens is the vitreous chamber, filled mostly with vitreous body, a clear gelatinous matrix that helps maintain the shape of the eyeball Biconvex, transparent, flexible and avascular It has two regions: lens epithelium (anteriorly) and lens fibers (form bulk of lens) Lens become more dense, convex, less elastic with age causing cataracts Its shape can alter the refraction of light |
|
|
In the eyeball, what is the fibrous layer? |
Outermost layer; dense avascular (not a lot of blood vessels) connective tissue Two regions: sclera and cornea |
|
|
What is the sclera in the eyeball? |
The white part of the eye Part of the fibrous layer Opaque posterior region (connective tissue) Protects, shapes eyeball; anchors extrinsic eye muscles Continuous with dura mater of brain posteriorly |
|
|
What is the cornea in the eyeball? |
Part of the fibrous layer Transparent anterior 1/6 of fibrous layer Bends light as it enters eye Na pumps of corneal endothelium on inner face help maintain clarity of cornea Numerous pain receptors contribute to blinking and tearing reflex Is a transparent, dome-shaped bulge at front of eye, continuous with the white of the eye (sclera) The cornea and lens focus light on the retina, the inner lining of the eye that contains photoreceptors |
|
|
What is the vascular layer (uvea)? |
It is the middle pigmented layer of the eye (non clear/transparent)
Has three regions: choroid, ciliary body and iris |
|
|
What is the choroid region in the eyeball? |
Part of the vascular layer Posterior portion of the uvea Supplies blood to all layers of the eyeball Brown pigment absorb light to prevent light scattering and visual confusion |
|
|
What is the ciliary body in the eyeball? |
Part of the vascular layer Ring of tissue surrounding lens Smooth muscle bundles (ciliary muscles) control lens shape Capillaries of ciliary processes secret fluid (not the same fluid as what produce tears) Ciliary zonule (suspensory ligaments) holds lens in position |
|
|
What is the iris in the eyeball? |
Part of the vascular layer Coloured part of the eye Pupil is the central opening (diameter) that regulates amount of light entering the eye Close vision and bright light (circular muscles contract; pupils constrict Distant vision and dim light - dilator pupillae (radial muscles) contract; pupils dilate using sympathetic fibres Changes in emotional state, pupils dilate when subject matter is appealing or requires problem-solving skills |
|
|
What is the outer pigmented layer in the eyeball? |
Single cell thick lining Absorbs light and prevents it scattering Phagocytize photoreceptor cell fragments Stores vitamin A |
|
|
What is the inner neural layer in the eyeball? |
Transparent Composed of three main types of neurons: photoreceptors, bipolar cells, and ganglion cells Signals spread from photoreceptors to bipolar cells to ganglion cells Ganglion cells axons exit eye as optic nerve |
|
|
What is the optic disc in the retina?
|
The blind spot
Site where optic nerve leaves eye Don't have a lot of photoreceptors here |
|
|
How does blood supply get to the retina? |
Two sources: Choroid supplies outer third (photoreceptors) Central artery and vein of retina supply inner two-thirds which enter/exit eye in center of optic nerve and vessels visible in living person |
|
|
What is the macula lutea? |
This region has the highest concentration and density hat is responsible for visual acuity |
|
|
What does the posterior segment of the internal chamber contain? |
Viterous humor has multiple functions such as transmitting light, support posterior surface of lens (give shape to eye), hold neural layer of retina firmly against pigmented layer, contributes to intraocular pressure, forms in embryo (last lifetime) |
|
|
What does the anterior segment of the internal chamber composed of and contains? |
Two chambers: Anterior chamber between cornea and iris Posterior chamber between iris and lens It contain aqueous humor which is a plasma like fluid continuously formed by capillaries of ciliary processes (found inside the eye and inside the chamber), drains via scleral venous sinus (canal of Schlemm) at sclera-cornea junction, supplies nutrients and oxygen mainly to lens and cornea but also to retina and removes wastes |
|
|
What is glaucoma? |
Blocked drainage of aqueous humor increases pressure and causes compression of retina and optic nerve which leads to blindness
The optic nerve is part of the CNS which you cannot regrow
It is usually associated with increase intraocular pressure, sometimes caused by excess aqueous humor
Treatment may involve drugs to inhibit production of aqueous humour, or surgery to reopen the canal of Schlemm
Optic nerve damage in glaucoma may involve nitric oxide or apoptosis-inducing factors |
|
|
What is lens fibers? |
Form bulk of the lens Filled with transparent protein crystalling |
|
|
What is cataracts? |
Clouding of lens
Consequences of aging, diabetes mellitus, heavy smoking, frequent exposure to intense sunlight
Can be genetic
Has crystallin proteins clump.
Some evidence to suggest that vitamin C increases cataract formation
Lens can be replaced surgically with artificial lens |
|
|
Explains what happens when light passes through the pupil: |
The pupil shrinks and dilates with the contraction and relaxation of a ring of smooth pupillary muscles, so it can affect the amount of light that reaches the retina In bright sunlight, the pupil shrinks to 1.5mm across as parasympathetic signals constrict the pupillary muscles In the dark, the pupils dilate to 8mm as sympathetic signals contract radial muscles orthogonal to the pupillaries |
|
|
Explain the pupillary/consensual reflex |

The examiner shines a light into one eye Signals travel along the eye's optic nerve (cranial nerve 2) to the thalamus, then to the midbrain From there, signals travel along parasympathetic fibers of cranial nerve 3 to constrict the pupils of both eyes |
|
|
How does the pupil control depth of field? |
When the pupil is tightly constricted, then we have full depth of field When the pupil is dilated, then we have a shallow depth of field That distance to one specific object of vision is called the focal length and depends on the shape of the lens |
|
|
What happens if the lens is too flattened? |
Lens doesn't bend the rays enough to bring them to a focus on retina, retinal image will be fuzzy Can be brought into focus by make lens rounder |
|
|
What is accommodation in the sense of lens? |
The fattening of the lens for near vision Weakens with age (called presbyopia) It is an unconscious reflex |
|
|
What are ciliary muscles? |
Smooth muscle that control the lens shape When the ciliary muscle is relax, the ring is wide and the tension of the zonules pulls the lens flat When the ciliary muscles contract, the ring is tighter so tension decreases and the lens round |
|
|
What is hyperopia? |
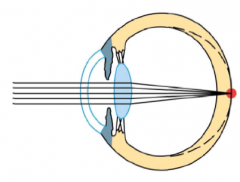
Far-sightedness The focal point falls behind the retina Fixed with a convex lens |
|
|
What is myopia? |
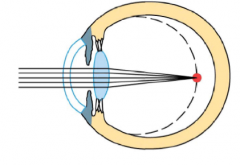
Near-sightedness Focal point falls in front of the retina Eyeball is elongated Fixed with a concave lens |
|
|
How does your brain see images? |
Images are actually seen inverted so your brain flips the inverted image |
|
|
What light wavelengths can human see? |
Visible light of 400-700nm and cannot see outside of it |
|
|
What is phototransduction? |
Conversion of light energy into electrical energy
In humans, phototransduction occurs in the retina, in light-sensitive neurons called photoreceptors
The photoreceptors are most densely packed in an area of retina called the macula which is an area specialized for high-acuity vision |
|
|
What is the fovea? |
The inner part of the macula |
|
|
Where do the photorceptors lie in the retina? |
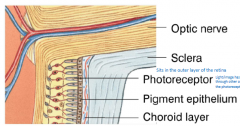
The outer layer
Therefore, the other neurons and their axons lie between the photoreceptors and the light, but these inner layers are mainly transparent
Melanin in the pigment epithelium absorbs any light ray that escape the photoreceptors so it prevents reflected rays corrupting the retinal image. The choroid layer contains blood vessel |
|
|
What are photoreceptor cones? |
High-acuity and colour vision in bright light They are densely packed in the fovea, a pit in the center of the macula that contains only cones and no other cells to block the light Three types of cones prefer different wavelengths for red, green and blue light The brain deduces colours from activities of the 3 types |
|
|
What are photoreceptor rods? |
More sensitive, so they function in low light
Outnumber cones 20:1
In dark light, you are using your rods but they cannot discriminate colour but because they are more sensitive, they outnumber cones |
|
|
What is the basic structure of rods and cones for photorecptors? |
In an outer segment, the membrane folds into disk-like layers (in rods, the outermost disk are detached from the cell). The disks contain visual pigments that transduce light into changes in membrane potential In an inner segment are the nucleus and organelles for ATP and protein synthesis; and in a basal layer, a synapse that release glutamate |
|
|
What is rhodopsin and the process associated with it? |
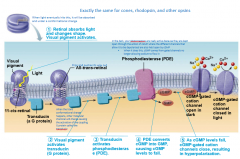
Rods have one kind of visual pigment, rhodopsin, composed of 2 molecules: 1) Opsin: a protein in the membrane 2) Retinal: vitamin-A derivative that is light-absorbing part In darkness, retinal binds opsin. A single photon can make retinal change shape and release its opsin (in a process called bleaching which alters MP) The process associated with it goes: 1) Retinal absorbs light and changes shape. Visual pigment activates. Changing from 11-cis retinal to all-trans retinal. 2) Visual pigment activates transducin 3) Transducin activates phosphodiesterase (PDE) 4) PDE converts cGMP into GMP causing cGMP levels to fall 5) As cGMP levels fall, cGMP-gated cation channels close, resulting in hyperpolarization In darkness, cGMP levels are high in the rod cytosol. K+ and cyclic-nucleotide-gated (CNG) channels are open and the rod is slightly depolarized to -40mV As a result, Ca++ channels are open in the synaptic terminal and so glutamate is released onto bipolar cells |
|
|
Why do humans have 3 different types of opsins? |
As certain types of fruits that are high with carbohydrates that can spend on our brain, they change colour so if we can see that, that would be an advantage |
|
|
What is PDE? |
Phosphodiesterase Convets cGMP into GMP |
|
|
What happens when [cGMP] concentration falls in photoreceptors? |
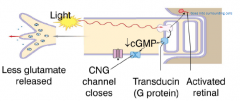
CNG channels close, slowling or stopping the influx of cations K+ efflux continues so the membrane potential falls to -70mV and less glutamate is released Activated retinal difffuses out of the rod and is transported into pigment epithelium In the recovery phase, retinal recombines with opsin. Retinal reverts to its inactive form in the pigment epithelium, then returns to the rods and recombines with opsin to make inactive rhodopsin. |
|
|
What is nyctalopia? |
Night blindness Rod degeneration Commonly caused by vitamin A deficiency If administered early, vitamin A supplements restore function Can be caused by retinitis pigmentosa |
|
|
What is retinitis pigmentosa? |
Degenerative retinal diseases that destroy rods |
|
|
True or false: Photoreceptors and bipolar cells only generate grades potentials (EPSPs and IPSPs) |
True
When light hyperpolarizes photoreceptor cells, it stops releasing inhibitory neurotransmitter glutamate, bipolar cells depolarize and release neurotransmitter onto ganglion cells and genglion cells generate AP transmitted in optic nerve to brain |
|
|
How does light turn into an AP? |

1) cGMP-gated channels close, so cation influx stops. Photoreceptor hyperpolarizes 2) Voltage-gated Ca++ channels close in synpatic terminals 3) No neurotransmitter is released 4) Lack of IPSPs in bipolar cell results in depolarization 5) Depolarization opens voltage-gated Ca++ channels; neurotransmitter is released 6) EPSPs occur in ganglion cell 7) Action potentials propagate along the optic nerve |
|
|
What are amarcine cells? |
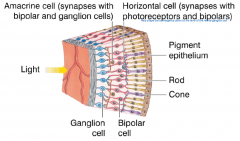
Synapses with bipolar and ganglion cells |
|
|
What are horizontal cells? |
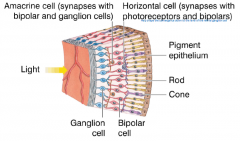
Synapses with photoreceptors and bipolars Help shape the convergence down to the level of the retinal ganglion cell |
|
|
What are the two types of bipolar cells? |
ON (or light-on): Bipolar cells have a metabotropic glutamate receptor, mGluR6, that hypoerpolarizes the cell when it binds glutamate. So these cells are active in light, when less glutamate is secreted by photoreceptors OFF (or light-off): Bipolar cells have an ionotropic glutamate receptor that depolarizes the cell when it binds glutamate. So these cells are active in darkness |
|
|
What are visual fields? |
Receptive fields of ganglion cells and other visual neurons Ganglion cells near the fovea have small receptive fields because only a few photoreceptors project to these cells, and so our visual acuity is high in this region Ganglion cells in the periphery of the retina have large receptive fields, because they receive input from many photoreceptors, so our acuity is low there |
|
|
What is an on-center/off-surround ganglion cell? |
Excited by light falling on the center of its receptive field Is inhibited by light falling in its surround |
|
|
What is an off-center/on-surround ganglion cell? |
Inhibited by light falling on its center Excited by light on its surround |
|
|
What are magnocellular ganglion cells? |
AKA M cells. Large Provide information that is used by the brain to infer the movement of objects |
|
|
What are parvocellular ganglion cells? |
AKA P cells Small Provide information that is used to infer form and fine detail, such as texture |
|
|
What are melanopsin ganglion cells? |
May act as photoreceptors Involved in detecting circadian rhymes Contain an opsin-like pigment called melanopsin Their axons project to the suprachiasmatic nucleus, which is the brain center of circadian rhythms and to other visual areas |
|
|
What is the binocular zone in vision? |
Region seen by both eyes The 2 eyes provide 2 slightly different views of objects in this zones Projects to the pretectal nuclei and the suprachiasmatic nucleus of the hypothelamus |
|
|
Where do the preganglionicneurons of the sympathetic nervous system emerge from the spinal cord? |
Thoracic and lumbar regions |
|
|
In response to stepping on a nail, the crossed-extensor reflex causes: |
Extension of the leg opposite the side of receptor activation |
|
|
Which of the following is NOT a function of the hypothalamus? A. Contains the cardiovascular control centers B. Controls thermoregulation C. Communication between the nervous and endocrine system D. Controls hunger and thirst |
A. Contains the cardiovascular control centers |
|
|
The division of theautonomic nervous system that prepares the body for intense levels of activityand stress is the ____________. |
Sympathetic division |
|
|
Sweat glands contain: A. Beta receptors B. Cholinergic receptors C. Alpha receptors D. All of the answers are correct |
Cholinergic receptors |
|
|
The structure whose abnormal function is associated with Parkinson's disease is the: |
Basal nuclei |
|
|
Golgi tendon organs monitor __________ of skeletal muscles. |
Contraction and stretch |
|
|
Identify the positive regulator of adult neurogenesis A) running B) aging C) Methamphetamine D) stress |
A) running |
|
|
Ramsay Bolton is a ruthless graduate student who enjoys examining the mechanisms underlying pain.If he wants to increase the levels of pain perception following a burn to the hand where tissue is damaged,what would be the most effective? |
Decrease the breakdown of ATP in damaged tissues |
|
|
Jorah believes he has isolated the thalamic ventrocaudal nucleus. Assuming that he has correctlyidentified this structure, which one of the following would he most likely observe in this area? A) Slow and rapid nociceptive information B) Polymodal inputs from wide-dynamic range neuron axons C) Mechanoreceptive and proprioceptive information D) Inputs from small diameter, unmyelinated axons |
C) Mechanoreceptive and proprioceptive information |
|
|
Identify the correct statement regarding adaptation A) Rapidly-adapting receptors are interested in overall magnitude of the stimulus B) Rapidly-adapting receptor potential decays to zero when stimulus is constant C) Slowly-adapting receptors are interested in how quickly the stimulus is being delivered D) Slowly-adapting receptor potential is never sustained for duration of stimulus |
B) Rapidly-adapting receptor potential decays to zero when stimulus is constant |
|
|
Don Draper has damaged the melanopsin containing ganglion cells in his retina. Which of thefollowing would be affected the most as a result? A) Loss of movement discrimination B) Loss of depth perception C) Loss of pupillary reflexes D) Loss of texture discrimination |
C) Loss of pupillary reflexes |
|
|
Alayne accidently creates a virus that selectively destroys all cell types that express high levels of glutamine synthetase (GS). If she infects the nervous system of a mouse with this virus, what would she most likely expect to observe?
A) Decreased resting membrane potentials in rod photoreceptors
B) Decreased myelination in the central nervous system
C) Decreased myelination in the peripheral nervous system
D) Decreased regulation of neurotransmitter levels in ganglia |
D) Decreased regulation of neurotransmitter levels in ganglia |
|
|
Ken Cosgrove has found that a substance is capable of specifically inactivating mGluR6 receptors byblocking glutamate binding on these receptors. If he applies this drug to the retina, which of the followingwould he most likely observe if he performs this experiment under lighted conditions (i.e. in the light)? A) OFF bipolar cells would become more active after drug application B) ON bipolar cells would become less active after drug application C) OFF bipolar cells would become less active after drug application D) ON bipolar cells would become more active after drug application |
D) ON bipolar cells would become more active after drug application |
|
|
Neurotransmitter release occurs by what mechanism? A) exocytosis B) secondary active transport C) primary active transport D) diffusion |
A) exocytosis |
|
|
Identify the incorrect statement regarding membrane transport A) Movement of one substance down its concentration gradient powers the transport of another down itsconcentration gradient B) Permeability depends on molecular size, lipid solubility, and charge C) Sequential binding of a substrate and ions to specific sites in the transporter protein induces aconformational change in the protein D) Carrier protein aid the movement of polar molecules across cell membrane |
A) Movement of one substance down its concentration gradient powers the transport of another down its concentration gradient |
|
|
Myrcella is taking a course in physiology but unfortunately is confused by the concept of rapid adaptation in the somatosensory system. Based on your expertise, which one of the following would you explain to Myrcella does NOT exhibit rapid adaptation?
A) Pacinian corpuscle
B) Merkel disk
C) Cool thermoreceptor at 20°C
D) Meissner’s corpuscle |
B) Merkel disk |
|
|
Theon has been carrying a heavy load for most of the day and his back is painful. If he asks someone to massage his back which one of the following would you expect to occur?
A) Decreased activation of neurons in the spinoreticulothalamic tract
B) Activation of inhibitory interneurons in the dorsal horn
C) Increased activation of PKC epsilon in the wide dynamic range neurons
D) Decreased firing of Adelta nociceptors |
B) Activation of inhibitory interneurons in the dorsal horn |
|
|
Identify the incorrect statement regarding the post synaptic receptors A) If you influence an ion channel through the metabolic effect, the change in membrane potential willdevelop slowly B) Binding of the ligand to the post-synaptic metabotropic receptor activates an enzyme that is usually Gproteincoupled C) Acetylcholine may bind to either the ionotropic or metabotropic receptors D) Binding of ligand may open ion channels which may be specific for cations resulting inhyperpolarization |
D) Binding of ligand may open ion channels which may be specific for cations resulting in hyperpolarization |
|
|
Daenerys decides to reward a student’s performance on a challenge by giving them a thick and heavybook on physiology (is there any other kind?). If the book is heavy enough to passively stretch thestudent’s biceps muscle but he does not drop the book, which one of the following would most likelyoccur? A) Rapid adaptation during stretch of the muscle B) Stretch of the gamma motoneuron fibre C) Activation of the Golgi Tendon Organ in the muscle D) Stimulation of group 1a afferents in the muscle |
D) Stimulation of group 1a afferents in the muscle |
|
|
What determines the strength of a graded potential? A) the amount of voltage-gated channels in the neuron B) the size of the stimulus C) the diameter of the axon D) the amount of leak channels open in the neuron |
B) the size of the stimulus |
|
|
Ted has developed a new chemical inhibitor of the enzyme phosphodiesterase. If he applies this drug to photoreceptors in the eye when there is no light present (i.e. in the dark), what would he most likely expect to observe in these photoreceptors if only this enzyme is affected?
A) Increased release of glutamate
B) Increased K+ efflux
C) Increased formation of 11-trans retinal
D) Increased activation of transducin |
A) Increased release of glutamate |
|
|
Which of the following potentials can sum? A) graded potentials B) threshold potentials C) both graded potentials and action potentials D) neither graded potentials nor action potentials |
A) graded potentials |
|
|
Where in the axon does passive spread of current occur? A) only at the axon terminal B) myelinated portion C) passive spread of current does not occur in axons D) nodes of ranvier |
B) myelinated portion |
|
|
Pete Campbell is an ambitious student who decides to dissect an eye before he has completely learned of all the different layers. His supervisor is upset but asks him to take pictures of the fibrous layer of the eye. Which one of the following should he take pictures of to keep his supervisor happy and to avoid being in trouble?
A) Ciliary Body
B) Iris
C) Choroid
D) Sclera |
D) Sclera |
|
|
The repolarization phase of the action potential in a neuron is driven by the A) closure of calcium channels. B) opening of sodium channels. C) opening of sodium channels and closure of potassium channels. D) closure of sodium channels and opening of potassium channels. |
D) closure of sodium channels and opening of potassium channels. |
|
|
Jeor has had an accident that has damaged the ventral funiculus of his spinal cord. Assuming that this is specific and localized to this area, which one of the following would most likely be affected?
A) Central processing of Pacinian corpuscle activation
B) Corticospinal tracts
C) Sensory inputs to wide dynamic range neurons
D) Bilateral descending motor information |
D) Bilateral descending motor information |
|
|
Roger Sterling has isolated secretions from the visual system that contain antibodies and lysozyme.Where did he most likely isolate this fluid? A) Medial commissure of the eye B) Anterior chamber of the anterior segment C) Scleral venous sinus D) Posterior chamber of the anterior segment |
A) Medial commissure of the eye |
|
|
Peggy Olson is writing a commercial for an optical company that specializes in selling merchandise toPhysiology students. She needs to be as precise as possible in her understanding of visual accommodationin order to make sure that the students will buy the company’s merchandise. Which one of the statementsshe is planning to use in the commercial is the most accurate? A) Ciliary muscles contract during accommodation B) Circular muscles in the iris contract during accommodation C) Ciliary muscles relax during accommodation D) Radial muscles in the iris contract during accommodation |
A) Ciliary muscles contract during accommodation |
|
|
When more than one ion species (i.e., Cl- and Ca+2) is present on both sides of the membrane, thechemical driving force acting on Ca+2 will include A) the most concentrated ion only. B) all positively charged ions. C) all negatively charged ions. D) Calcium only. |
D) Calcium only. |
|
|
Joan Harris want to become a partner in her clinical practice. In order to do so, she needs to pass theophthalmology board exams that test heavily on the consensual pupillary reflex. She is having difficultywith the following question and asks for your help. Which one of the following statements regarding thisreflex is not correct? A) The stimulus initially sends information to the thalamus B) Radial muscles in both eyes contract C) Parasympathetic stimulation is required D) The reflex is organized at the level of the midbrain |
B) Radial muscles in both eyes contract |
|
|
Which of the following statements about sensory coding is FALSE? A) The location of the stimulus is coded for by the receptive field activated. B) The type of stimulus is coded for by the specific pathway activated. C) The energy from the environment in general will cause depolarization D) The intensity of stimulus is coded for by the size of the action potential. |
D) The intensity of stimulus is coded for by the size of the action potential. |
|
|
Identify the correct statement regarding the blood brain barrier A) Blood vessels found in the brain mostly contain large gaps B) Concentration of K+ in blood vessels and the interstitial fluid is almost identical C) Between blood vessels and the cerebrospinal fluid, there is free diffusion D) Most of the brain is protected by blood brain barrier, but it is not continuous |
D) Most of the brain is protected by blood brain barrier, but it is not continuous |
|
|
When the myosin heads are loosely bound to the actin filaments, the __________ span the space between the parallel thick and thin filaments. |
Crossbridges span the gap. |
|
|
A muscle is referred to as a(n) __________ if the bones it connects move closer to each other when that muscle contracts. |
Flexor |
|
|
How does transduction involve ion channels in the receptor's membrane? |
The stimulus opens or closes ion channels directly or via a second messenger Usually a channel is opened, letting Na+ or other cations into the cell, depolarizing the membrane In a few cases K+ leaves the cell, hyperpolarizing the membrane In the case of vision, light closes cation channels, hypoerpolarizing the receptor membrane |
|
|
What is a threshold? |
Minimal stimulus that will activate/produce an action potential in the receptor itself or its downstream sensory neuron |
|
|
What is perceptual threshold? |
Minimal stimulus that will make you aware of a sensation It depends on attention, as the brain can filter out certain stimuli when you are drowsy or attending to something else This can help determine if you are smelling something good or hearing something |
|
|
What are primary (or first-order) sensory neurons? |
The first neurons in the system. These are the actual neurons that propagate action potentials They have synapses onto secondary sensory neurons which synapse onto tertiary and so on At each stage, many presynpatic neurons may provide input to one or a few postsynaptic neurons, a pattern called convergence, which allows secondary and teriary and higher neurons to combine information from many receptors |
|
|
What is convergence (in aspect of neurons)? |
Where many presynaptic neurons may provide input to one or a few postsynaptic neurons which allows secondary, tertiary and higher neurons to combine information from many receptors |
|
|
What is stimulus modality? |
Determine whether it is a light, sound or touch
Indicate modality by labeled lines (activity on neurons in the visual pathway is interpreted by the CNS to mean light; in the auditory pathway it means sound) |
|
|
Where does the olfactory pathway pass through in the brain? |
Through the olfactory bulb It bypasses the thalamus but goes to the cortex, amygdala and hippocampus |
|
|
Where is the auditory cortex found in (which brain lobe)? |
Temporal
|
|
|
What are chemoreception? |
Chemoreception is evolutionary old: bacteria use it to guide their movements; animals without brains use it to find food and mates May have evolved into chemical synaptic communications Smell and taste are forms of chemoreception These receptors are primary olfactory neurons, which project into the olfactory bulb |
|
|
What is the olfactory bulb? |
The olfactory bulb is an extension of the forebrain and lies on the underside of the frontal lobe |
|
|
What do olfactory neurons make synaptic connections with? |
Primary order neurons Axons of primary sensory neurons form the olfactory nerve and synapse with secondary sensory neurons in the olfactory bulb |
|
|
Explain what developing neurons do in the olfactory sensory? |
Stem cells in the basal layer of the olfactory epithelium continuously divide to create new neurons. As you get older, you are less likely to grow more stem cells and regenerate neurons (which can proceed the development of Alzheimer's disease) These developing neurons will have to send a projection up into the mitral cells as well as sending out a process down to the mucus layer as they start to develop |
|
|
Describe odorant receptors: |
Each odorant receptor is a protein which is responsible for transducing a sense into electrical activity which will then activate primary neuron cells These are G protein-coupled membrane proteins (each GPCR is different and will bind a different odorant and different combiantions of odorant receptors allow us to smell many odors) When an odorant molecule binds its receptor protein, it activates a G protein, Golf, which increases the local concentration of cAMP cAMP-gated cation channels open, depolarizing the cell and triggering an action potential that travels along the axon to the bulb There are also pain and temperature receptors in the nasal cavities |
|
|
What is the odorant receptor pathway? |
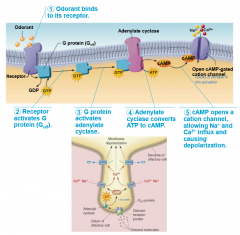
1) Single odorant binds to the odorant receptor (odorants dissolve best in liquid and doesn't interact well with its receptor unless in a psuedoaqueious environment) 2) Receptor activates G proetin (G_olf) 3) G-protein activates adenylate cyclase which converts ATP into cAMP 4) cAMP opens cation channels, allowing Na+ and Ca2+ influx and causing depolarization The Na+ causes depolarization and impulse transmission Ca++ causes olfactory adaptation which is a decrease response to sustained stimulus There will also be Cl- leaving the cell which will bring its negative charge from inside to outside causing a further membrane depolarization |
|
|
Why do animals have a more sensitive and powerful sense of smell than humans? |
Animals per unit area imbedded in the cilia tend to be much higher in animals so molecules have a much easier probability of finding a receptor in animal olfactory system than in humans |
|
|
What are mitral cells? |
They are responsible for detecting different types of odors. They can amplify, refine and relay signals. They can send signals towards the brain Olfactory receptor cells synapse with mitral cells in glomeruli of olfactory bulbs Can be inhibited by amacrine granule cells releasing GABA Impulses from activated mitral cells travel via olfactory tracts to piriform lobe of olfactory cortex Some information to frontal lobe (smell consciously interpreted and identified) Some information to hypothalamus, amygdala, and other regions of limbic system (emotional responses to odor elicited/where smell is part of your memory) |
|
|
What do amacrine granule cells do? |
They release GABA to inhibit mitral cells (only highly excitatory impulses transmitted) |
|
|
What is a glomeruli? |
A series of synaptic connections that make their way from the sensory cell to the mitral cell All the receptors that is sending up to the glomeruli is interacting with the same odorant |
|
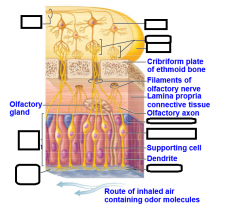
Fill in the missing labels: |
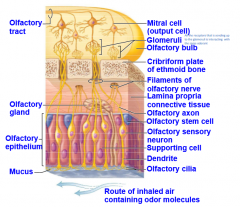
|
|
|
What is vomeronasal organ (VMO)? |
In rodents, an accessory olfactory structure in the nasal cavity, the vomeronasal organ, is involved in behavioural responses to sexpheromones There i no clear evidence for a VMO in humans, but there may be compounds that act as human pheromones |
|
|
What can umami be activated by? |
MSG like meat and cheese
It can also signal nutrients (sugar and glutamate) |
|
|
What can trigger sour taste? |
H+ |
|
|
What can trigger salty taste? |
Na+ |
|
|
What do tight junctions do in the tongue? |

These get activated by ligands which will activate G-protein coupled receptors
|
|
|
What do Type 1 cells do on the tongue? |

Type 1 (support) cells may sense salt Believed to be activated by ions It is a polarized epithelial cell Sweet and umami involves T1R receptors |
|
|
What do Type 2 cells do on the tongue? |

Type 2 (receptor) cells sense sweet, bitter and umani Release ATP which acts on neurons and Type 3 It is a polarized epithelial cell It expresses G-protein-coupled receptors Bitter involves ~30 T2R receptors These receptor proteins are associated with a G-protein called gustducin, which activates signal-transduction pathways These pathways increase intracellular [Ca++], triggering release of ATP through what looks like exocytosis |
|
|
What do type 3 cells do on the tongue? |

Type 3 (presynaptic) cells sense sour These are the only type cells on the tongue that form synapses with sensory neurons, activating them with serotonin It is a polarized epithelial cell |
|
|
Do salty and sour transduction involve ion channels or G-proteins? |

Ion channels Na+ enters Type 1 cells through apical channel, such as epithelial Na+ channel, depolarizing the cell Sour is controversial. It involves Type 3 cells but it is not clear whether H+ acts on receptor or enters the cell. H+ may act on ion channels from both the intra- and extra-cellular sides of the membrane (H+ can either directly enter cell or block efflux of K+) |
|
|
What cranial nerves does the axons of gustatory neurons travel through? |
7, 9, 10 They synapse in medulla, from there the pathway leads to the thalamus and then the gustatory cortex |
|
|
Describe the nerve endings in the mouth: |
The nerve endings in the mouth have TRP receptors activated by capsaicin, menthol, cinnamon, mustard, etc. and projecting via the trigeminal nerve (cranial nerve V) |
|
|
What is the fifth cranial nerve? |
The trigeminal nerve |
|
|
Describe the gustatory pathway: |
Cranial nerves 7 and 9 carry impulses from taste buds to solitary nucleus of medulla Impulses then travel to thalamus and from there fibers branch to gustatory cortex in the insula and the hypothalamus and limbic system (appreciation of taste) Vagus nerve transmit from epiglottis and lower pharynx |
|
|
What are anosmias? |
Olfactory disorders The first sense that disappears as you get older Proceeds neurodegenerative diseases Most results of head injuries and nuerological disorders (such as Parkinson's disease) Example would be uncinate fits |
|
|
What is uncinate fits? |
Olfactory hallucinations Olfactory auras prior to epileptic fits People who have epileptic seizures say they smell something that isn't there before it happens |
|
|
What does the external ear consist of? |
Pinna and the ear canal, sealed at its end by the tympanic membrane, or eardrum |
|
|
What is the middle ear? |
An air-filled space connected to the pharynx by the Eustachian tube |
|
|
What does the inner ear contain? |
Vestibular apparatus for equilibrium and cochlea for hearing |
|
|
What is the vestibular apparatus? |
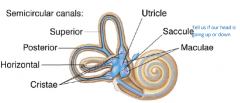
Also known as the membranous labyrinth It is a set of fluid-filled chambers Contains the cristae, maculae, saccule and other sections There are 3 orthogonal (90 degree to one another) canals, for the 3 dimensions of head rotation The horizontal canal sense side-to-side rotation, as in shaking your head "no"; the superior and posterior canals sense up-and-down nodding and ear-to-should tilt Each canal is filled with a fluid called endolymph and ends in a bulge (ampulla) containing its cristia |
|
|
What is the saccule? |
Tell us if our head is going up or down |
|
|
What is the cristae? |
The cristae of the semicircular canals sense the rotational acceleration of the head |
|
|
What is the maculae? |
The maculae of the 2 otolith organs (utricle and saccule) sense the head's tilt and translational acceleration |
|
|
Which canal of the vestibular apparatus detects side-to-side rotation? |
The horizontal canel |
|
|
Which canal(s) of the vestibular apparatus detect up-and-down and ear-to-should tilting? |
Superior and posterior canals |
|
|
What is the fluid in the canals of the vestibular apparatus? |
Endolymph |
|
|
What are hair cells? |
These cells have stiff cilia called sterocilia in their apical membranes
The cilia extends into a gelatinous mass called the cupula, which seals off the canal
When the head turns, the endolymph, owning to its inertia, lags behind and so pushes on the cupula, bending the hairs (if head swings right, then endolymph bends the hairs to the left)
Thereis a polarity towards the longest of the cilia (kinocllium) where there areother, non-longest sterocilia which point towards the kinocllium which gives itsome directionality and when they bending a certain direction, they cause different receptors to open which can leadto depolarization leading to more glutamate so can tell where head is benttowards by direction of sterocilium If the hairs bend toward the kinocilium, then the hair cell depolarizes and releases transmitter, activating a sensory neuron; if the bend away, the cell hyperpolarizes
Hair cells are tonically active, releasing neurotransmitter onto primary sensory neurons |
|
|
What is the kinocilium? |
The longest cilia on the hair cell |
|
|
What happens if hair cell's cilia bend toward the kinocilium? |
Depolarization and release of transmitter, activating the sensory neuron |
|
|
What happens if the hair cell's ciliar bend away from the kinocilium? |
Hyperpolarizes |
|
|
What is the otolith membrane? |
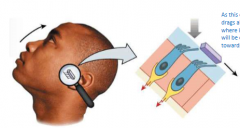
In the maculae, hair cells extend their steocilia into a gelantinous otolith membrane On the membrane's surface are particules of calcium carbonate and protein, called otoliths. When gravity or acceleration moves the otoloiths then the membrane moves with them, bending the hairs When the head is upright, the macula of the utricle is horizontal and that of the saccule is vertical When the head is tilted, gravity bends the hairs. As the calcium otolith slides, it drags along the sterocilia with it where in this orientation, they will be excited as they are pulled towards the longer cilia. |
|
|
What is the cochlea? |
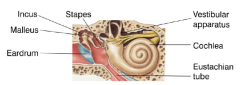
The cochlear hair cells activate primary sensory neurons of the cochlear branch of the vestibulocochlear nerve (cranial nerve 8) There are three bones here which are needed to amplify the vibration up against the eardrum by 22 fold so that movements of air can becomes movements of fluids in the cochlea |
|
|
What is sound? |
Pressure waves At the peaks of waves, the molecules are crowded together and the pressure is high; at the troughs the molecules are far apart and the pressure is low |
|
|
What is frequency and how do we (humans) perceive it? |
Frequency is the number of peaks that pass a given point each second We perceive frequency as pitch (the changes in frequency) where low frequencies as low-pitched sounds and high frequencies as high-pitched sounds Frequency is measured in waves per seconds: Hertz (Hz) Most people can hear frequencies from 20-20,000 Hz. Acuity is highest from 1000-3000Hz |
|
|
In the aspects of sound/hearing, what is amplitude? |
Amplitude is the pressure difference between peak and trough Amplitude is the main factor that determines our perception of loudsness: small-amplitude waves are soft, large amplitudes are loud More precisely, loudness relates to sound intensity, a function of amplitude measured in units called decibels (dB) that are logarithmic (in increase of 10dB means a 10-fold increase in intensity) Normal conversation is ~60dB where >80dB can damage hearing |
|
|
How is sound energy conveyed in the cochlea? |
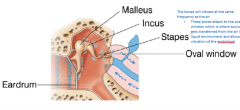
By the bones in the middle ear They will vibrate at the same frequency as the air Sound waves shake the eardrum and the attached malleus bone transduces sound waves into vibrations Malleus connects to incus which connects to stapes, which seals off the oval window leading into the cochlea. These 3 bones amplify the vibration as they convey it to the inner ear |
|
|
Where can perilymph be found? |
In the vestibular duct (or scala vestibuli) and tympanic duct (scala tympani) |
|
|
Where can endolymph be found? |
In the cochlear duct (scala media) By the way: it has high [K+] and low [Na+] |
|
|
What is the organ of corti? |
In this chamber and only this chamber, the organ of corti allows you to hear It is rich in K+ which can hyerpolarize where if it comes into the cell, in this case, it depolarizes the hair cells It sits on top of the basilar membrane and under the tectorial membrane. All the hair cells sit on the basilar membrane which go from ovial window to tree line. Each hair cell has 50-100 sterocilia, which extend into the tectorial membrane The fluid waves in the perilymph deform the basilar and tectorial membranes, bending the cilia back and forth |
|
|
What is IHC (in relation to hearing)? |
Inner Hair Cell Detects sounds As it detect sounds, it bounces up and down causing fluids in the chamber to move with it which will pull open the tectorial membrane |
|
|
What are tip links? |
Sterocilia are attached by protein bridges called tip links which open and close ion channels in the cilia membrane At rest, ~10% of the channels are open They will close when hair cell is being hyperpolarized They can break if they move around too much and when this happens, you hear a ringing sound as it cannot close and is constantly active where the neuron is constantly will be excited |
|
|
Do we hear bilaterally? |
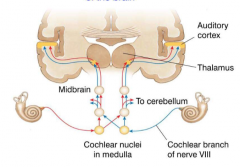
Yes, there is a crossing over event at the cochlear nuclei in the medulla. |
|
|
Explain how the brain localizes sounds based on loudness and timing: |
If a sound is louder in the right ear, than in the left it is coming from the right side of the head. Loudness is conveyed by firing frequency like how louder sounds make auditory sensory neurons fire at a faster rate |
|
|
What are the three kinds of hearing loss? |
Conductive Central Sensorineural |
|
|
What is conductive hearing loss? |
Sound cannot be transmitted through the external or middle ear to the CNS |
|
|
What is central hearing loss? |
There is damage in the cortex or the pathways from cochlea to cortex |
|
|
What is sensorineural hearing loss? |
There is damage to the hair cells or elsewhere in the inner ear. Mammals cannot replace dead hair cells but birds can. |
|
|
What are cochlear implants? |
Restored hearing to many deaf people A tiny microphone, processor and transmitter fit behind the ear. These convert sound into electrical impulses and then into radio waves, and send the radio signal to a receiver and 8-24 electrodes under the skin The electrodes relay the signals to the cochlea or the auditory nerve, bypassing any damaged areas After surgery, recipients are trained to understand what they hear. |
|
|
What is simple reflexes? |
Sensory neurons make synapses with spinal cord monotneurons to mediate simple reflexes Simplest form of motor control |
|
|
What are CPGs (is aspect of movement)? |
Central Pattern Generators Networks of interneurons in the spinal cord and brainstem coordinate the interaction of many different motor groups (locomotion, respiration) Anything rhythmic requires CPGs Are located principally in the spinal cord and brainstem (and also hypothalamus) CPGs are activated in order of relevance Important in behaviour responses Important in locomotion and motor control |
|
|
What is complex/volitional movement? |
Motor output that is planned and refined by the motor cortex, basal ganglia and cerebellum |
|
|
Explain the reflex arc: |
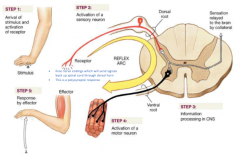
1) Arrival of stimulus and activation of receptor 2) Activation of sensory neuron (free nerve ending which will send signals back up spinal cord through dorsal horn, this is a polysynaptic response) 3) Information processing in CNS 4) Activation of a motor neuron 5) Response by effector |
|
|
What is the stretch reflex? |
Stimulus: passive stretch of a muscle by applied load or contraction of antagonist muscle (75m/s) Response: active contraction of muscle Very sensitive and fast due to muscle spind afferents, and monosynpatic connection to motoneurons Essential for stabilizing posture; reflex strongest in postural muscles Short latencies of about 25ms for forearm muscles, 37ms for ankle extensors Parallel multisynaptic paths through spinal cord and a transcortical path During movement, reflex suppressed |
|
|
What is the golgi tendon reflex? |
Stimulus: active tension in muscle Response: relaxation or reduction of tension GTO afferents (lb) synapse on interneurons in intermediate zone of spinal cord lb-interneurons inhibit (alpha)-motoneurons of same muscle Golgi tendon reflex signals the lb axon (large diameter, myelinated) to relax which prevents over contraction when a load is picked up What it does is prevent movement Acts in concert with stretch reflex to stabilize posture Suppressed when net motion is desired (when we move, we turn Golgi tendon reflex off) |
|
|
What is the stimulus and response for a stretch reflex? |
Stimulus: Passive stretch of muscle Response: Active contraction of muscle |
|
|
What is the stimulus and response of Golgi tendon reflex? |
Stimulus: Active tension in muscle Response: Relaxation or reduction of tension |
|
|
Under what conditions is the Golgi tendon reflex output reversed? |
Positive feedback instead of negative feedback Stance phase of walking |
|
|
What is flexion withdrawal reflex? |
Stimulus: noxious injury of limb Response: Flexion of joints proximal to stimulus (extension distal to stimulus) A(delta),C nociceptor afferents synapse on interneurons in superfical dorsal horn Multi-synaptic path to motoneurons |
|
|
What is the stimulus and response of flexion withdrawal reflex? |
Stimulus: Noxious injury of limb Response: Flexion of joints proximal to stimulus |
|
|
What is reciprocal inhibition? |
Intermediate zone neurons are found between ventral region of spinal cord Basic property of intermediate zone is reciprocal inhibition: the activation of one motor nucleus is coupled to inhibition of antagonistic motor nucleus (activation of flexor motoneurons elicits inhibition of antagonist extensors) When co-contraction of antagonists desired (for joint stiffness), this circuit is suppressed |
|
|
What is crossed extension? |

Full expression of flexion withdrawal reflex involves contralateral extension for increased postural support (mainly in legs) Commissural interneurons carry signal to contralateral spinal cord The only way the other leg to know what to do, the same interneuron to call withdrawn, it will go to the other leg and extend to provide support This reflex is sorta voluntary |
|
|
What does ipsilateral mean? |
Same side where stimulus is recieved |
|
|
What does contralateral mean? |
Opposite side of where stimulus is received |
|
|
What is extensor thrust reflex? |
Stimulus: Pressure on sole of foot (innocuous) Response: Activation of leg extensors A(beta) mechanoreceptors project to intermediate zone interneurons to extensor motoneurons Reflex operates only during stance It is influenced by the contricospinal tract Can be elicited at rest (like in toes by vigorous stroking of sole of foot) If contricospinal tract is damaged (stroke, spinal injury), the reflex pattern is switched to flexion withdrawal |
|
|
What is Babinski pattern? |
If youdamage your spinal cord, your toes will do opposite which is a switch of antigravity pattern to a flexion withdrawal |
|
|
What is the stimulus and response of extensor thrust reflex? |
Stimulus: Pressure on sole of foot (innocuous) Response: Activation of leg extensors |
|
|
What is presynaptic inhibition? |
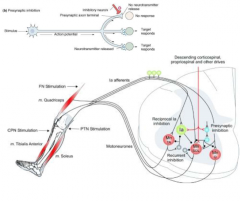
Presynaptic inhibition of afferent or interneuronal terminals is main mechanism for regulating and switching reflex effects When on route to a motor nucleus is inhibited, another can be disinhibited |
|
|
What is the vestibulospinal reflex? |
Normal purpose is to stabilize the body Stimulus: Downward deviation of head on one side to activate otolith afferents Response: 'downhill' limbs extend As youtilt your head on one side or the other, you get ipsilateral extension of motorneurons, and contralateral flexion on the opposite side Otolith afferents activate lateral vestibulo-spinal tract: ipsilateral projection to extensor (antigravity) motor nuclei on side head is turned and flexors induced on opposite side |
|
|
What is the stimulus and response of vestibulospinal reflex? |
Stimulus: Downward deviation of head on one side to activate otolith afferents Response: 'downhill' limbs extend |
|
|
What is vestibulo-ocular reflex (VOR)? |
This is the concentration/fix on a gaze
Stimulus: Head angular rotation; excites semicircular canals (rightward rotation excites right horizontal canal afferents) Response: Eye movement at opposite angular velocity to head rotation Canal afferents project to superior vestibular nucleus where VOR is organized Eye saccade occurs first (less ienrtia or less effort to move these) when tracking something or someone When head starts to move, if eye is already on target, the head movement will shift gaze off the target As soon as eye foveates target, VOR is 'turned on', stabilizing gaze despite continuing head movement |
|
|
What is the stimulus and response of VOR? |
Stimulus: Head angular rotation; excites semicircular canals (rightward rotation excites right horizontal canal afferents) Response: Eye movement at opposite angular velocity to head rotation |
|
|
How does VOR function? |
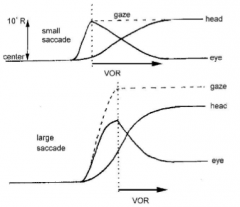
Eye saccade occurs first (less inertia or less effort to move these) when tracking something or someone
When head starts to move, if eye is already on target, the head movement will shift gaze off the target
As soon as eye foveates target, VOR is 'turned on', stabilizing gaze despite continuing head movement |
|
|
What is the stimulus of stretch reflex, Golgi tendon reflex, flexion withdrawal, extensor thrust, vestiboluspinal and VOR? |
Stretch: Passive stretch of a muscle by applied load or contraction of antagonist muscle (75m/s) Golgi tendon: Active tension in muscle Flexion withdrawal: Noxious injury of limb Extensor thrust: Pressure on sole of foot (innocuous) Vestiboluspinal: Downward deviation of head on one side to activate otolith afferents VOR: Head angular rotation; excites semicircular canals (rightward rotation excites right horizontal canal afferents) |
|
|
Which reflex would give me 'downhill' limb extension? |
Vestiboluspinal reflex |
|
|
What reflex would give be active contraction of muscles? |
Stretch reflex |
|
|
What reflex would I want to use when I want to reduce tension on muscles? |
Golgi tendon reflex |
|
|
Explain the leg step cycle: |

The step cycle of each leg during walking is programmed by a network of neurons within the intermediate zone of the lumbar cord Properties of the network: 1) Pacemaker neurons, diffuse excitation 2)Reciprocal inhibition 3) Phase-dependent reflexes |
|
|
What are the "half-center" structures of CPG? |
1) Flexor burst generator network of neurons drives flexor motor nuclei (within intermediate zone) - lifts leg then turns off 2) Extensor burst generator drives extension Both are spontaneously active when not inhibited and they can mutually inhibit one another |
|
|
What is flexor burst generator? |
The fluxion phase of the leg swing has a fixed duration, regardless of the speed of locomotion Flexor network has a build-up of inhibition that eventually stops the burst of action potentials which end of activation of flexor motoneurons Reciprocal inhibition of extensor burst network ceases causing extensor network active |
|
|
In the transition to leg swing, when would the E3 phase stop? |
1) Leg is not bearing weight 2) Hip is extended 3) Opposite leg is in stance (bearing weight) Crossed projections provide correct phase-linking of CPGs on each side |
|
|
Describe the CPGs role in arm swings: |
CPGs in cervical cord program motion of arms during walking Flexion phase in arms is synchronous with contra-lateral flexion in leg: diagonal pattern to cancel torque on trunk This phase-linking occurs via propriospinal tracts |
|
|
Describe the CPGs role in upper body balance: |
Bipedal humans must produce postural compensation in the trunk and head to maintain stability on top of moving legs Requires postural CPGs in reticular formation to coordinate upper body motion with spinal step cycles Spinally injured patients cannot walk without trunk support Spinoreticulothalamic pathways send information centrally about large regions of the body |
|
|
How is the stability of the head angle maintained? |
By combinations of visual vestibular and propioceptive reflexes |
|
|
What is mesencephalic locomotory region? |
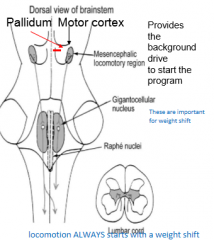
This is a midbrain 'switch' that turns on reticulospinal locomotory CPGs which then activate spinal CPGs [locomotion starts with weight shift (postural change)] Governs speed of locomotion: the faster the rate of impulses, the faster the locomotion No pattern generation though (MLR just initiates the locomotion, does NOT generate patterns) Locomotion ALWAYS start with weight shift |
|
|
How is there postural maintenance? |
Organized in reticular formation of pons and medulla Relies on 3 sensory sources: 1) Somatosensory (especially proprioceptive) 2) Vestibular (gravitational reference) 3) Visual (slower system, but important vertical cues and motion cues) |
|
|
Describe eye-head co-ordination: |
Movement to inspect novel visual stimulus is programmed in superior colliculus
This area computes how much and in what direction gaze must be shift to 'foveate' target Send same motor signal to extraocular and neck motor centers Eye-head coordination is function of VOR |
|
|
Describe the collicular spatial map: |

Position of activated cells in s. colliculus codes spatial location of visual/auditory stimulus Spatial map is calibrated for eyes/head facing straight forward Activated cells provide motor signal to shift gaze in order to foveate stimulus |
|
|
What is synergy? |
A group of muscles contracting together for a specific purpose Synergies that are organized by reticulospinal tract are very widespread (typically cover half of the body) for generating support postures In contrast, rubrospinal (and corticospinal) synergies are highly localized |
|
|
What is the red nucleus? |
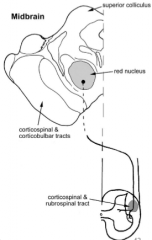
It is actually red in colour and part of the spinal synergy Rubrospinal cells within the red nucleus activate localized synergies, especially in distal limbs and in the face (gripping and twisting movements of hands) Reticulospinal and vestibulo-spinal tracts organize widespread postural and locomotory synergies |
|
|
What is the motor cortex? |
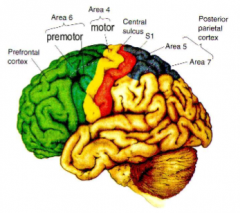
Located on the precentral gyrus, has somatotopic organization Layer 5 pyramidal cells are large; project to motor nuclei and interneurons in brainstem and spinal cord (corticobulbar/spinal tract) Direct corticospinal synapses on moto-neurons mostly to distal limb and speech motor nuclei |
|
|
What is a motor field? |
For motor fields, we are talking about how one corticospinal axon synapses with a set of motor nuclei, in more than one spinal segment Set of synaptic contacts with motor nuclei constitutes the motor field; many synapses are 'silent' Some motor nuclei much more strongly influenced than others The motor field provides potential for plasticity |
|
|
What are somatosensory inputs? |
Only sensory input with direct access to motor cortex
Cutaneous input comes from somatosensory association areas; related to postural and motion information Proprioceptive input direct from thalamus (and from somatic association cortex) |
|
|
What are transcortical reflexes? |
Allow you to adjust influx incoming Much more versatile and modifiable than spinal reflexes Proprioceptive signals from one muscle can be used to trigger contractions in other muscles leading to synchronize actions at several joints When proprioceptive afferent inputs are lost, the person cannot synchronize reversals of motion at elbow and shoulder. Arm trajectories become both arbitrary and totally inconsistent |
|
|
What is the grasp reflex? |
Transcortical cutaneous reflex Slippage of object in fingers activates mechanoreceptors Direction of slip computed in somatosensory association areas Increased finger tension triggered in motor cortex |
|
|
What is the premotor area in the cortex? |
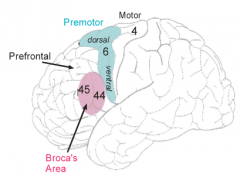
Set of regions projecting into motor cortex (but also with parallel routes to motor nuclei) Select motor cortical synergies into proper sequence for a given movement Pattern generation role for learned, highly evolved movement Different premotor areas need to be activated depending on what we want to do It processes sensory inputs, especially visual and auditory for cueing movement phases (dorsal visual stream to dorsal half (spatial location), ventral visual stream to ventral half) |
|
|
What is Broca's area? |
Premotor zone for sequencing language elements for speech or writing-typing input from Wernicke's area |
|
|
What is preparatory activity? |
Premotor neurons set up the motor cortex
Hence they often are not active during performance Typically active during preparatory phase of movement: facilitating appropriate synergies in motor cortex Premotor neurons are typically active only when they are preparing the motor cortex, but not when the motor responses/contractions are actually occuring |
|
|
What is the supplmentary motor area (SMA)? |
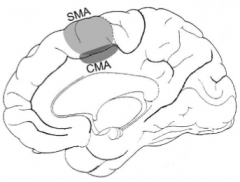
Found on the medial wall of the hemisphere; somatotopic representation of body, but less detail than on the motor cortex Processes internal 'volitional' signals that drive movements; regulates sensorimotor drives via lateral frontal lobe Controls bilateral coordination of limbs when different motions done on each side |
|
|
What is the cinglulate motor area (CMA)? |
Located within cingulate sulcus Gross somatotopic representation of body Processes emotional and motivational drive to movements The 'limbic' motor center; important in many epileptic seizures Also contributes to corticospinal tract |
|
|
What is the cortical pattern generation? |
Sequencing the elemental synergies involved in speaking or picking up a teacup is a "grand" production Temporal, and parietal cortex provide sensory cues to promotor area Limbic cortex provides emotional input Basal ganglia provide volitional input |
|
|
What is the basal ganglia? |
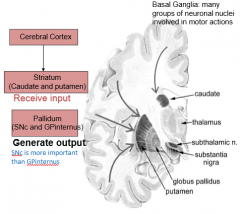
Regulates flow of 'volitional' drive to premotor centers 2 tiers of nuclei, collectively known as 'striatum' and 'pallidum' Striatum: Topographic input from cerebral cortex and thalamus (centromedian nucleus) Pallidum: Projects to premotor centers |
|
|
What is the striatum? |
Found in basal ganglia Topographic input from cerebral cortex and thalamus (centromedian nucleus) |
|
|
What is the pallidum? |
Found in basal ganglia Projects to premotor centers Neurons are tonically (always active) discharging These work to inhibit the premotor thalamus, sup. colliculus, mesenchephalic locomotory regions (MLR responsible for initiation of walking) Pallidum tonically suppresses motor programs In order to initiate a specific movement, a specific premotor center is disinhibtied Inhibiting the pallidum by turning on things within the striatum will lead to activation of CPGs via premotor neurons, and activation of motor synergies in the result |
|
|
What happens when you inhibit pallidum by turning on things within the striatum? |

Will lead to activation of CPGs via premotor neurons and activation of motor synergies as the result |
|
|
What is striatal modulation? |
Substantia nigra (SN) neurons containing dopamine facilitate striatopallidal projection neurons Striatum chooses motor act to perform at any instant, guided by cortical and reticular inputs SN dopaminergic system plays a key role in determining active part of striatum SN neurons are most important for turning on the striatum via dopamine |
|
|
What are the symptoms of Parkinson's disease? |
Movement problems Festinating gait Limbs exhibit classic cogwheel rigidity Very little voluntary movement and when there is movement, it is "unbalanced" Pill-rolling tremor Face-mask appearance towards later stages Sometimes, but not always assoicated with dementia (can also affect degeneration in other parts of the brain) |
|
|
What is Parkinson's disease caused by? |
Loss of SNc dopaminergic neurons |
|
|
What pallidal modulation? |
Level of activity in pallidal neurons can be adjusted by subthalamic nucleus Excitatory effect on pallidum to counter-balance striatal inhibition Regulates speed/force of movements: over-activity responsible for bradykinesia Lesion of subthalamic n. to hemiballismus (unilateral wild arm movements) |
|
|
What is the cerebellum? |
Not essential for motor performance
Agenesis of cerebellum is the delayed motor development and perpetual clumsiness
Cerebellum is the "conductor" of the motor system; it does not generate any movements but gets all the parts of the pattern generating circuits temporally coordinated |
|
|
What is agenesis of the cerebellum? |
Delayed motor development and perpetual clumsiness |
|
|
What is the cerebellar cortex? |
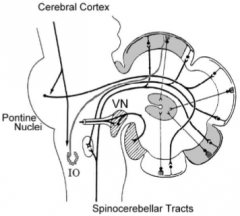
Receives most of input Cortex is heavily folded into folia Auditory and visual inputs goes to the cerebellum Spinocerebellar pathway is the somatosensory input but particularly vestibular input to the structure known as vermis |
|
|
What is the cerebellar nuclei? |
Located in the core of the cerebellum Provide the excitatory output of cerebellum to motor centers Neurons in cerebellar nuclei are spontaneously active Tonically excite all motor centers (brainstem and thalamic) These include: 1) Fastigial nucleus (posture and locomotion) 2) Interposed nuclei (reach and graps) 3) Dentate n. (fine skills such as writing, speech, etc.) |
|
|
What are cerebellar inputs? |
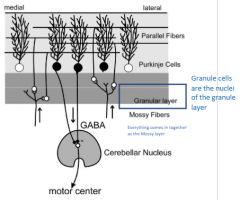
There are three layers where the lower granular layer receives the inputs (via 'mossy fibers' Inputs from spinal cord, brainstem and cerebral cortex and sensory (dynamic) and motor signals Each input projects to a specific region but extensive overlap and mixxing of inputs |
|
|
What are purkinje cells? |
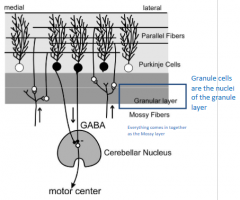
Output neurons of cerebellar cortex Located in middle layers Inhibits neurons in deep cerebellar nuclei by releasing GABA Responds to large sets of granule cells via 'parallel fibers', they therefore recognize a specific coincidence of events |
|
|
What do purkinje cells inhibit and how so? |
Inhibit neurons in deep cerebellar nuclei By releasing GABA |
|
|
How can Purkinje cells regualte the CPGs? |
A cluster of Purkinje cells is activated at a specific instant in a motor performance The Purkinje cells inhibit a target zone in the cerebellar nuclei As a result, a target sensorimotor area is disfacilaited, bringing an associated action to a precisely timed end |
|
|
What is ataxia? |
Cerebellar dysfunction Movement meander because components are not balanced or coordinated |
|
|
What is dysmetria? |
Cerebellar dysfunction Movements overshoot target |
|
|
What is action/intention tremor? |
Cerebellar dysfunction Oscillation around motor target; repetitive correction of previous error due to dysmetria |
|
|
What is ANS? |
Autonomic nervous system Part of the CNS controlling internal organs, endocrine function, blood flow, smooth muscle of the eye, viscera, etc 2 efferent (outflow) subsystems: i) Sympathetic: Stressed related (Fight of Flight) ii) Parasympathetic: Restorative (Rest and Digest) Coordinates cardiovascular, respiratory, digestive, urinary and reproduction functions through visceral effectors Preganglion neurons in the CNS send axons to autonomic ganglia outside the CNS to synapse with postganglionic neurons. Preganglion neurons ALWAYS release ACh Nearly all organs are supplied by the ANS |
|
|
What do we need both subsystems of the ANS? |
If one is always turned on, in the long term, it is not good to keep it always on You need parasympathetic to restore glucagon levels and glucose |
|
|
What are preganglionic axons in the ANS? |
Neurons in the CNS that send axons to autonomic ganglia outside the CNS to synapse with postganglionic neurons They are myelinated |
|
|
What are postganglionic axons? |
Unmyelinated What is released in the postganglionic is not the same between sympathetic and parasympathetic |
|
|
What are ganglionic axons like in the sympathetic system? |
Origin of preganglionic neurons are thoracolumbar They also have short preganglionic fibers (all myelinated) where they almost immediately hit their target as they leave the spinal cord |
|
|
What are ganglionic axons like in the parasympathetic system? |
Origin is not from thoraculumbar but rather the brain stem or carinosacral The preganglionic axons are much longer than in the sympathetic neurons |
|
|
What is the sympathetic nervous system? |
In the sympathetic system, when the flight of flight response is turned on, everything is turn on at the same time |
|
|
What is the parasympathetic nervous system? |
When activated, it will active in localized (specific areas) at a time |
|
|
What are the effects of the sympathetic nervous system? |
Increased alertness Energy and euphoria Increased cardiovascular and respiratory activities Elevation in muscle tone Mobilization of energy reserves |
|
|
Describe the sympathetic efferents: |
Preganglionic efferents from intermedio-lateral horn of thoraco-lumbar cord Synapse in chain of ganglia parallel to cord Postganglion efferents project to target tissue, not always a nerve with two exceptions: 1) ACh is a transmitter at the skin sweat glands 2) Muscle vasodilation Muscle and skin sympathetic efferents normally act independently Major influence is noradrenergic vascoconstriction (causes the blood vessels to constrict, the diameter gets smaller and blood pressure increases) which is tonically active to maintain blood pressure (counteracts vasodilation produced by metabolites) Extremely important for regulation of blood pressure; part of baroreflex Sympathetic cholinergic vasodilation is not significant; metabolites cause vasodilation |
|
|
Describe parasympathetic efferents: |
Originate in several cranial motor nuclei (3, 7, 9, 10-vagus) and intermediolateral part of sacral cord (S2-S4) Project to ganglia embedded in target organ ACh is transmitter; exception is NO |
|
|
What is NO in aspects of parasympathetic system? |
Nitric Oxide Gaseous transmitter; potent vasodilator (especially in the penile region) Not released from vesicles; volatile gas diffuses right through membranes Produced by NO synthase upon activation by Ca++ influex Binds guanylyl cyclase and activates it |
|
|
What does guanlylate cyclase do? |
Turns GTP into cGMP (which can cause vasodilation) |
|
|
What is Enteric Nervous System? |
ENS contains both excitatory and inhibitory motorneurons ENS programs peristalsis and segmentation movements |
|
|
What is the pupillary light reflex? |
Organized in pretectal area of midbrain (tectum is the superior colliculus)
Uses ON and OFF aferents to luminance and darkness detectors, respectively in the olivary pretectal nucleus
Too bright, the parasympathetic reflex via 3rd cranial nerve to ciliary ganglion and circular iris muscles (use ACh for pupillary constriction) so the pupil itself gets smaller
When its too dark, the sympathetic reflex via thoracic cord, sympathetic chain to radial muscles would constrict using NA oe NE for pupillary dilation |
|
|
What is the PeriAqueductalGray (PAG)? |
Midbrain 'premotor' center for autonomic behavioural programs Beahviours are pre-planned and you don't have to think about it |
|
|
What is the reticular activating system? |
Diffuses collection of nuclei within the brainstem Modulatory; causes a global shift in CNS activity; mainly metabotropic mechanisms |
|
|
What is cholinergic? |
A modulatory in the reticular activating system Determines level of attention and sleep-wake cycle; mainly ascending (pontine reticular formation) |
|
|
What is serotonergic? |
A modulatory in the reticular activating system For stressful situations; influences mood, sleep-wake cycle |
|
|
What is adrenergic? |
Modulatory in the reticular activating system For stressful situations and vigilance |
|
|
What is the Acetylcholine system in the brain? |
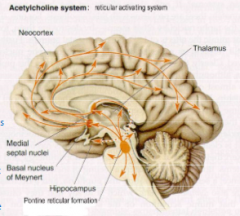
Send its projection up to the medial septial nuclei and basal nucleus of Meynert These will send cholinergic projections to other parts of the brain This begins at the level of the brain stem In here, there is a group of neurons that come together and form the pontine reticular formation Some of these neurons that release ACh, some are descending where majority are ascending When you want to be as awake as possible, you want to turn these on as it will activate the brain through its ascending projections |
|
|
What are tricyclic antidepressants? |
Part of the Acetylcholine system Important in sleep-wake cycles, arousal, learning and memory |
|
|
What serotonin system in the brain? |
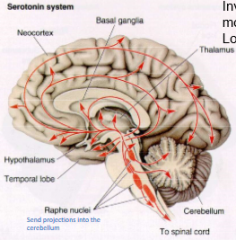
Involved in pain modulation and locomotion Neurons of this system originate in the Raphe nuclei along midline of brainstem |
|
|
What is the norepinephrine system in the brain? |
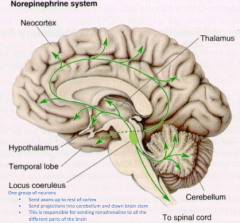
There is a group of neurons called the locus coeruleus which: 1) Send axons up to the rest of the cortex 2) Send projections into cerebellum and down brain stem 3) This is responsible for sending noradrenaline to all different parts of the brain |
|
|
What is the histaminergic system in the brain? |
Originates in the posterior hypothalamus: specifically in the tuberomamillary nucleus Projects throughout forebrain and to other activating systems in brainstem Important in sleep/wake control - this system "turns off" when you fall asleep |
|
|
What is a side effect of anti-histamine? |
Causes drowsiness as it blocks histamine |
|
|
What does the hypothalamic contain? |
NTS - information includes blood pressure and gut distension Reticular formation - from CN X. among them is information about skin temperature, which is relayed to the hypothalamus Retina - some fibers from the optic nerve go directly to a small nucleus within the hypothalamus called the suprachiasmatic nucleus (this nucleus regulates circadian rhythms, and couples the rhythms to the light/dark cycles) Limbic and olfactory systems - regulate behaviours such as eating and reproduction |
|
|
What is thermogenesis? |
If skin temperature is different form body temperature, information relayed from skin detecting changes in the environment There are Thermoreceptors at base of hypothalamus (these can also detect changes in the environment) Interestingly, it appears that warm-sensitive neurons greatly outnumber (and are more sensitive) than cold-sensitive neurons and that these neurons ultimately control thermogenesis More likely to have a homestatic response by raising your temperature by 1C than lowering it by 1C When its too cold, the reaction/response would be skin vasoconstriction, piloerection, decreased cardiac output, shift of fluid out of plasma, and shivering (a somatomotor effect from posterior hypothalamus). This is all an adrenergic input When its too put, the reaction/response would be skin vasodilation, sweating, increased cardiac output, shift of fluid into plasma from extracellular space, ADH release to prevent loss of fluid through urination (anterior hypothalamus). This is all an serotonergic input. |
|
|
What is piloerection? |
Hair on skin will stand up and try to trap as much air in that region as possible |
|
|
Why would you want to decrease cardiac output when its too cold (temperature)? |
Decreasing the blood through skin so this way the heat can be released into the environment |
|
|
Explain the cardiovascular centre? |
Mainly located in the ventrolateral medulla, beside the respiratory center NTS (Nucleus Tractus Solitarii) receives input from baroreceptors and sends this info first to the caudal VLM (ventrollateral medulla). The NTS would receive input from pressure receptors from/near the heart Rostral half excites sympathetic efferents causing raise of blood pressure and heart rate (pressor function) Caudal half inhibits rostral half causing a drop in blood pressure (depressor function) |
|
|
What is the Baroreflex? |
Barorceptors (carotid sinus and aortic arch) -> n. solitary tract -> ventrolat. medulla -> sympathetic output |
|
|
What is VLM? |
VentroLateral Medulla Long group of neurons Blood pressure regulation occurs within/inside the VLM |
|
|
Explain the regulation of feeding by the hypothalamus: |
Many different nuclei within the hypothalamus: 1) Arcuate nucleus control: 1 set of neurons (NPY) drives feeding via paraventricular n.; other neurons (melanocortin) suppress feeding (antagonistic) 2) Neurons in ventromedial nucleus act as glucoreceptors; discharge in relation to ambient glucose levels, inhibit NPY-mediated drive to feeding behaviours Leptin, secreted by white adipose tissue, provides long-term suppression of feeding by inhibiting NPY-containing neurons within the arcuate nucleus |
|
|
What is leptin? |
Leptin, secreted by white adipose tissue, provides long-term suppression of feeding by inhibiting NPY-containing neurons within the arcuate nucleus |
|
|
What is MCrt? |
Melanocortin This is a neurotransmitter that is released when you feel full/not hungry that leads to the satiety network |
|
|
What are the paraventricular neurons? |
This neuron transmitter has NPY and will transmit up and release neuro-peptide Y which will activate the paraventricular neurons which when activated will cause you to start feeding/hunger network |
|
|
What does glucose levels have to do with feeding? |
Glucose receptors in VMN directly inhibit NPY when they become activated
Glucose levels will determine the firing rate of the neuron in the ventral medialnucleus
This can inactivate the NPY neurons if you don't need to feed and have a lot of blood glucose |
|
|
What is Ghrelin? |
Feedback hormone from GI tract to control feeding Ghrelin form empty stomach promotes feeding It will work its way up to the brain and initiate feeding behaviours Positive hormone Released from anterior portion of the stomach every time it starts growling |
|
|
What is PPY? |
Feedback hormone from GI tract to control feeding PPY released from intestine in response to food and insulin from pancreas inhibit feeding at the articulate nucleus |
|
|
What is CCK, OEA? |
Feedback hormone from GI tract to control feeding Fatty acid derivatives Secreted by duodenum activate vagal afferents; via NTS inhibit feeding |
|
|
What is the amygdala? |
Part of basal ganglia controlling autonomic behaviours Input from 'limbic' cortex (border region of the amygdala), autonomic brainstem Output generally inhibitory on PAG-hypothalamus (when you want to turn off the PAG/hypothalamus, you turn on amygdala) Lesions can result in uncontrolled autonomic behaviours ('sham rage', hypersexuality, fear) Memories related to emotional experiences, especially fearful ones, rely on the amygdala for consolidation The amygdala is not the site of memory storage It is designed for learning the circumstances where a behaviour is appropriate |
|
|
What is the limbic cortex? |
Border regions of cerebral cortex at edge of hemisphere (phylogentically old) Consists of cingulate gyrus, hippocampal region (consolidates general memories), and insula Subserves emotional experience, motivation and memory consolidation Neurons from this region project to hypothalamus, PAG, amygdala |
|
|
What is FFI? |
Fatal familial insomia Rare autosomal dominant disease which you cannot sleep It is a neurodegenerative condition in the thalamus Sleeping pills do nothing for these people They will develop dementia |
|
|
What does REM stand for? |
Rapid eye movement |
|
|
What are circadian rhythms? |
Governed by neuronal oscillator with near-24 hour period Entrained to exact day-night cycle by retinal input from ganglion cells with melanopsin Retinal projection to: 1) Suprachiasmatic nucleus 2) Pretectal area to sympathetic efferents to superior cervical ganglion to pineal body (which is important for releasing hormones like melatonin) SCN is situated on top of the optic chiasm (where eyes nerves send their information back and forth) in the hypothalamus SCN is a paired structure on either side of the 3rd ventricle SCN is the master clock (activity lowest at night and highest during day) |
|
|
What is a 24-hour oscillator in aspects of circadian rhythms? |
Based on gene transcription and translation: genes and protein product interactions form a negative feedback loop Mechanism located in suprachiasmatic nucleus of hypothalamus (master circadian clock) Modulated by: 1) Retinal input (retinal ganglion cells that contain melonopsin) 2) Pineal input (seasonal variation) 3) Reticular activating systems (serotonin) |
|
|
What is the pineal body? |
Activated via sympathetic systems in darkness Secretes melatonin (a neuro-hormone); blocked by even small amounts of light (blue and green, not red) Melatonin involved to module sleep in sleep induction Maximal secretion occurs at about 2am Seasonal variations (higher secretion in summer than winter) Sits on top of the thalamus and 3rd ventricle, surrounded by CSF and blood vessels Pineal body can secrete melatonin into CSF and blood stream |
|
|
Explain the sleep-wake cycle: |
In the SCN, it sends axons to two different areas: 1) VLPO - when this gets activated by SCN, you start to fall asleep and inhibits the TMN 2) TMN - this keeps you awake which can inhibit VPL There are orexinergic neurons which induce feeding behaviour (usually) but more specifically, release orexin which activate TMN neurons (this gets activated by the SCN) TMN would release histamines There is a "sleep switch" in ventrolateral preoptic nucleus of the anterior hypothalamus Activation of VLPO by circadian clock (including melatonin), sleep debt (brain in use causes small glycogen stores to drop and adenosine to rise). This is INHIBITORY Waking switch in the TMN or tubermamillary nucleus which involves histamine activating system. This is EXCITATORY to brainstem activation and modulation by orexin/hypocretin |
|
|
A new drug specifically destroys neurons that produce serotonin. Which of the following groups of neurons would most likely be targeted by this new drugs? A) Raphe nucleus B) Purkinje cells C) Type 2 taste receptor cells D) Retinal bipolar cells |
A) Raphe nucleus |
|
|
What area of the nervous system would someone stimulate to produce an increase in the rate of flexion-extension in the step cycles of walking? A) Flexor burst generator neurons in the lumbar spinal cord B) Cingulate motor area (CMA) C) Rubrospinal (red nucleus) neurons D) Mesencephalic locomotory region |
D) Mesencephalic locomotory region |
|
|
What are skeletal muscles? |
Activated by the somatic nervous system Chemical signaling between motor neuron and skeletal muscle are neuro-muscular junctions (NMJ) NJM are the synapses between a motor neuron and a muscle fiber (motor neuron's axon terminal, muscle fiber) Contractile filaments in sacromeres; striated Has a well developed sacroplasmic reticulum (SR) |
|
|
What are sacroplasmic reticulum? |
Storage for Ca Best developed in skeletal muscle |
|
|
What is a T-tubules? |
Allow the spread of AP deep inside the muscle by transmitting the signal to allow muscle fibre to respond |
|
|
What is the sacrolemma? |
The muscle membrane |
|
|
What is a myofibril? |
Most basic unit Run the entire length of the muscle form tendon to tendon |
|
|
What is a motor unit? |
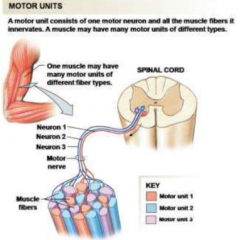
A motor neuron and all the muscle fibers that it innervates Muscle fibers of a motor unit all contract together The smoothness and precision of movement depends on the number and timing of motor units that are activated Small motor neuron are more easily excited than the larger motor neurons and contractions usually begin with small motor units that are innervating too many fibres Muscle contraction begins with small motor units being activated first |
|
|
Why is microsurgery not that good? |
As you get older, muscles get larger |
|
|
What are slow oxidative/type 1 (red) muscle fibers? |
Small Wide z-line thickness High resistance to fatigue High myoglobin content Aerobic respiration High oxidative coapacity Slow twitch rate Low myosin ATPase content |
|
|
What are fast oxidative/type IIA (red) muscle fibers? |
Intermediate diameter Intermediate Z-line thickness Intermediate resistance to fatigue High myoglobin content Aerobic respiration High oxidative capacity Fast twitch rate High myosin ATPase content |
|
|
What is fast glycolytic/type IIX (white) muscle fibers? |
Large diameter Narrow Z-line thickness Low resistance to fatigue Low myoglobin content Anaerobic respiration Low oxidative capacity Fast twitch rate High myosin ATPase content |
|
|
Of the NMJ, what do all motor nuerons release and are they excitatory or inhibitory? |
Acetylcholine Excitatory |
|
|
How does communcation at the NMJ work? |
1) Action potential arrives at terminal bouton 2) Voltage-gated calcium channels open 3) Calcium enters cell triggering release of ACh 4) ACh diffuses across cleft and binds to nicotinic receptors on motor end plate 5) ACh binding triggers opening of channels for small cations (Na and K) 6) Net movement of positive charge in less depolarization 7) Causes action potential in muscle cell 8) Action potential spreads through muscle causing contraction |
|
|
What happens when curare (posion dart) interacts with NMJ? |
Nicotinic receptor blocker This causes the skeletal muscle and NMJ to block voluntary movement Can be used for muscle relaxants (curariform drugs) |
|
|
Explain how muscle contract using myosin and actin? |
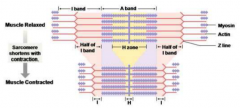
They are very regulated and overlapping When there is contraction, the sacromere shrotens during contraction. The actin and myosin do not change in length but rather slide past each other This is done by the myosin head (dimer) on the M-line which has a binding site for the actin and ATP (as ATPase) |
|
|
Describe the thick myofilament |
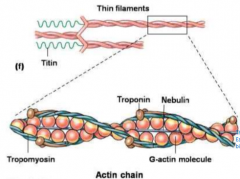
The balls are the actin molecules
Each actin molecule has a binding site for myosin The binding with the myosin head normally does not occur unless there is Calcium
It is two polymerase/chains wound up together |
|
|
Describe troponin and tropomyosin's actions: |
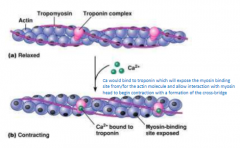
No calcium: troponin holds tropomyosin over myosin binding sites on actin. No crossbridges form betwen actin and myosin, muscle relaxed When calcium present: Binds to troponin, causing movement of troponin, causing movement of tropomyosin, exposing binding sites for myosin on actin. Crossbridges form between actin and myosin. Cycle occurs, muscle contracts |
|
|
What is the crossbirdge cycle? |
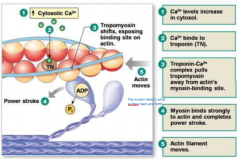
|
|
|
What is the steps of excitation-contraction coupling? |
1) Somatic motor neuron releases ACh, a neuromuscular junction 2) Net entry of Na+ through ACh receptor-channel initiates a muscle action potential 3) Action potential in t-tubule alters conformation of DHP (dihydropyridine L-type calcium channel) receptor 4) DHP receptor opens RyR (ryanodine receptor channel) Ca++ release channels in sacroplasmic reticulum, and Ca++ enters cytoplasm 5) Ca++ binds to troposin allowing actin-myosin binding 6) Myosin heads execute power stroke |
|
|
What is twitch contraction? |
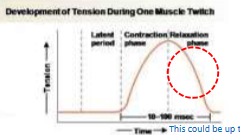
A muscle twitch is a single contraction-relaxation cycle Rise-time and duration of twitch force varies with muscle fiber type (fast glycolytic fibers have a rise time of about 50ms and duration of 120ms) To generate force, you need to have many twitches working together There are three periods/phases to twitch contraction: 1) Latent period - motor neuron already excited but yet not generating any force where AP is traveling down tubules and requires time for Ca to be released 2) Contraction phase - cross-bridge occurs and allows muscle to produce force increasing in tension (steady increase in tension till reach max) 3) Relaxation phase - generating less tension and Ca get pumped back into SR where fewer and fewer cross-bridges are allowed to interact with actin-myosin |
|
|
How can summation lead to tetanus? |
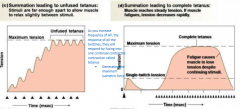
As you increase frequency of AP, the response of all the twitches, they will respond by fusing into one continual contractile contraction called tetanus to generate maximum isometric force Summation can lead to unfused tetanus where stimuli are far enough apart to allow muscle to relax slightly between stimuli Summation can lead to complete tetanus where muscle reaches steady tension and if muscle fatigues, tension decreases rapidly |
|
|
What are smooth muscles? |
Found in internal organs and blood vessels Not arranged in sacromeres Under involuntary control by ANS Must operate over a range of lengths Layers may run in several directions Contracts and relaxes much more slowly Uses less energy Sustains contraction for extended periods They can be classified by location (vascular, gastrointestinal, urinary, respiratory, reproductive, ocular) or communication with neighbouring cells (single-unit, visceral, multi-unit) |
|
|
What is a single-unit smooth muscle? |
Single-unit can activate tension and force and maintain it Single unit smooth muscle cells are connected by gap junctions and the cells contract as a single unit they exhibit spontaneous activity |
|
|
What are multi-unit smooth muscles? |
Found in large airways and ciliary muscles Are not electrically linked and each cell must be stimulated independently |
|
|
Explain what excitation-contraction coupling is? |

Lacks specialized receptor regions
Ca++ is from the extracellular fluid and sacroplasmic reticulum
Ca++ initiates a cascade ending with phophorylation of myosin light chain and activation of myosin ATPase
Steps:
1) Opening of calcium channels in plasma membrane
2) Calcium triggers release of calcium from sacroplasmic reticulum
3) Calcium binds to calmodulin
4) Ca-Calmodulin activates MLCK
5) MLCK phosphorylates myosin heads
6) Crossbridge cycling |
|
|
What is calmodulin? |
When binded to calcium, it activates MLCK |
|
|
What is MLCK? |
Myosin light chain kinase When activated, it phosphorylates myosin head |
|
|
What is considered normal blood pressure? |
(between 90 and 140)/(between 60 and 90) mmHg |
|
|
What is a sphygmomanometer? |
A blood pressure cuff |
|
|
Jill is 18-year old U of T student. She plans to go to medical school so she decides to pratice with a sphygmomanometer that her parent recently purchased. On day 1, she wakes up, goes for a 5k run, skips breakfast and determines that her blood pressure if 110/80 mmHg. The next day, she skips the run and drinks glass of juice and has two cups of tea at breakfest. Her blood pressure is 112/80 mmH. How does the body maintain blood pressure? |
Thebaroreceptor found there was not enough pressure within the body and willchange that by doing it in many different ways such as speeding up the heart,increasing contractility of the heart (via sympathetic pathway) causing vesselsto get smaller |
|
|
Define homeostatis |

The process of maintaining a constant internal environment despite changing conditions |
|
|
What is negative feedback for homeostasis? |
1) Initial stimulus (change within the body someway where the body doesn't like and want to change back to way it was) 2) Triggers response 3) Response decreases stimulus 4) Inhibits initial stimulus |
|
|
What is positive feedback for homeostasis? |
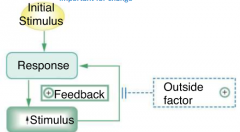
1) Initial stimulus 2) Response triggered 3) Response causes increase/heightens in stimulus (the positive feedback) 4) Triggers more response (can be inhibited by outside factor) |
|
|
Explain the negative feedback of regulation of blood pressure: |
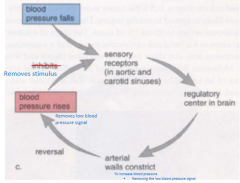
1) Blood pressure falls 2) Sensory receptors (in aortic and carotid sinuses) responds 3) Regulatory center in brain responds 4) Arterial walls constrict to increase blood pressure and removing low pressure signal 5) Blood pressure rises 6) Removes stimulus (if not, go back to step 2) |
|
|
Explain positive feedback of hypothalamus's hypothalamic hormone release: |
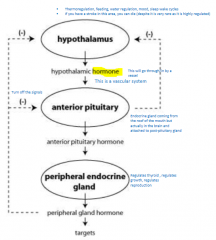
1) Hypothalamus will create hypothalamic hormone (this go through/in by a vessel as this is a vascular system)
2) Hypothalamic hormone interact with anterior pituitary (this can inhibit hypothalamus release of hypothalamic hormone) causing release of anterior pituitary hormone 3) Anterior pituitary hormone will interact with peripheral endocrine gland (this regulates thyroids, growth and reproduction) which releases peripheral gland hormone (which can inhibit release from hypothalamus and anterior pituitary) and reach its target |
|
|
What happens if you have a stroke in the hypothalamus? |
Though it is very rare as it is highly regulated, you can die from it |
|
|
Explain the positive feedback of oxytocin and control of uterine contractions: |
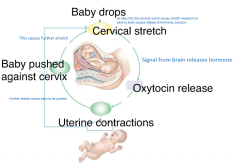
1) Baby drops (as baby hits cervices, this cause stretch receptors to send to brain causes release of hormone: oxytocin) 2) Cervical stretch which signal brain to release hromones 3) Oxytocin released 4) Causes uterine contractions (if baby pushed out, this inhibits the cervical stretch, step 2, and stops the feedback loop) 5) Causes further stretch and baby being pushed against cervix (repeat from step 2) |
|
|
Imagine a hormone that is released in response to low blood pressure and acts to reduce blood pressure. What is this an example of? a) Positive feedback b) Negative feedback c) Feed forward control d) Neutral feedback |
a) Positive feedback
|
|
|
What are the three forms of intercellular/local communcations for maintaining homeostasis? |

1) Gap junctions: Allows transfer of ions, ATP and different substances Allows rapid communication between cells to allow cells to contract at same time Form direct cytoplasmic connection between adjacent cells 2) Contact-dependent signals Require interaction between membrane molecules on two cells 3) Autocrine signals and paracrine signals Autocrine signals act on same cell that secreted from Paracine signals are secreted by one cell and diffuse to adjacent cells |
|
|
What is the form of long-distant communcation in the endocrine system? |

Hormones are secreted by endocrine glands or cells into the blood. Only target cells with receptors for the hormone respond to the signal |
|
|
What are the two form of long-distant communcation in the nervous system? |
1) Neurotransmitters: Chemicals secreted by neurons that diffuse across the gap to target cell 2) Neurohormones: Chemicals released by neurons into the blood for action at distant targets (degrade really quickly) |
|
|
What is FLAT PEG? |
It is an acronym to remember the hormones released from the pituitary gland: FSH (follicle-stimulating hormone) LS (lichen sclerosus) ACTH (adrenocorticotropic hormone) TSH (throid-stimulating hormone) PROLACTIN (can cause milk production in males if not inhibited) ENDODROPHIN GH (growth hormone) |
|
|
What are the two ways endocrine glands secrete hormones into the blood stream? |
Once epithelium connective tissue go through division, they can either do: 1) Exocrine into duct Goes to a specific space/through specific substrate 2) Endocrine into bloodstream Sitting in a gland as one epithelium |
|
|
What would you expect to observe in a mouse transgenically over-expressing OPG? |
Harder for parathyroid hormone to exert its effect on bone |
|
|
Bill decided to drink a sports drink with a high concentration of salt (a hypertonic solution). What physiological responses would you expect to observe? |
Vasopressin would be released from the posterior pituitary |
|
|
Which of the following is a step in the intracellular mechanisms involved in the stimulation of insulin secretion by glucose? A.Glucose moves into the beta cells against its concentration gradient B.The beta cell depolarizes triggering the opening of voltage-gated calcium channels C.ATP binds to K+ channels in the plasma membrane of the beta cell and causes them to open D.The ratio of ADP to ATP in the beta cell increases |
B.The beta cell depolarizes triggering the opening of voltage-gated calcium channels |
|
|
What would you observe in the liver of someone experiencing a flight or fight response? |
Glycogen synthase inactive |
|
|
Which one of the following statements concerning the spinal reflexes is incorrect? A) The golgi tendon reflex is mediated by type 1b afferents B) The stretch reflex is active during movement C) The golgi tendon reflex is polysynaptic D) The stretch reflex is mediated by muscle spindle afferents |
B)
|
|
|
Which one of the following would not be considered an orexigenic signal to the hypothalamus or brainstem?
A) PYY
B) ghrelin
C) activation of melanocortin containing neurons in the arcuate nucleus
D) stimulation of glucose receptors in the ventral median nucleus of the hypothalamus |
A)
|
|
|
If a student has stimulated her maculae, which one of the following most likely occurred? A) She nodded her head B) She rotated her head C) Her malleus was activated D) She heard a noise |
A
|
|
|
Where would the neurons responsible for light/dark luminance and darkness detection used in thepupillary light reflex send their projections? A) Olivary pretectal nucleus B) Periaqueductal gray C) Suprachiasmatic nuclei D) Ciliary ganglion |
A
|
|
|
Which one of the following has been most closely associated with olfactory densensitization in thecontinued presence of an odorant? A) Elevated cAMP B) Elevated G‐olf C) Elevated Ca2+ D) Elevated Na+ |
C
|
|
|
Which of the following directly influences the activation of the extensor thrust? A) Vestibulospinal tract B) Corticospinal tract C) Rubrospinal tract D) Spinocerebellar tract |
B
|
|
|
Which one of the following would most likely be involved in directly and tonically inhibiting thepremotor thalamus? A) Pallidum B) Striatum C) Superior colliculus D) Substantia nigra |
A
|
|
|
A patient comes in complaining of “uncinate fits”. What sensory system is most likely affected? A) Gustatory (taste) B) Vestibular C) Hearing D) Olfactory |
D
|
|
|
Which one of the following are the output cells found in the cerebellar cortex that allows for finemotor control? A) Purkinje B) Rubrospinal C) Granule D) Betz |
A
|
|
|
Where would the cell bodies of sympathetic nervous system neurons be located? A) Dorsal column of the lumbar region of the spinal cord B) Lateral funiculus of the spinal cord C) Intermediolateral gray of the spinal cord D) Ventral horn of the spinal cord |
C
|
|
|
Which of the following reflexes would be activated by tilting of the head sideways while walkingdownhill via activation of the otolith afferents?
A) Crossed extension
B) Propiospinal
C) Vestibulocular
D) Vestibulospinal |
D) |
|
|
Which one of the following does not accurately represent parts of the autonomic nervous system? A) Sympathetic: maintenance of blood pressure: activated in baroreflex B) Sympathetic: preganglionic release of Ach: postganglionic release of Noradrenaline C) Parasympathetic: thoracolumbar origins : long myelinated preganglionic axons D) Parasympathetic: preganglionic release of Ach: involved in pupil constriction when bright |
C
|
|
|
In smooth muscle, what is the small protein chain that regulates contraction and relaxation? A) calcium B) myosin heavy chain C) myosin light chain D) actin |
C
|
|
|
Which one of the following would not be directly associated with neurons found in the intermediatezone of the spinal cord? Choose the most appropriate response A) Commissural interneurons B) Postsynaptic inhibition C) Crossed extension reflex D) Flexion withdrawal reflex |
B
|
|
|
Which cells in the olfactory system are involved in relaying action potentials to the olfactory cortex? A) Olfactory receptor cells B) Amacrine granule cells C) Mitral cells D) Amacrine cells |
C
|
|
|
Where would the central pattern generators (CPGs) involved in body trunk control during locomotion most likely be found?
A) Globus pallidus
B) Mesencephalic locomotory region (MLR)
C) Locus coeruleus
D) Brainstem reticular formation |
D
|
|
|
Which one of the following areas in the brain would most likely become activated if levels of adenosine in the hypothalamus rise during the day?
A) pineal body
B) ventrolateral preoptic nucleus
C) tuberomamillary nucleus
D) suprachiasmatic nucleus |
B
|
|
|
Which one of the following ion(s) would have the greatest impact on depolarizing the inner hair cellsof the Organ of Corti following their displacement against the tectorial membrane? A) Ca2+ B) K+ C) Na+ D) All of the above |
B
|
|
|
Which one of the following structures would be involved in cholinergic modulation of the autonomicnervous system? A) Locus coeruleus B) Medial septal nuclei C) Tuberomamillary nucleus D) Brainstem Raphe nuclei |
B
|
|
|
Which one of the following statements about hearing a low frequency sound would be the mostaccurate? A) There would be maximal displacement of the basilar membrane near the round window B) There would be maximal displacement of the basilar membrane near the oval window C) The entire basilar membrane would be equally displaced along its entire length D) There would be maximal displacement of the basilar membrane near the helicotrema |
D
|
|
|
Which one of the following areas would be involved in mediating the baroreflex directly? A) reticular formation in the pons B) paraventricular nucleus of the hypothalamus C) base of the hypothalamus D) Brainstem ventrolateral medulla |
D
|
|
|
Identifty the incorrect statement regarding the neuromuscular junction of skeletal muscle A) ACh binding triggers opening of Ca2+ channels B) All motor neurons release acetylcholine C) ACh diffuses across cleft and binds to nicotinic receptors on motor end plate D) All synapses are excitatory |
A
|
|
|
When comparing complete tetanus with unfused tetanus, which is true? A) In complete tetanus, no relaxation occurs between stimuli. B) In complete tetanus, maximum tension is developed. C) In complete tetanus, the muscle fiber is stimulated at a higher frequency. D) All of the above |
D
|
|
|
Factor A causes the release of factor B. Factor B causes the release of factor C. Factor C inhibits bothfactors A and B. If Factor A, B and C are all abnormally high, what could possibly be going on? A) Factor B cells are creating abnormally high levels of factor B and not responding to any outside factors B) The cells that release Factor A are creating abnormally high levels of factor A and these cells are notresponding to any outside factors C) Factor C is being created at abnormally high levels and factor C producing cells are not responding tooutside stimuli D) This is an example of homeostasis working correctly |
B
|
|
|
As ATP binds to the myosin head at the beginning of a muscle contraction cycle, A) ATP does not bind to the myosin head. B) the myosin head tightens its bond to actin. C) the myosin head initiates binding with actin. D) the myosin head detaches from actin. |
D
|
|
|
The purpose of transverse tubules is to A) ensure a supply of Ca2+ ions through the muscle fiber. B) ensure a supply of glycogen throughout the muscle sarcoplasm. C) rapidly conduct action potentials to the interior of the muscle fiber. D) conduct ATP molecules out of the mitochondria throughout the sarcoplasm |
C |
|
|
What are the three main types of hormones? |
Peptide/protein (3 or more amino acids, most common) Steroid (derived from cholesterol) amine (derived from single amino acids) |
|
|
What are peptide/protein hormones? |
They are the most common type of hormone Made in advance Synthesized like secreted proteins Stored in vesicles Release by exocytosis upon a signal (released on demand, released by Ca+ hormones) Water soluble (dissolved in plasma, hydrophilic which means not cross cell membrane which means acts at cell membrane) Short half life (because protein released into the blood and seeks and broken down, unstable and when binds to receptors, they are internalized and digesting after one use) Bind to membrane receptors |
|
|
What are the three parts of peptide/protein hormone production? |
All protein/peptide hormones are coded by genes 1) Signal sequence Tell you where to go and then dropped off Genes are transcribed into mRNA, translated in cytosol and ribosome detects the ER signal sequence 2) Prohormone Signal sequence gets cleaved, hormone will get transported to Golgi complex to get modified Gets stored into a secretory vesicle which leads to sorting/peptide fragment 3) Sorting/peptide fragment Get separated from peptide fragment into two components Not always the case but often |
|
|
What are some of the active hormones does the prohormone pro-opiomelanocortin (POMC) process to? |
ACTH (involved in cortosil production) Gamma lipotropin Beta endorphin |
|
|
What is alpha-MSH involved in and what does MSH stand for? |
Apetite (inhibit food intake) and skin activating melanocytes Melanocyte stimulating hormone |
|
|
What is beta-lipotropin involved in? |
Pain relief |
|
|
POMC production is inhibited by Factor A. POMC produces proteins that increase skin pigmentation which darkens skin, increase blood sugar, relieve pain and decreases appetite. The gland that produces Factor A s no longer working in John. What might we see happen to John? |
Darkening of skin |
|
|
Outside measuring a lot of ACTH, how can you tell if there is a lot of ACTH? |
If you see a lot of ACTH, you would see a lot of alpha-MSH |
|
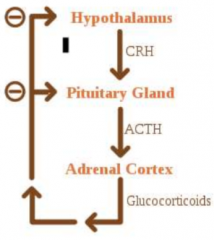
In this system, what would happens if you shut down the pituitary gland? |
There will be an increase of CRH |
|
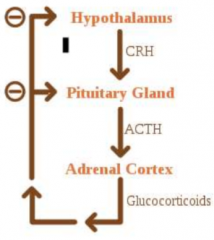
In this system, what would happen if you take away glucocorticoids? |
Increase/a lot of ACTH and CRH as there is no inhibition |
|
|
How are two mature insulin peptide chains bonded? |
By disulphide bonds |
|
|
For insulin, what is C-peptide? |
The "inactive" fragment that is cleaved from proinsulin |
|
|
Insulin is degraded in the body extremely quickly and is difficult to measure because of this. How else could we indirectly measure insulin release? |
Measure C-peptide levels Can be argued to measure preproinsulin peptides but that would be difficult to do in humans |
|
|
What are steroid hormones? |
Synthesized only from cholesterol Made on demand Released from cell by simple diffusion Water insoluble (bounds to carriers in blood) Long half-life Binds to cytoplasm or nucleus receptors (but in some cases, also act on plasma membrane receptors) |
|
|
What is the starting molecule of aldosterone, cortisol, estriol, etc...? |
Cholesterol When one of the transforming enzymes is blocked, that specific hormone product cannot be produced and something else will be produced |
|
|
What is aldosterone important for? |
Sodium pretention |
|
|
What does aldosterone synthease do? |
Turns corticosterone to aldosterone Seen in the adrenal gland |
|
|
How do you determine which hormone is produced? |
It is dependent on the cell type as the cell type will express the enzyme of interest |
|
|
The 21-alpha-hydroxyalase enzyme is no longer working in John. What may you see happen in this person? |
Increased production of androgens |
|
|
What are amine hormones? |
Synthesized only from tryptophan or tyrosine Example of tryptophan derivative: - Melatonin (behaves like peptides or steroids) Examples of tyrosine derivatives: - Catecholamines (behave like peptides, water soluble, have membrane receptors, can act as neurotransmitters) - Thyroid hormones (behave like steroids, diffuse into cells, carrier proteins in blood that are long lasting) |
|
|
What is melatonin? |
Darkness hormone Secreted at night (Sleep) Made in pineal gland (also gi tract, leukocytes, other brain regions) Receives light information from eyes Diverse effects: - Transmits information (light-dark cycles to govern biological clock) - Immune modulation - Anti-oxidant |
|
|
Where does the synthesis of catecholamines taken place? |
Synthesized in adrenal medulla (mainly in cytosol) Stored in vesicles prior to release (released in adrenal gland) |
|
|
Explain the glucose stimulation of insulin release: |

1) High concentration of glucose transported into the pancreatic beta cell which triggers glycolysis and cellular respiration 2) ATP is made since glucose is coming into the cell 3) ATP binds to K channel, causing it to close 4) More positive charge builds up, causing depolarization, triggering opening of calcium channels causing calcium to come into cell 5) The calcium acts on stored vesicles and releases insulin (triggers exocytosis of vesicles) |
|
|
Glucose that enters beta cells cause the release of insulin by increasing cellular ATP levels which close K-ATP sensitive channels. This leads to cell depolarization and opening of voltage gated channels. An insulin causes body wide uptake of glucose, what is this an example of? |
Negative feedback |
|
|
Sulfonylurea blocks K_ATP channels, what effect would this have? A) Keeps voltage-gated Ca2+ channels closed B) Enhances insulin secretion C) Cause the cell to hyperpolarize D) Directly reduces the levels of ATP in the cell |
B) Enhances insulin secretion |
|
|
In the anterior pituitary, what are portal vessels? |
Carry the trophic hormones directly to the anterior pituitary |
|
|
What are endocrine cells? |
They release their hormones into the second set of capillaries for distribution to the rest of the body |
|
|
What do GHRH target and what hormone does it effect? |
GHRH = GH releasing Hromone Target cell: Somatotrope Causes stimulation of GH |
|
|
What do SRIF (Somatostatin) target and what hormone does it affect? |
Target cell: Somatotrope Causes inhibition of GH OR Target cell: Thyrotrope Causes inhibition of TSH |
|
|
What do Dopamine target and what hormone does it affect? |
Target: Lactotrope Causes inhibition of PRL |
|
|
What does TRH target and what hormone does it affect? |
TRH = Thyrotropin releasing hormone Target cell: Lactotrope Causes stimulation of PRL OR Target cell: Thyrotrope Causes stimulation of TSH |
|
|
What does GnRH target and what hormone does it affect? |
GnRH = Gonadotropin releasing hormone Target cell: Gonadotropes Causes stimulation of FSH and LH |
|
|
What does CRH target and what hormone does it affect? |
CRH = Corticotropin Rel. Hormone Target cell: Corticotrope Causes timulation of ACTH |
|
|
When Vasopressin (ADH) is released at nerve terminals, what is the target tissue? |
Kidney, vasculature |
|
|
When Oxytocin is released at nerve terminals, what is the target tissue? |
Mammary gland, uterus |
|
|
What determines the amount of active hormone in the plasma? |
Hormone being release, its going into blood, going to bind to carriers and diffuse off of carriers into target cells Depends on pre-hormone concentration and number of receptors present on target cell Hormones is going to be metabolized as go through liver and kidney (by excretion in urine) |
|
|
How are hormones detected/measured? |
Hormones are exceptionally potent chemicals (nanomolar to picomolar) Hormone measurements (sensitive method): immunoassay and immunohistochemistry Both use antibodies that specifically bind to part of the hormone |
|
|
What is immunoassay? |
Tagged antibody specific to hormone (detection in blood and urine) Use antibodies that specifically bind to part of the hormone |
|
|
What is immunohistochemistry |
Detection in tissue Use antibodies that specifically bind to part of the hormone |
|
|
How do hormones signal? |
Hormone binds to receptor (primary ligand, agonist, antagonist) Changes the conformation and activity of the receptor Alters activity of intracellular signaling pathways Leads to change in synthesis of target proteins and/or modification of existing target proteins There can be hydrophobic hormones where binds to both intracellular and membrane receptors There can be hydrophilic hormones which are water soluble hormones that bind to plasma membrane receptors |
|
|
What are the properties of hormone receptors? |
High affinity (strong interaction for binding of receptor and hormone) Saturable (can reach a point where all receptors are bounded to a hormone) Specific (if receptor is modified, than the ligand will have less affinity to the receptor or won't bind at all) Reversible (binding is reversible, no covalent interactions, hormones can dissociate from the receptor) |
|
|
Hormone A binds to receptor B which causes response C. The concentration of hormone A doubles in the body causing a doubling in response C. The concentration of hormone A doubles again, but this time no change in response C. What could be happening? |
Receptor B is saturated |
|
|
What are the two main types of hormone receptors? |
Intracellular receptors (bind lipid soluble hormones) Plasma membrane receptors |
|
|
Explain how intracellular receptors work: |

1) Hydrophobic hormone will diffuse into the cell and bind to either cytoplasmic receptor (exposing a nuclear localization signal on receptor and goes into nucleus) or onto a nuclear receptor 2) Bind to HRE (a specific DNA sequence that recognizes the complex but remember, some genes don't have HRE) 3) Complex would act as a gene regulatory protein, having some effect on transcription of a subset of genes found in nucleus) End result is a decrease or increase in transcription and increase or decrease in protein production |
|
|
What are HRE? |
Hormone response elements They are specific DNA sequences that will increase or decrease gene transcription Sometimes receptors recruit co-repressors to inhibit transcription Only genes with the response elements will be activated/repressed |
|
|
What is the most common type of hormone receptor? |
GPCR |
|
|
What is G_as? |
It is a stimulatory G-protein alpha subunit |
|
|
What is G_ai? |
An inhibitor G-protein alpha subunit |
|
|
What is G_aq? |
A phosphorator G-protein alpha subunit |
|
|
How does G_as activate adenyly cyclase? |
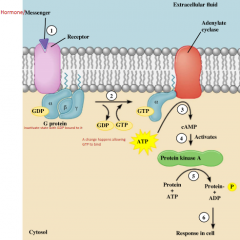
1) When hormone binds to receptor, it causes change in the receptor and causes alpha subunit of G-protein to change its conformation 2) When that happens, GDP binds to the alpha subunit in exchange for GTP (so GDP falls off, GTP binds) 3) When that happens, the beta and gamma subunits dissociates from the alpha subunit (now just left with alpha subunit) 4) The alpha subunit then interacts with adenylate cyclase (in this case) which converts ATP into cAMP (cyclic AMP) 5) That then binds to the enzyme Protein kinase A which uses specific substrates (proteins found in cell) and phosphorylates it 6) When proteins are phosphorylated, it changes its shape and hence it changes its activity and creates response |
|
|
What is an advantage of using a G-protein receptor? |
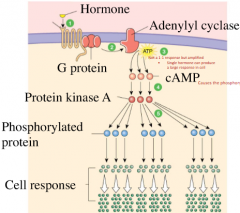
You don't have to have very much of a hormone to have an amplification effect G-protein activates the adenylyl cyclase BUT it can make lots of cAMP Lots of cAMP can be made which then binds to many protein kinase A which acts on different substrates |
|
|
Describe cAMP formation and breakdown: |

Formation: Of ATP, two phosphates are cut of to create a cyclic structure called cAMP Breakdown: cAMP phosphodiesterase breaks the bond to create 5' AMP, turning off hormone signaling |
|
|
What is cAMP phosphodiesterase? |
It breaks the bond of cAMP to create 5' AMP |
|
|
How does G_aq activate phospholipase C? |

1) Signal molecule activates receptor and associated G-protein 2) G-protein activates phospholipase C (PL-C), an amplifier enzyme 3) PL-C converts membrane phospholipids into diacylgycerol (DAG) which remains in the membrane, and IP3, which diffuses into the cytoplasm 4) DAG activates protein kinase C (PK-C) which phosphorylates protein 5) IP3 causes release of Ca++ from organelles, creating a Ca++ signal |
|
|
What is the fight or flight response in the liver, fat, heart, skeletal muscles/blood vessels, and intestine/skin/kidney? |
Liver: glucose release Fat: fatty acid release Heart: muscle contraction Skeletal muscle/blood vessels: Less vasoconstriction, less blood to artery Intestine/skin/kidney: vasoconstriction |
|
|
What adrenergic receptors would you use if you want your arteries to dilate? |
Beta-1 Beta-2 |
|
|
What adrenergic receptors would you want to use if you want your arteries to constrict? |
Alpha-2 |
|
|
What happens when a specific hormone binds to a beta-1 or beta-2 adrenergic receptor? |
G_as which stimulates adenylate cyclase, producing cAMP, activating protein kinase leading to protein phosphorylation causing target cell response |
|
|
What happens when a specific hormone binds to a alpha-2 adrenergic receptor? |
G_ai which inhibits or causes a decrease response of adenylate cyclase |
|
|
What happens when a specific hormone binds to a alpha-1 adrenergic receptor? |
G_aq which stimulates phospholipase C |
|
|
Does epinephrine increase of decrease glycogen breakdown?
|
Epineprhine increases glycogen breakdown and decreases its synthesis It increases blood glucose |
|
|
Insulin activates what pathway? |
The PI3K/MAPK pathway |
|
|
Describe the insulin receptor: |
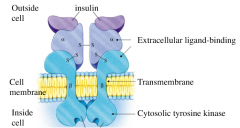
It is a receptor enzyme that is also a transmembrane receptor Has 2 subunits Insulin binds to change conformation of cytosolic portion which is an enzyme on its own (tyrosine kinase) Tyrosine kinase phosphorylates specific tyrosine on other proteins and can even phosphorylate itself and other signaling molecules |
|
|
What is tyrosine kinase? |
Found on/in the insulin receptor Tyrosine kinase phosphorylates specific tyrosine on other proteins and can even phosphorylate itself and other signaling molecules |
|
|
What happens when insulin activates the Ras-MAP kinase signaling pathway? |
Insulin receptor is bound to insulin Phosphate groups attached to cytosolic portion IRS-1 binds to the phosphate, it gets phosphorylated it can recruit Which binds to phosphorylator receptor and that recruits Grb2, then SOS which activates enzyme Ras, which phosphorylates Raf, which phosphorylates MEK, which phosphorylates Erk and that causes regulatory proteins to create change in protein sythesis |
|
|
What happens when insulin activates the PI-3 kinase/protein kinase B pathway? |
Insulin receptor is bound to insulin Phosphate groups attached to cytosolic portion IRS-1 binds to the phosphate, it gets phosphorylated it can recruit other enzymes to area and activate them PI3-kinase which then phosphorylates PIP3 Then it brings other enzymes (PKB, PDK1) to the area Then PKB, PDK1 regulate glycogen synthesis, glucose transport and suppress cell death |
|
|
How is signalling modulated? |
Hormone degraded Receptor down-regulation or upregulation Receptor desensitization Breakdown of second messengers Modification of any component in the pathway Biological effect provides feedback to reduce hormone secretion |
|
|
Put the step of signal transduction in order: 1) Creates response 2) Activates a protein 3) Ligand binds to receptor 4) Creates second messengers |
3, 2, 4, 1 |
|
|
Epinephrine released from the medulla in response to sympathetic activation can cause both vasodilation and vasoconstriction of arteries, how is this possible? |
Epinephrine can work on multiple receptors causing different physiological responses |
|
|
Hormone A binds to a G-protein coupled receptor that has a G_as subunit. What can we expect to see happen inside this cell? |
Increase in cAMP |
|
|
Which function is not true: A) Insulin release will reduce blood glucose B) Epinephrine will increase blood glucose from the liver C) Intracellular receptors primarily work through cell signaling D) Epinephrine can cause both vasodilation and vasoconstriction |
C) Intracellular receptors primarily work through cell signaling |
|
|
What are the three hormones that control Ca++? |
Parathyroid hormone (increase Ca++) Calcitriol/Vit D3 (increases Ca++ which happens at bones, kidneys and digestive tract) Calcitonin (decreases Ca++) |
|
|
Why is calcium critical for normal physiology? |
Intracellular signaling Hormone secretion Blood clotting Neural excitability and muscle contraction Building and maintaining bone |
|
|
Which cells are responsible for bone growth/turnover? |

Osteoblast (bone forming) Osteocyte (maintain matrix) Osteoclast (bone resorption by taking bone and depositing it into the extracellular fluid) |
|
|
Via what does the osteoclast use to break down bone? |
Acid and enzymes |
|
|
What does the osteoblast promote? |

It promotes osteoclast formation via RANKL/RANK interaction (MPT) Osteoblast will have RANKL which will work with the receptors on the osteoclast precursors RANK (communication between osteoclast and osteoblasts) causing differentiation and fusion to form osteoclasts. |
|
|
What does RANK do? |
Found on osteoclast precursors It is a receptor activator of nuclear factor kappa B which works with RANKL of osteoblast to cause osteoclast to differentiation and fuse into an osteoclast |
|
|
What does RANKL do? |
Found on osteoblasts It is a RANK ligand Essential for osteoblast to be reduced which results in bone respiration A stimulus comes to osteoblast, telling RANKL to make for bone |
|
|
What is OPG? |
Osteoprotegerin Secreted by osteoblasts Black RANKL/RANK interactions |
|
|
The RANKL/RANK/OPG system was discovered in the late 1990s. If you were an employee of a biotechnology company at that time, how might you have used this knowledge to develop a drug for treating osteoporosis? An effect drug might: |
Mimic effect of OPG |
|
|
What is osteoporosis? |
A medical condition in which the bones become brittle and fragile from loss of tissue, typically as a result of hormonal changes, or deficiency of calcium or vitamin D |
|
|
What is the hormone PTH? |
Parathyroid hormone Senses calcium levels and when calcium is low, PTH will be released, which acts of three targets: bone, kidney and digestive system. With the bone, you can increase calcium from bone into extracellular fluid through osteoclast, telling osteoblast to increase RANKL expression. PTH can work on osteoblast to increase osteoclast activity Released from parathyroid glands (chief cells) Its function is to increase plasma Ca++ concentration Its stimulus is low plasma Ca++ (if you remove PT gland, you can cause calcium deficiency called hypocalcemia) |
|
|
What is the stimulus of PTH? |
Low plasma Ca++ |
|
|
What is hypocalcemia |
Calcium deficiency |
|
|
How sensitive are the parathyroid cells to changes in extracellular calcium concentration |
They are exquisitely sensitive Calcium needs to be maintained in a very narrow range With very small changes, you will have changes in PTH |
|
|
What is used to monitor extracellular Ca++? |
Ca++-sensing receptor on plasma membrane
When Ca levels are high, through multi-signaling pathways, they decrease PTH release
When Ca levels are low, you will not have stimulus
This is a negative feedback
When Ca++ binds to the receptors, G-proteins activated, adenylyl cyclase inhibited, phospholipase C activated, PTH secretion (synthesis) is inhibited |
|
|
How does PTH increase plasma [Ca++] in intestine? |
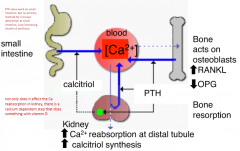
PTH work on small intestine Primary method for increasing absorption at small intestine by increasing vitamin D synthesis |
|
|
How does PTH incraese plasma [Ca++] in kidneys? |
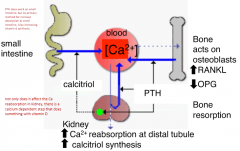
Ca++ reabsroption at distal tubule increase Calcitriol synthesis increase Decrease phosphate reabsroption at proximal tubule |
|
|
How does PTH effect bones? |
PTH acts on osteoblast by increase cAMP to increase RANKL and decrease OPG expression More ostoclasts are formed leading to bone resorption |
|
|
What 3 organs are crucial in development of calcitriol? |
Skin Liver Kidney Vitamin D through multiple enzymatic steps create calcitriol |
|
|
What does calcitriol target? |
Intestines, bones and kidney to increase serum calcium |
|
|
What happens when calcitriol binds to vitamin D nuclear receptor |
Increases expression of calcium channels/binding proteins/transporters in kidney and intestine as well as RANKL and OPG in osteoblasts Also increase plasma Ca++ |
|
|
How do hormones correct a calcium deficit? |
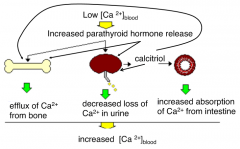
|
|
|
What are three ways that PTH can raise plasma Ca++? |
1) PTH mobilizes calcium from bone: osteoclasts via RANKL and OPG mechanisms 2) PTH enhances renal reabsroption of Ca++ 3) Calcitriol - PTH enchances the production of Calcitriol |
|
|
What is calcitonin? |

Secreted from C cells of the thyroid gland Calcitonin is a peptide hormone Release triggered by high plasma Ca++ concentrations C cells also have Ca++ sensing receptors |
|
|
What are the actions/roles of Calcitonin? |
"Tones down" calcium levels Protect the skeleton from Ca++ loss during pregnancy and lactation Reduces activity of osteoclasts (inhibits bone resorption) Stimulates osteoblasts and deposit calcium Inhibits calcium reabsorption by kidneys |
|
|
How does PTH increase phosphate secretion? |
PTH increases Ca+ reabsroption at the level of the kidney causing phosphate secretion This done so you can avoid developing a high concentration of calcium and phosphate which can develop stops |
|
|
How does Vitamin D increase phosphate levels? |
Does it at the level of the kidney as well at the same time increase Ca++ levels |
|
|
Kramer comes into your office and tells you he has bone pain, abdominal pain and recently passed a kidney stone. You do blood work in your office and see he has high calcium and high phosphate levels. Hormone testing is yet to come back. What might you expect on to see? |
High vitamin D |
|
|
Jerry presents to your office after having a blood test. His values are as follows: Ca++ 3.0 (high) PTH 20 (high) What is the likely source of his abnormal blood values? |
PTH secreting tumor |
|
|
Which organ is not crucial in the processing of Vitamin D to Calcitriol? A) Skin B) Kidney C) Pituitary gland D) Liver |
C) Pituitary gland |
|
|
Which statement is false? A) PTH acts directly on osteoclasts to increase Ca++ resoprtion B) PTH increases Ca++ through multiple mechanisms C) PTH is secreted from 4 glands on thyroid D) PTH is involved with calcitriol synthesis |
A) PTH acts directly on osteoclasts to increase Ca++ resoprtion
|
|
|
How are daily water intake and excretion balanced? |
Intake + (Metabolic production) = Output |
|
|
What do podocytes modulate? |
Modulate and allow the extent of filtration |
|
|
What does the mesengial matrix contribute to? |
Filtration |
|
|
Give an example of how the afferent and efferent work in tandem for the kidney: |
Afferent constricts, efferent dilates to reduce filtration |
|
|
What does the macula densa of the kidney do? |
When low blood pressure sensed, your body will try to increase blood pressure If blood pressure is too high, you will release enzymes to increase filtration |
|
|
How is urine formed in the nephron? |
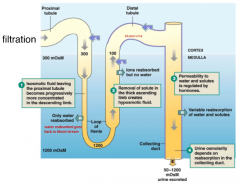
By filtration, reabsorption and secretion 1) Isomotic fluid leaving the proximal tubule becomes progressively more concentrated in the descending limb 2) Removal of solute in thick ascending limb creates hyposomotic fluid 3) Permeability to water and solutes is regulated by hormones 4) Urine osmolarity depends on reabsorption in the collecting duct |
|
|
How do hormones regulate water, Na+ and K+ balance? |
1) Vasopressin Comes from posterior pituitary, important for keeping water Increases H2O reabsorption 2) Aldosterone Comes from adrenal gland, important for keeping Na Increases Na+ reabsorption Increases K+ secretion 3) Atrial natriuretic peptide Get rid of Na and H2O when there is a lot of stretch in atria Decreases Na+ and H2O reabsorption Increase K+ reabsorption |
|
|
Where is Vasopressin (antidiuretic hormone, ADH) synthesized and secreted? |
Synthesized in hypothalamus Secreted from posterior pituitary |
|
|
Explain regulation of vasopressin release: |
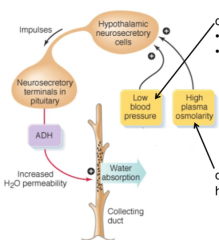
When there is low blood pressure (detected by reduced stretch of walls of atria of heart or aortic and carotid arteries) and/or high plasma osmolarity (detected by osmoreceptors in hypothalamus) Stimulate hypothalamic neurosecretory cells Sends impulses to neurosecretory terminals in piuitary which causes release of ADH This causes increase H2O permeability, stimulating water absorption in collecting duct leading to lower osmolality |
|
|
Can angiotension 2 stimulate ADH release? |
Yes |
|
|
What is the most potent stimulus for vasopressin release? |
Osmolarity |
|
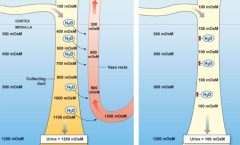
Which panel shows what happens in the presence of vasopressin? |
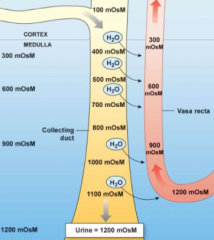
Left |
|
|
Dave consumes a large size pack of salty potato chips. What would you expect to observe in response? A) Decreased release of vasopressin B) Production of large volume of salty urine C) Decreased cAMP in collecting duct cells D) Aquaporins moving to apical membranes |
D) Aquaoporins moving to apical membranes |
|
|
What is aldosterone? |
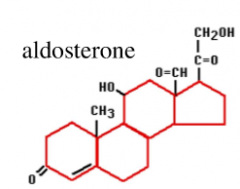
A steroid synthesized in the adrenal cortex Causes Na+ reabsorption (retain water), K+ secretion and acts on distal tubule and collecting duct (which prevents degradation of apical Na+ channels, increases expression of Na+ and K+ channels and Na+/K+ ATPase) |
|
|
What happens when aldosterone acts on distal tubule and collecting ducts? |
Prevents degradation of apical Na+ channels Increases expression of Na+ and K+ channels and Na+/K+ ATPase |
|
|
Aldosterone synthesis is what type of feedback and what is its simulators and inhibitors? |
Negative feedback Stimulator: High K+ concentration in plasma and Angiotensin 2 Inhibtor: High osmolarity in extracellular fluid |
|
|
What is renin and where is it secreted from? |
Renin is an enzyme involved in controlling aldosterone release Secreted from Renal juxtaglomerular (juxta) cells |
|
|
Dave decides to donate blood, which results in blood pressure. What would be observed in Dave during after the blood donation? A) Aldosterone synthesis will increase B) Kidneys will secrete water and salt C) Levels of angiotensinogen will increase D) K+ reabsorption will increase |
A) |
|
|
What are the three families/types of natriuretic peptides? |
ANP BNP CNP |
|
|
Where is the natriuretic peptide ANP expressed? |
Atria and brain |
|
|
Where is the natriuretic peptide BNP expressed? |
Ventricles and brain |
|
|
Where is the natriuretic peptide CNP expressed? |
Brain, pit, vessels and kidneys |
|
|
Which of the following is a correct match hormone and transport location? A) Aldosterone + aquaporin collecting duct B) Vasopressin + aquaporin collecting duct C) Angiotensinogen + aquaporin distal tubule D) Renin + aquaporin loop of henle |
B)
|
|
|
Vasopressin/ADH is produced in which structure? |
Hypothalamus |
|
|
Aldosterone is directly stimulated by? |
Angiotensin 2 |
|
|
What is insulin secreted in response to and what can it decrease and promote? |
Secreted in response to glucose, GLP1, PNS and amino acids Decreases blood glucose Promote anabolic pathways |
|
|
What is glucagon secreted in response to and what can it increase? |
Secreted by alpha cells in response to low glucose, SNS and amino acids Increase blood glucose, gluconeogensis, glycogenolysis and through the catabolic pathways, increase energy |
|
|
What is GLP-1 released in response to, stimulate, increase and decease? |
Released from intestine in response to glucose and amino acids Stimulates insulin secretion Increase beta cell mass Decrease glucaagon |
|
|
What is Basal Metabolic Rate (BMR)? |
An individual's energy expenditure when resting, comfortable temperature, fasted |
|
|
What is metabolism? |
Sum of all chemical reactions in the body Nutrients stored or energy extracted to be used for work Two states: 1) Fed, absorptive, anabolic (use glucose for energy) 2) Fasted, psotabsorptive, catabolic (use glucose, fat for energy) |
|
|
What is gluconeogenesis? |
Synthesis of glucose from non-carbohydrate substrates such as glycerol and amino acids |
|
|
One hour after a person has eaten a meal, which of the follow would you expect to observe? A) Gluconeogenesis in the liver B) Lipolysis in fat cells C) Protein synthesis in muscle cells D) Glycogenolysis in the liver |
C) |
|
|
What hormone does exocrine (acinar) cells secret? |
Zymogen
|
|
|
What hormone does delta-cells secret? |
Somatostatin (inhibits alpha and beta cells) |
|
|
What hormone does alpha-cells secret? |
Glucagon |
|
|
What hormone does beta-cells secret? |
Insulin (and c-peptides) |
|
|
What does the insulin-to-glucagon ratio control? |
Glucose homeostasis Glucagon low, insulin high Glucose dips, release of glucagon |
|
|
What is the dominant hormone of the fed state? |
Insulin (anabolic) Synthesized as a typical petide Binds to a receptor tyrosine kinase Reduces blood glucose Promotes formation of glycogen, fat and protein |
|
|
What are the effects of insulin? |
Increase glucose transport into insulin-sensitive cells Activates enzymes involved in glycolysis, glycogenesis, lipogenesis Inhibits enzymes for glycogenolysis, gluconeogensis and lipolysis Increases uptake of amino acids into muscles and protein synthesis Promotes lipogenesis and inhibits beta oxidation Enhances cell proliferation |
|
|
What happens to GLUT4 when insulin binds to an insulin receptor on the plasma membrane of a cell? |
1) Insulin binds to receptor 2) Signal transduction cascade will occur with a GLUT4 transporter protein on a secretory vesicle 3) Exocytosis causing GLUT4 to be part of plasma membrane 4) Glucose enters cell by GLUT4 |
|
|
What does hexokinase do? |
Activated by insulin, it maintains a high glucose concentration gradient Hexokinase-mediated conversion of glucose to glucose-6-phosphate which keeps intracellular glucose concentrations low |
|
|
What is the pathway which stimulates insulin release? |
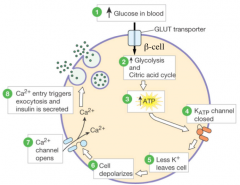
1) Increase of glucose in blood
2) Increase of glycolysis and citric acid cycle 3) Increase of ATP 4) K_ATP channels closed 5) Less K+ leaves cells 6) Cell depolarizes 7) Ca++ channels open 8) Ca++ entry triggers exocytosis and insulin is secreted |
|
|
What does the hormone Gastric inhibitory peptide (GIP) do? |
Increase insulin Decreases gastric emptying/acid |
|
|
What does the hormone Glucagon-like peptide-1 (GLP-1) do? |
Increases insulin Decreases glucagon (effects depend on high glucose) Increase beta-cell growth Decreases gastric acid emptying, feeling of satiety |
|
|
What stimulates insulin secretion? |
Increased plasma glucose Gastrointestinal hormones like GLP-1 and GIP, both released in response to nutrient ingestion (feed forward regulation) Increase plasma amino acids Parasympathetic nervous system |
|
|
What inhibits insulin secretion |
Sympathetic nervous system |
|
|
Jennifer was recently diagnosed with type 1 diabetes. One morning she injects herself with somewhat more insulin than is needed for the amount of food that she consumed, but less than a fatal dose. What changes would you expect to observe after the injection? B) Hyperglycemia C) Fewer glucose transporters on cell membranes D) Release of glucagon |
D) |
|
|
What is glucagon secreted by and what is its target? |
Secreted by pancreatic alpha-cells Target is liver |
|
|
What are the effects of glucagon when there is more of it than insulin? |
Increased glycogenolysis Increased gluconeogenesis Increase ketogenesis |
|
|
What can glucagon prevent? |
Hypoglycemia In response to fasting, glucagon triggers the activation of a cascade of signalling molecules inside the hepatocytes, each transmitting and amplifying the fasting signal |
|
|
What stimulates glucagon secretion? |
Decreased plasma glucose Increased plasma amino acids Sympathetic nervous system |
|
|
What inhibits glucagon secretion? |
GLP-1 |
|
|
What are the three active hormones does proglucagon produce and where is proglucagon expressed? |
Glucagon, GLP-1 and GLP-2 Expressed in alpha cells, L cells of intestine and brain |
|
|
What is the main product of proglucagon in alpha cells? |
Main product is glucagon |
|
|
What is the main produce of proglucagon in L cells of intestine and brain? |
Main products are GLP-1 and GLP-2 |
|
|
A 38 year old women with extreme thirst and frequent urination (symptoms started 3 months ago) Drink 10-15 large glasses of water and several cans of soda over 2-3 hours. She urinates at least 4-5 times per hour When conducting a physical exam, she appears normal, 5ft tall, 128lbs, blood pressure 102/68, pulse 72. What disorder should be ruled out immediately? |
Diabetes type 2 |
|
|
What is the adrenal medulla and what does it secret? |
It is a modified sympathetic ganglia which contains sympathetic nervous tissue for hormone response to flight or flight system Secretes catecholamines (epinephrine) that are of three categories: 1) Sex steroids (testosterone 2) Mineralcorticoids (aldosterone) 3) Glucocorticoids (cortisol) |
|
|
What regulates catecholamine release from the adrenal medulla? |

In the spinal cord, innervated by the preganglionic sympathetic neuron would, causing release of ACh in adrenal medulla causing the chromaffin cell (a modified postganglionic sympathetic neuron in the adrenal medulla) to release catecholamines (like epinephrine) into the blood and to target tissues Main hormone is epinephrine because it is secreted in sufficient quantity to exert effects Stimulus for release would be activation of sympathetic nervous system |
|
|
What is the role of epinephrine? |
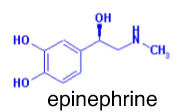
Mediate rapid stress response |
|
|
What is the role of epinephrine in liver? |
Glucose release via enhanced glycogenolysis |
|
|
What is the role of epinephrine in fat? |
Fatty acid release Used as energy substrate |
|
|
What is the role of epinephrine in the heart? |
Increase force of contraction by inotropy (increasing force) or chronotropy (increase heart rate) causing more blood output to tissue |
|
|
What is the role of epinephrine in intestine? |
Muscle relaxation |
|
|
What is the role of epinephrine of intestine, skin and kidneys? |
Arteriole/afferent constriction Things like digestion and making urine is inhibited |
|
|
What is the role of epinephrine in muscles? |
Arteriole constriction (alpha receptors) or arteriole relaxation (beta-2 receptors) |
|
|
What is the role of epinephrine in the brain? |
Increase alertness |
|
|
What is the role of epinephrine in respiration? |
Bronchodilator Increases the airway to get more air into the lungs |
|
|
How does epinephrine trigger vasoconstriction? |
By an alpha-receptor response |
|
|
How does epinephrine trigger vasodilation? |
By an beta-2-receptor response |
|
|
What is the location, GPCR and basic pathway of an alpha-1-adrenoceptors? |
Smooth muscle Gq Increases PLC, IPS and intracellular Ca++ (causing muscle contraction) |
|
|
What is the location, GPCR and basic pathway of a alpha-2-adrenoceptor? |
Presynaptic nerves Gi Decreases activation of adenylate cyclase and cAMP |
|
|
What is the GPCR and basic pathways of beta adrenoceptors? |
Gs Increases activation of adenylate cyclase, cAMP, and intracellular signaling pathways |
|
|
Where can beta-1 adrenoceptors be found? |
Heart |
|
|
Where can beta-2 adrenoceptors be found? |
Smooth muscles |
|
|
Where can beta-3 adrenoceptors be found? |
Fat tissue |
|
|
What adrenoceptors can be found on smooth muscle? |
Alpha-1 and beta-2 |
|
|
What kind of adrenoceptors can be found in the intestinal blood vessels? |
Alpha-receptors |
|
|
How does the effect of epinephrine change depending on its concentrations? |
At low concentration, has more pronounced beta receptor effects At high concentrations, more pronounced alpha-1 receptor effects |
|
|
What adrenoceptor does phenylephrine work on exclusively? |
Alpha 1 |
|
|
George is eating at his new favourite thai restaurant, Pai. He forgets he's allergic to peanuts and goes into anaphylaxis. This includes having a low blood pressure, tightening of his airways and a diffuse urticarial rash. What would help George right at this moment |
Catecholamines (phenylephrine or epinephrine to increase bronchioles) Steroids can but it won't help him immediately and in the moment |
|
|
What is anaphylaxis? |
Systemic immune reaction to an allergen that the body has been previously exposed to. Patients develop the following symptoms (only need a rash and one other): 1) Rash - urticaria 2) Cardiovascular system - hypotension (low blood pressure) secondary to systemic vasodilation (artery dilation) 3) Respiratory - Tightening of the upper airways (life threatening) 4) Gastrointestinal - nausea/vomiting/diarrhea |
|
|
Why is anaphylaxis life threatening? |
Because it causes tightening of the upper airways |
|
|
What happens when you have too much or too little ACTH in the adrenal cortex? |
Too much: gets bigger in size Too little: Atrophy |
|
|
What are the three main regions of the adrenal cortex |

Zona reticularis Zona fasiculata Zona glomerulosa |
|
|
What does the zona reticularis of the adrenal cortex produce? |
Sex hormones |
|
|
What does the zona fasciculata of the adrenal cortex produce? |
Glucocorticoids |
|
|
What does the zona glomerulosa of the adrenal cortex produce? |
Aldosterone |
|
|
What would happen with an increase in ACTH production from the anterior pituitary? |
Increase of production of all hormones coming from the adrenal cortex |
|
|
What is the hormone DHEA? |
Dehydroepiandrosterone
|
|
|
What are the physiological roles of DHEA and androstenedione? |
Men: no outstanding physiological role Women: maintain pubic hair and axillary hair (secondary sex characteristics), source of estrogen after menopause Children: contribute to andrenarche - public hair, body odor, skin oiliness and acne at onset of puberty |
|
|
How is the synthesis of DHEA and androstenedione regulated? |
Stimulated by adrenocorticotrophic hormone (ACTH) which activates an enzyme at an early step in steroidogenesis But intrinsic changes in enzyme activity occur during life span |
|
|
What happens when aldosterone acts on the kidney? |
Increases transportation in both apical and basal sides Prevents degradation of apical Na+ channels Increases expression of Na+ and K+ channels and Na+/K+ ATPase Reabsorption of Na+ and secretion of K+, water can follow Na+ which increases plasma Na+ and blood volume |
|
|
What prevents cortisol from activating receptors in principal cells? |
Principal cells express 11beta-hydroxysteroid dehydrogenase (only expressed in cells that have aldosterone receptors) which converts cortisol to cortisone (which no longer has the same affinity for the aldosterone receptor) |
|
|
What does 11beta-hydroxysteroid dehydrogenase do? |
Converts cortisol to cortisone |
|
|
What stimulates aldosterone synthesis? |
Adrenocorticotropic hormone (ACTH) High concentration of potassium in the plasma (can cause potassium excretion which keeps sodium, this can be lethal) Angiotensin 2 |
|
|
What inhibits aldosterone synthesis? |
High osmolarity of extracellular fluid Main osmosis in blood is sodium (and chloride but not as much) Done by peeing out sodium and returning osmolality to where it's supposed to be |
|
|
What would be an effect of removing the aldosterone from an individual? A) Increase in plasma K+ concentration B) Increase in blood pressure C) Increase in plasma Na+ concentration D) Increase in blood volume |
A) Increase in plasma K+ concentration |
|
|
Kramer has an elevated aldosterone concentration noted in his blood stream. What would happen to his ACTH? |
Normal ACTH |
|
|
What are the functions of cortisol? |
Protects against hypoglcemia (catabolic) by: - liver gluconeogenesis (increase blood concentration of glucose) - skeletal muscle protein breakdown - fat lipolysis - required for full activity of glucagon and epinephrine Reduces concentration of Ca++ in the body - decreases intestinal absorption, increases renal excretion and stimulates bone resoprtion Suppresses the immune system |
|
|
Why are analogs of cortisol used as drugs to suppress the immune system? |
Inhibit inflammatory response Suppresses pituitary hormones including ACTH |
|
|
What is the hormone CRH and where is it secreted from and what does it stimulate? |
Corticotropin releasing hormone Secreted from the hypothalamus Stimualtes the anterior pituitary which produces ACTH |
|
|
Where is cortisol secreted from and what does it stimulate/inhibit? |
Secreted from adrenal gland Stimulates/target cells of liver, fat, muscle, bone and lymphocytes to increase concentration of blood glucose, decrease body's calcium concentration and decrease immune system Inhibits hypothalamus and anterior pituitary hormone release |
|
|
Elaine has chronic arthritis that require high does steroid treatment for several months. She is now better and would like to come off her steroids. What would you do to reduce the chance of becoming steroid deficient? A) It's too late, she has to stay on steroids for life B) Stop them abruptly and see what happens C) Give catecholamines as needed D) Taper (lower) the steroid dose |
D)
|
|
|
What is Cushing's syndrome? |
An adrenal hormone disorder It is cortisol excess Can cause tumors Treatment is cortisol therapy Symptoms are hyperglycemia, muscle protein breakdown, lipolysis but build up of fat on trunk and fat, increased appetite, mood elevation followed by depression, difficulty when learning and memory |
|
|
What is a treatment for Cushing's syndrome? |
Cortisol therapy |
|
|
What are the symptoms of Cushing's syndrome? |
Hyperglycemia Muscle protein breakdown Lipolysis but build up of fat on trunk and face Increased appetite Mood elevation followed by depression Difficulty with learning and memory |
|
|
What is Conn's syndrome? |
Aldosterone excess Can cause tumors Symptoms are K+ depletion, Na+ retention, weakness, hypertension (high blood pressure), polyuria, and tetany |
|
|
What are the symptoms of Conn's syndrome? |
K+ depletion Na+ retention Weakness Hypertension Polyuria Tetany |
|
|
What is Addison's disease? |
Hyposecretion of all adrenal steroid hormones Caused by autoimmune destruction of adrenal cortex Symptoms are loss of weight, fatigue, hypotension, fasting causing fatal hypoglycemia and stressed caused collapse, water retention, danger of water intoxication, diffuse tanning of skin, spotty pigmentation |
|
|
What are the symptoms of Addison's disease? |
Loss of weight Fatigue Hypotension Fasting causing fatal hypoglycemia and stressed caused collapse Water retention and danger of water intoxication Diffuse tanning of skin Spotty pigmentation |
|
|
How does Addison's disease cause tanning of the skin? |
Because no cortisol but rather a lot of ACTH which comes from POMC which can produce alpha-MSH which activate melanocytes which cause skin pigmentation |
|
|
An individual has Cushing's syndrome caused by a tumour of the anterior pituitary. What would you observe in comparison to normal? A) CRH and ACTH low and cortisol high B) CRH, ACTH and cortisol low C) CRH low and ACTH and cortisol high D) CRH, ACTH and cortisol high |
C) |
|
|
How do bones form and grow? |
2 steps bone growth: 1) Chondrocytes form a model of bone 2) Esteoblasts differentiate to start ossification |
|
|
What is the long part of the bone called? |
Diaphysis |
|
|
When does bone growth cease? |
When the epiphyseal plates fuse If you fracture your epiphyseal plate, you disrupt the tissue and structure, causing deformed joints (and possible preventing further growth) |
|
|
What is growth dependent on? |
Diet and genetics Hormone and growth factors such as: - Growth hormone and insulin-like growth factor 1 - Thyroid hormones - Insulin - Sex steroids - Cortisol |
|
|
What does estrogen do to chondrocytes?
|
Can cause them to die |
|
|
What do growth hormones (GH) do? |
Stimulate bone growth GH directly and indirectly, via IGF-1, stimulate bond remodeling |
|
|
What do osteoclast do? |
Reabsorbs bone Increases recruitment and matrix resorption |
|
|
What do osteoblasts do? |
Increase recruitment, proliferation and matrix |
|
|
What closes the epiphyseal plate to stop growth? |
Raising estrogen levels results in the closure of epiphyseal growth plate in both males and females |
|
|
What is somatotropin? |
Synthesized in the anterior pituitary Single-chain polypeptide Species-specific Receptor signals through kinase pathways Plasma GH binding protein Acts directly and by stimulating IGF-1 release |
|
|
What are the metabolic effects of somatotropin? |
Anabolic for protein Catabolic for fat and carbohydrates, increasing glucose in blood to allow growth to happen |
|
|
What are portal vessels in the anterior pituitary? |
Carry the trophic hormones directly to the anterior pituitary |
|
|
What stimulates the release of GH and what does GH stimulate the release of? |
Stimulated from GHRH released from the hypothalamus which goes to the anterior pituitary gland to secrete GH GH goes to the liver and simulate the release of IGF-1 |
|
|
You suspect that Jerry has GH excess but you are not 100%. The wait time for an MRI is 6 months and you want to see if he has elevated GH. What could you do? |
Glucose suppression test This is negative feedback which can inhibit GH levels. If not suppressed, there is some sort of problem with GH |
|
|
What is normal levels of GH |
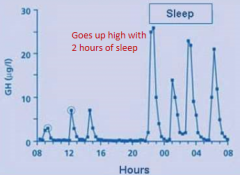
It will go up after 2 hours of sleep |
|
|
What would you expect to observe in a person who has developed a tumour of the anterior pituitary that arose in cells that secrete growth hormone? |
Insulin-like growth factor levels would be higher than normal |
|
|
What hormone does C cells secret? |
Secrets calcitonin which tones down calcium |
|
|
What are two important thyroid hormones? |
Triiodothyronine (T3)
- Made up of 2 tyrosine and 3 iodine -This is 5x more biologically active than T4 Thyroxine (T4) -Made up of 2 tyrosine and 4 iodine |
|
|
How are T3 and T4 synthesized? |

1) Follicular cell synthesizes enzymes and thyroglobulin for colloid 2) A Na+/I- symporter brings I- into the cell. Pendrin transporter moves I- into colloid 3) Enzyme add iodine to tyrosine to make T3 and T4 4) Thyroblogulin is taken back into the cell in vesicles 5) Intracellular enzymes separate T3 and T4 from protein 6) Free T3 and T4 enter circulation |
|
|
What is the MIT in T3/T4 synthesis? |
Monoiodotyrosine Just an iodine and a tyrosine |
|
|
What is DIT in T3/T4 synthesis? |
Diiodotyrosine A iodine and a monoiodotyrosine |
|
|
Put the following steps in the synthesis of thyroid hormones in correct order: 1) T3 and T4 cleaved from thyroglobin 2) Phagosome fuses with lysosome 3) Tyrosine residues on thyroglobulin iodinated 4) T3 and T4 diffuse into blood stream 5) Coupling of MIT and DIt |
3, 5, 2, 1, 4 |
|
|
What does TRH (hormone) stand for? |
Thyrotropoin releasing hormone |
|
|
What does TSH (hormone) stand for? |
Thyroid stimulating hormone |
|
|
What does TSH stimulate and activate? |
TSH activates the G-protein coupled adenylyl cyclase-cAMP-protein kinase A system in thyroid follicular cells It stimulates: 1) Activities of enzymes involved in T3 and T4 synthesis 2) Activity of specific transcription factors that turn on genes involved in T3 and T4 synthesis and thyroid growth |
|
|
What is the mechanism of action of thyroid hormones? |
T3 and T4 (both steroids) circulate in the blood bound to plasma proteins T3 more 3-5x more potent than T4 T4 converted to T3 in target tissues Both bind to nuclear thyroid receptors (form homodimers or heterodimers with retinoic acid receptor) Alter gene transcription |
|
|
What is the function of thyroid hormones in metabolics? |
Increase metabolic rate Increase oxygen consumption Increase heat production Increase protein degradation Increase lipolysis Using more energy and producing more heat, if you have excessivethyroid function you lose weight and are very hot |
|
|
What is the function of thyroid hormones in the nervous system? |
Speaks more quickly and have more energy to do things Sleep more Thinking Reflexes |
|
|
What are the function of thyroid hormones in growth and development? |
Essential in children Works with CH |
|
|
What are the functions of thyroid hormones in cardiovascular? |
Enhances heart rate and contractility Peripheral blood flow Works in part by increasing number of beta adrenergic receptors and other proteins |
|
|
What are the functions of thyroid hormones in muscular? |
Too much cause muscle weakness |
|
|
What is hyperthyroidism? |
Thyroid hormone disorder of thyroid hormone excess Caused by tumours of thyroid gland and thyroid-stimulating immunoglobulins (Graves' disease) Symptoms are nervousness, insomnia, high heart rate, eye diseases such as exopthalamus (can see white around iris), weight loss and anxiety |
|
|
What is Graves disease? |
Thyroid-stimulating immunoglobulins Autoimmune disease where body produces abnormal antibodies against the TSH receptors that are produced Most common cause of general thyroid enlargement in developed counties |
|
|
What are the symptoms of hyperthyroidism? |
Nervousness Insomnia High heart rate Exopthalamus Weight loss Anxiety |
|
|
What does the thioamides do? |
Inhibits production of T3 and T4
|
|
|
What is hypothyroidism? |
Thyroid hormone deficiency Caused by lack of iodine in diet and under active thyroid (T3 and T4 will be low) Symptoms is lethargy, fatigue, cold-intolerance, weakness, hair loss and weight gain |
|
|
What are the symptoms of hypothyroidism? |
Lethargy Fatigue Cold-intolerance Weakness Hair loss Weight gain |
|
|
What are the causes of hypothyroidism? |
Lack of iodine in diet Under active thyroid |
|
|
A man is iodine deficient, predict his levels of TRH, TSH and T3 and T4 secretion in comparson to normal: |
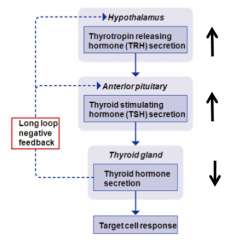
|
|
|
A man has a tumour of anterior pituitary that secrets excessive TSH. What would his levels of TRH, T3 and T4 secretion be in comparison to normal? |
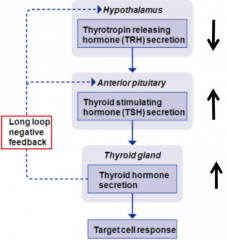
|
|
|
A woman has Graves disease, what would her levels of TRH, TSH and T3 and T4 secretion be in comparison to normal? |
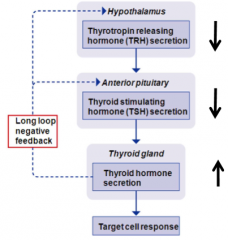
|
|
|
How often do female's gametes go through positive feedback? |
Once a month |
|
|
What is gametogenesis? |
Gametes with 34 chromosomes are produced from cells in gonads with 46 chromosomes Process involves Meiosis: 1) DNA replicated once 2) Cells undergo division twice In contrast: Mitosis = normal cell division: 1) DNA replicated once 2) Cells undergo division once |
|
|
What happens to a person's sperm count and menstruation when they are stressed? |
Lower sperm count and stop menstruating |
|
|
How are GnRH secreted from the hypothalamus? |
GnRH is secreted in pulses from the neuroendocrine cells in the hypothalamus Low pulse frequency stimulates FSH High pulse frequency stimulates LH GnRH is released in pulses (to allow normal release of LH where highdosage of GnRH will cause everything to stop and shut everything down) Pulsatility critical for reproductive function Regulated by hormonal feedback and higher brain centers Pulse frequency/amplitude changes during devleopment |
|
|
Why is GnRH secreted in pulses? |
To allow normal release of LH where high dosage of GnRH will cause everything to stop and shut everything down |
|
|
Which of the following concerning the regulation of reproductive hormone secretion is correct? A) GnRH acts directly on the gonad to stimulate peptide hormone release B) LH and FSH are released from posterior pituitary C) LH stimulates the release of steroid hormones from the gonads D) GnRH is released continually from cells in the pituitary |
C)
|
|
|
Where do sperm sit in the male reproductive system? |
Epididymis |
|
|
Why does the scrotum sit outside the body? |
Outside because spermatogenesis likes to be just below bodytemperature |
|
|
Where are sperm produced? |
Produced in testis Optimal at 2-3C lower than body temperature Takes ~64 days 200 million per day Further mature in epididymis |
|
|
What are sertoli cells? |
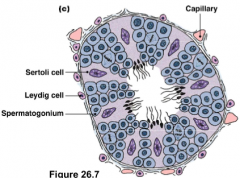
AKA sustentacular cells Support sperm development Providing the right environment for sperm production |
|
|
What are Leydig cells? |
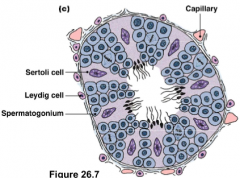
AKA interstital cells Secrete testosterone NOTE: No testosterone receptors on sperm cells |
|
|
Explain spermatogenesis/spermiogenesis? |
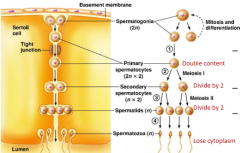
Formed during fetal development Following mitosis, one spermatogonium stays to produce more The other cells begin to undergo meiosis forming spermatocytes Four spermatids produced from one starting cell Spermatids mature into spermatozoa Lose cytoplasm and gain a tail |
|
|
What is the acrosome of the spermatozoa? |
Derived from the Golgi Contains hyaluronidase and acrosin which breakdown the zona pellucida, a glycoprotein coat that overs the oocyte |
|
|
What is in semen? |
1% of it is spermatozoa Rest are secretions of accessory glands: -Water -Lubricant such as mucous - Buffers to neutralize the slightly acidic vaginal vault - Nutrients such as fructose, citric acid, vitamin C and carnitine - Enzymes - Zing - Prostaglandins for smooth muscle contraction (vaginal wall contractility which allow sperm to move to right location) |
|
|
What is the purpose of the corpora cavernosa in the penis? |
It has space for blood to fill which is important for maintaining erections |
|
|
What regulates transfer of semen to female? |
The nervous system Sympathetic is to point (erection), parasympathetic is to shoot (ejaculation) With artillery (high pressure systems) dilation, you increase theamount into the penis (and blood leaves through veins which are lower pressuresystems) which compresses the veins which means you cannot have blood leave theerection |
|
|
What is the name of the cells that nurture the developing spermatozoa? |
Sertoli cells |
|
|
What is the protein ABP? |
Androgen-binding protein Any testosterone produced by leydig cells can bind to this protein so it concentrates testosterone to it when the testosterone enters the testes |
|
|
What happens when FSH stimulates Stertoli cells? |
Support sperm development
Secret inhibin (a hormone that inhibits FSH release)
Secrete androgen-binding protein (helps to concentrate androgen in testis) |
|
|
What happens when LH stimulates Leydig cells? |
Secrete testosterone in response to LH |
|
|
What does neonatal mean? |
Soon after birth |
|
|
What is the hormone DHT? |
Dihydro-testosterone More potent and stable than testosterone and expressed at tissue sites of interest |
|
|
What does 5(alpha)-reducatase do? |
Turns testosterone into dihydro-testosterone (DHT) |
|
|
What does testosterone and related steroids do in sex-specific tissue of adult males? |
Promote spermatogenesis Maintains and stimulates secretion from prostate (primary DHT stimulates prostate which means here there is a lot of 5(alpha)-reductase) and seminal vesicles Maintains reproductive tract |
|
|
What does testosterone and related steroids have on reproductive effects in adult males?
|
Increases sex drive (even for females) Negative feedback effects on GnRH, LH and FSH secretion |
|
|
What does testosterone and related steroids have on secondary sex characteristics in adult males? |
Male pattern of hair growth, including baldness Promotes muscle growth (anabolic) Increases sebaceous gland secretion (can cause achene during puberty) |
|
|
What does testosterone and related steroids do for nonreproductive effects in adult males? |
Promote protein synthesis Increase aggression Stimulates erythropoiesis (production of red blood cells) |
|
|
How can you treat benign prostate enlargement and male pattern baldness? |
With unwanted side effects (such as production of breast tissue in men), you can use 5(alpha)-reducatase |
|
|
A 28 year old weight lifter, who for the past 6 years has been competing at the national level. Has has been taking high levels of androgenic (i.e. anabolic) steroids for several years. Predict his blood levels of LH, FSH and endogenous testosterone in comparison to normal? |
All will be low |
|
|
A 28 year old weight lifter, who for the past 6 years has been competing at the national level. Has has been taking high levels of androgenic (i.e. anabolic) steroids for several years. What changes to the reproductive system would you expect to observe? |
Less sperm development, no FSH (but still have testosterone development) |
|
|
How are oocytes produces? |
By oogenesis During fetal life, oogonia (diploid) develop, which enter (not complete, stops at prophase 1) meiosis 1 Born with ~1-2 million primary oocytes. At puberty about 300,000 remain After puberty, one primary ooctye completes meiosis 1 and enters meiosis 2 to become a secondary oocyte The secondary oocyte released at ovulation Secondary oocyte completes meiosis 2 only if it is fertilized |
|
|
What are three differences between oogenesis and spermatogenesis? |
In oogenesis: 1) Assymmetric cell division (only one secondary oocyte product from each oogonium, while spermatogenesis is 4 from 1) 2) Limited duration (no oocyte production after menopause, average age 51) 3) Limited number of primary oocytes |
|
|
When does fecundity begin to decrease? |
At the age of 30 |
|
|
What can FSH simulate in females? |
Stimulate follicle to grow, producing estrogen thus positive feedback on follicle to continue growing As blood estrogen increases, FSH inhibited |
|
|
Where is progesterone produced? |
Corpus luteum |
|
|
Why does menses happen? |
Progesterone withdrawal
|
|
|
How frequent does the endometrium fall off? |
Happens approximately every 28 days Sensitive to estrogen |
|
|
In the ovarian cycle, what happens at the end of the follicular phase and beginning of luteal hase? |
An oocyte (egg with DNA) is released |
|
|
What is the Theca? |
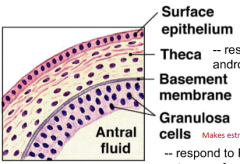
A cell of the amture follicle Respond to LH and make androgens esp and androstendione |
|
|
What are genuolsa cells? |
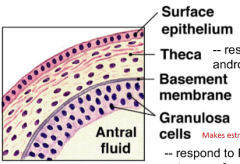
Make estrogen, stimulated by FSH Respond to FSH and make estrogens from androstendione released from theca |
|
|
What are the steps in the ovarian cycle? |
1) Small number of priomordial follicles develop 2) Become a primary follicle with thecal and granulosa cells. Theca cells synthesize androgens which are converted to estrogens in granulosa cells 3) An antrum (fluid filled cavity forms). Fluid contains hormones and enzymes. Structure now called secondary follicle 4) A dominant follicle develops called the Graafian (tertiary) follicle 5) Graafian follicle ruptures and ovulation occurs 6) Follicular cells left behind in ovary become corpus luteum. Corpus luteum releases progesterone and estrogen 7) If fertilization does NOT occur, corpus luteum degenerates. The scar tissue remaining is called corpus albicans. If fertilization occurs, corpus luteum continues to make progesteron and estrogen until the end of the first trimester |
|
|
What hormones does the corpus luteum secret and what happens to the corpus luteum when there is no fertilization? |
Secrets progesterone and estrogen
Degenerates if not fertilized and the scar tissue becomes the corpus albicans |
|
|
What is the menses? |
Blood vessels supplying the endometrium undergo constriction causes shedding of the endometrial lining because of declining levels of progesterone and estrogen |
|
|
What is the proliferative phase of the uterine cycle? |
Endometrium develops in response to estrogen. Endomatrial lining thickens as the blood supply to the tissue is re-established and cells proliferate |
|
|
What is the secretory phase of the uterine cycle? |
Glands in endometrium secrete more viscous fluid
Endometrial cells deposit lipid and glycogen in cytoplasm under the influence of progesterone and estrogen |
|
|
Which of the following concerning the luteal phase of the ovarian cycle is correct? B) It starts after ovulation of the secondary oocyte C) It occurs during the proliferative phase of the uterine cycle D) It is named for the yellow colour of the secondary oocyte |
B) |
|
|
What is the early to mid-follicular phase? |

Day 0 = start os menses Just before day 0, GnRH pulses (one every 1.5 hr), causing LH and FSH release LH stimulates the release of androgens from theca cells, which are converted to estrogens by ganulosa cells under influence of FSH Ganulosa cells also secrete AMH (anti-Mullerian hormone) prevents recruitment of additional follicles Estrogens exert positive feedback on granulosa cells by increasing number of estrogen receptors and increasing proliferation, which leads to more estrogen release Estrogen exerts negative feedback at pituitary and hypothalamus |
|
|
What is late follicular phase and ovulation? |

Tertiary follicle present (large follicle that produces anti-molarity hormone not allowingother follicles to ovulate) Follicular cells begin to secrete inhibin and progesterone along with estrogen High estrogens increase frequency of GnRH pulse to 1/65 min (positive feedback) causing a surge of estrogen Progesterone also increases pituitary sensitiveity to GnRH Causes LH surge, which triggers completion of meiosis I and ovulation High estrogen output does not directly work in GnRH but ratherneurons afferent to it |
|
|
What is early to mid-luteal phase? |

Corpus luteum under influence of LH and FSH releases progesterone, inhibin and estrogen These hormones exert negative feedback at hypothalamus and pituitary Progesterone inhibits GnRH pulses (1 every 3-4 hours) Doesn't have a follicle to do the inhibition but now rather the hormones |
|
|
What is the late luteal phase? |

The intrinsic life-span of the corpus luteum is 12 days If fertilization does not take place, corpus luteum undergoes apoptosis Progesterone and estrogen levels fall Reduced negative feedback at hypothalamus and pituitary returns GnRH pulses to one ever 1.5 hours |
|
|
What are the secondary sex characteristics of the estrogen in females? |
Development and maintenance of breast development as well as fat distribution on hips and upper thighs |
|
|
What are the secondary sex characteristics of androgens from the adrenal cortex in females? |
Public and axillary hair and sex drive |
|
|
Birth control pills are often contain a combination of estrogens and progesterone that are taken continuously for 3 weeks/cycle. What effect do you think this has on plasma FSH and LH levels for these 3 weeks? |
Both remain low |
|
|
When does the oocyte under go its Meiosis 2? |
After fertlization from a sperm |
|
|
Which hormone is not produced by the corpus luteum? A) Estrogen B) Progesterone C) Inhibin D) AMH - anti-mullerian hormone |
D) Produced by the ganulosa cells of the follicle, not corpus luteum |
|
|
How does estrogen create a positive feedback on LH levels? A) Estrogen works through neurons upstream of GnRH to stimulate GnRH at high concentrations B) Estrogen works through neurons upstream of GnRH at low concentrations to stimulate high concentrations C) Progesteron acts directly at the GnRH neuron to stimulate GnRH D) Estrogen at high concentrations directly stimulates LH |
A) |
|
|
What causes menopause and what is it? |
Menopause is the cessation of the reproductive cycle Ovaries lose their ability to response to FSH and LH (follicles just stop responding) Estradiol and progesterone levels fall Lack of negative feedback causes FSH and LH to rise |
|
|
When you want to get pregnant, when would be the most optimal time to have sex? |
Between 4 days before ovulation and 1 day after |
|
|
How long is an oocyte viable for? |
24 hours |
|
|
What happens when a sperm undergoes capcitation? |
It becomes hyperactive Albumin, enzymes and lipoproteins bind to the sperm Glycoprotein coat removed, intracellular changes and develop strong whip-like motion |
|
|
What aid the transport of sperm in the vagina? |
Uterine and oviduct contractions |
|
|
What is the corona radiata of the egg? |
Loosly connected granulosa cells |
|
|
What is the zona pellucida of the egg? |
Glycoprotein layer Fusion of sperm and egg causes a cortical reaction which prevent polyspermy |
|
|
What does the glycoprotein layer of the egg have receptors for? |
The sperm which allow the sperm to sit down on the ovum and desposits its nucleus into the ovum |
|
|
What is the acrosomal reaction? |
Enzymes allowing to break through the corona radiata Sperm then bind to sperm binding protein and allow nucleus to enter the egg Sperm docks with sperm-binding protein on oocyte membrane, triggering depolarization of oocyte (a fast polysperm block) Fusion of cortical granules (vesciles) with membrane is a slow polysperm block. Contents coat oocyte and prevent pentration of other sperm |
|
|
What happens after fertlization? |
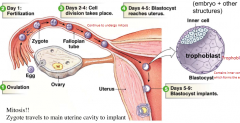
Day 1: Fertlization Day 2-4: Cell diversion takes place Day 4-5: Blastocyst reaches uterus Day 5-9: Blastocyst implants |
|
|
What is a trophoblast? |
Outerlayer of the blastocyst |
|
|
What is the decidua? |

Comes from mom (maternal) Very vascular to provide nutrients for potentially developed embyro To increase surface area, it spreads itself from developing fetus Produced from endomatrial cells, secrete several hormones and growth factors which form the maternal placenta |
|
|
What do the syncitiotrophoblast/cytoblast cells do? |
Help with invasion of endometrium and form the placenta AND secrete hormones (HCG, Estrogen, progesteron and human placental lactogen) |
|
|
What does the hormone Human Placental Lactogen do? |
AKA Human chorionic somatomammotropin Decreases insulin sensitivity in mom If this is not kept in check, this can cause diabetes in mom called gestational diabetes which can cause an increased likely of developing diabetes in the future as well Cure for this is either mom get more insulin or to deliver the baby |
|
|
What is Preeclampsia? |
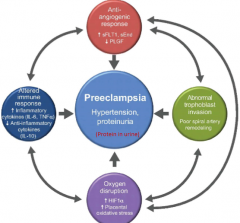
Hypertension and proteinuria (protein in urine) It is potentially fatal in mother Can be caused by: - Abnormal trophoblast invasion - Oxygen disruption - Altered immune response - Anti-angiogenic response |
|
|
Which hormone does the trophoblast not secrete? A) Estrogen B) Human placental lactogen C) Progesterone D) Luteinizing hormone E) Human chorionic hormone? |
D) |
|
|
What can prevent menses? |
Human chorionic ganadotropin (hCG) secreted from the trophoblast/placenta Similar in structure to LH |
|
|
What does the hCG do in relation to pregnancy? |
Maintains the corpus luteum which allows you to maintain the endometrium for pregnancy |
|
|
What does the hormone inhibin do? |
Inhibits FSH |
|
|
Of week two of embryonic/placental development (FYI), what is the amnion? |
Eventually form the sac like structure that surrounds embryo |
|
|
Of week two of embryonic/placental development (FYI), what is the yolk sac? |
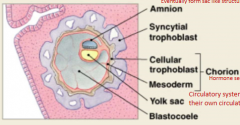
Circulatory system until the fetus gets their own circulatory system (the heart) |
|
|
What role does the placenta have? |
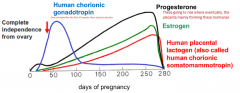
It is a temporary endocrine organ Performs role of digestive, respiratory and renal system for the fetus For the first 10 weeks, Human chorionic gonadotropin will be elevated then start to decrease For progesterone, estrogen and human placental lactogen, they will begin off low and eventually rise |
|
|
What is critical at the beginning of pregnancy to maintain the endometrial lining? A) Follicle cells B) Corpus luteum C) Yolk sac D) Amniotic fluid |
C) |
|
|
In the placental circulation, is oxygenated or deoxygenated blood coming from the veins from mom? |
Oxygenated |
|
|
In the placental circulation, is oxygenated or deoxygenated blood coming from the arteries from mom? |
Deoxygenated |
|
|
What is the function of human chorionic gonadotropin as a placental hormone? |
Maintains corpus luteum Stimulates fetal testis (teste growth in males) |
|
|
What is the function of progesterone as a placental hormone? |
Suppresses uterine contractions, cervical plug and mammary gladn development |
|
|
What is the function of estrogen as a placental hormone? |
Uterine development (growth, blood supply, oxytocin receptors), breast duct development |
|
|
What is the function of human placental lactogen as a placental hormone? |
Structurally related to growth hormone and prolactin High in mother/low in fetus Decreases maternal cellular uptake of glucose, enhances maternal lipolysis |
|
|
How is labour triggerd? |
Before parturition, relaxin released from ovary and placenta loosens the ligaments in the pelvic bone and causes the cervix to stretch Specific/exact triggers/initiation is not well known at the moment (date of writing this answer: June 21, 2015) |
|
|
What is the hormone relaxin? |
Relaxin is a hormone coming from placenta will relax some ligamentsof the pelvis which can allow the baby to move downwards and cause cervicalstretch |
|
|
Elaine is 41 weeks pregnant (over normal gastation) and wants to deliver her baby. What can you do to help with this process? |
Soften the cervix
By doing this, you can allow the baby to move down to create stretch which can create a natural process to happen |
|
|
What hormones are necessary for breast milk BEFORE parturition? |
Estrogens and progesterone needed for the development of mammary glands but inhibit milk production |
|
|
What hormones are necessary for breast milk AFTER parturition? |
Prolactin for epithelial milk producing cells Oxytocin for myoepithelial cells for squeezing milk out Both released form the pituitary gland |
|
|
Why should a mother breastfeed? |
Reduced infections (passing of immunity) Perfect balance of nutrition Skin to skin contact promotes bonding Decreased incidence of sids Reduced obseity Protection against chronic diseases Its FREE!!!!!! Consumes about 500 kcal per day for mom |
|
|
Match the correct hromone and response: A) Estrogen - milk secretion B) Progesteron - milk secretion C) Prolactin - milk production D) Oxytocin - milk production |
C) |
|
|
What chromosome pair gives a female offspring? |
XX |
|
|
What chromosome pair gives a male offspring? |
XY |
|
|
What is the Mullerian duct? |
Forms all internal female organs Fallopian tube uterus upper vagina |
|
|
What is the Wolffian duct? |
Forms all the male internal organs Epididymis vas deferens seminal vesicles |
|
|
What is so special about the Y chromosome? |
Has SRY gene that promotes tastes development If you are XY with non-functioning SRY gene, you will become a female SRY codes for transcription factor called SOX9 |
|
|
What is the SRY gene? |
It codes for the transcription factor SOX9
|
|
|
What is SOX9? |
Coded by the gene SRY It is a transcription factor Involved in development of Sertoli cells and testes as well as expression of Anti-Mullerian Hormone It can initiate Sertoli cell differentiation |
|
|
How does SOX9 cause regression of Mullerian duct? |
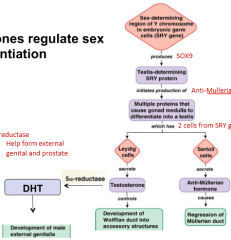
1) Sex-determining region of Y chromosome in embryonic germ cells (SRY gene) produces SOX9
2) Testis-determining SRY protein initiates production of Anti-Mullerian
3) Multiple proteins that cause gonad medulla to differentiate into testis
4) Sertoli will then secrete anti-Mullerian hormone which cause regression of Mullerian duct |
|
|
How does SOX9 cause development of Wollfrian duct into accessory structures? |
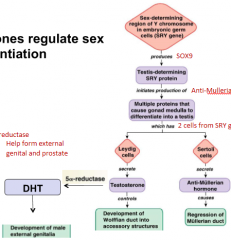
1) Sex-determining region of Y chromosome in embryonic germ cells (SRY gene) produces SOX9 2) Testis-determining SRY protein initiates production of Anti-Mullerian 3) Multiple proteins that cause gonad medulla to differentiate into testis 4) Leydig cells will secrete testosterone which controls development of Wolffian duct into accessory structures |
|
|
How does SOX9 cause the development of male external genitalia? |
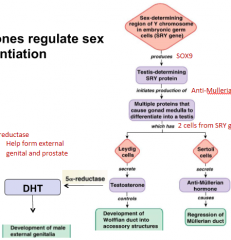
1) Sex-determining region of Y chromosome in embryonic germ cells (SRY gene) produces SOX9 2) Testis-determining SRY protein initiates production of Anti-Mullerian 3) Multiple proteins that cause gonad medulla to differentiate into testis 4) Leydig cells will secrete testosterone which will be converted into DHT by 5alpha-reductase 5) This will cause development of male external genitalia |
|
|
Explain the development of internal male organs: |
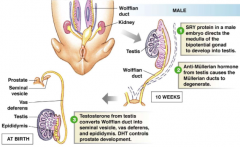
1) SRY protein in a male embryo directs the medulla of the bipotential gonad to develop into testis 2) Anti-Mullerian hormone from testis cause the Mullerian duct to degernate 3) Testosterone from testis converts Wolffian duct into seminal vesicle, vas deferens and epididymis. DHT controls prostate development |
|
|
Explain the development of external male genetalia: |
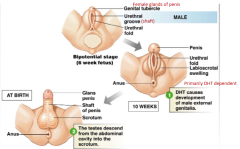
1) DHT causes development of male external genitalia (primarily DHT dependent) 2) The testes descend from the abdominal cavity into the scrotum |
|
|
What is the genital tubercle? |
Female gland of the penis |
|
|
What is beta-catenin? |
A gene regulatory protein that suppresses SOX9 expression |
|
|
Explain the development of female internal organs |
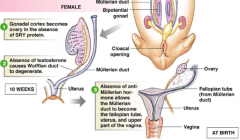
1) Gonadal cortex becomes ovary in the absence of SRY protein 2) Absence of testosterone causes Wolffian duct to degenerate 3) Absence of anti-Mullerian hormone allows the Mullerian duct to become the fallopian tube, uterus and upper part of the vagina |
|
|
Explain the development of female external genitalia |
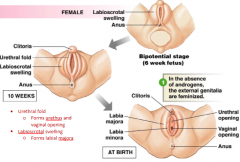
In the absence of androgens, the external genitalia are feminized
|
|
|
What are urethral folds? |
Forms urethus and vaginal opening |
|
|
What is the labioscrotal swelling? |
Forms labial majora |
|
|
Predict development in XY individual with complete androgen insensitivity (androgen receptors not function. Will there be internal male organs? Will there be external male genitalia? What will be the phenotype? |
No No Female not fertile |
|
|
Predict development in XY individual with t-alpha reductase defficiency Will there be internal male organs? Will there be external male genitalia? What will be the phenotype? |
Yes Variable because you can still have testosterone Variable |
|
|
Predict development in XX individual exposed to high levels of androgens during fetal development
Will there be internal male organs?
Will there be external male genitalia?
What will be the phenotype? |

No
Variable
Variable |
|
|
What is puberty? |
Activation of HPG axis resulting in gonad maturation Rapid growth and development with earlier, more obvious signs in girls At the onset of puberty, the GnRH system is activated which as well as pulse frequency increases during puberty With no leptin receptors, there will be no puberty |
|
|
What hormone will Cause the regression of Wolffian ducts? |
AMH |
|
|
What happens to pulse frequency of GnRH when you enter puberty? |
Increased frequency of pulses |
|
|
POMC is an example of what type of hormone? A) Prohormone B) Exocrine hormone C) Amine hormone D) Steroid hormone |
A) |
|
|
Catecholamine hormone typically act at what part of the cell? A) Intracellular B) Cell membrane C) Nuclear D) Both cytosol and cell membrane |
B)
|
|
|
What does estrogen when bound to its receptors act on? A) Other receptors B) Translation directly C) Hormone response elements D) None of the above |
C) |
|
|
Which of the following hormones decreases total calcium levels? A) Vitamin D B) Cortisol C) PTH D) Estrogen |
B) |
|
|
George has PTH secreting tumor. What would you see in his blood work and how could you help him? A) Low calcium - remove parathyroid glands B) High calcium - remove parathyroid glands C) Low calcium - give a thioamide D) High calcium - give a thioamide |
B) |
|
|
Which of the following changes will increase renal filtration of blood? A) Dilation of afferent and efferent arterioles B) Constriction of afferent and efferent arterioles C) Dilation of efferent and constriction of afferent D) Constriction of efferent and dilation of afferent |
D) |
|
|
Diabetes insipidus will produce what type of urine? A) Highly concentrated urine B) Highly diluted urine C) Urine with lots of glucose D) Urine with lots of amino acids |
B) |
|
|
Which of the following hormones does come from the medulla? A) Epinephrine B) Dopamine C) Androgens D) Norepinephrine |
C) |
|
|
George comes into your office with a high blood pressure, low potassium and high sodium levels. What do you think is going on and the possible source of his problem?
A) High aldosterone levels - posterior pituitary tumor
B) High aldosterone levels - tumor of the fasiculata
C) High aldosterone levels - tumor of glomerulosa
D) High aldosterone levels - tumor of medulla |
C) |
|
|
What hormone is responsible for closure of epiphyslea plate? A) Epinephrine B) Dopamine C) Testosterone D) Estrogen |
D) |
|
|
How can both an underactive and overactive thyroid both present a goiter (thyroid hyperplasia large neck mass)? A) Iodine deficiency and a thyroid hormone secreting nodule (that is 1cm in size) B) Iodine surplus and TSH producing tumor C) Iodine deficiency and Graves disease D) Iodine surplus and PTH tumor |
C) |
|
|
What does not inhibit growth hormone release? A) Glucose B) Growth hormone C) Somatostatin D) Cortisol |
D) |
|
|
Abdominal pain, renal stones, confusion/delirium and bone pain is the result of what abnormality? A) Hypocalcaemia B) Hypercalcaemia C) High cortisol levels D) Low cortisol levels |
B) |
|
|
|
|