![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
92 Cards in this Set
- Front
- Back
|
In what position should the knee be place when performing a Valgus stress test for the medial collateral ligament? A-2 |
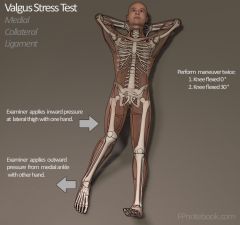
20 to 30° flexion |
|
|
Patient has a transtibial amputation and has recently been fitted with a patellar tendon bearing socket. During initial prosthetic check out, the PT instruct the patient to walk several times in the parallel bars, and then sit down and take off the prosthesis. Upon inspection of the skin the therapist would expect to see no redness in what area? A-4 |
The anterior tibia and tibial crest. There may be redness at the patellar tendon and tibial tuberosity, medial tibial and fibular plateaus, and the medial and lateral ends of the residual limb |
|
|
Patient is experiencing sensory changes secondary to left CVA. I'm testing, the patient is unable to detect pinprick or temperature in the right hand, leading to disuse and increased safety risk. These changes are best documented as "patient is experiencing:" A – 7 |
Analgesia: the absence of sensibility to pain. NOT anesthesia which is loss of sensation, usually by damage to the nerve receptor; NOT allodynia is pain resulting from a stimulus which would not normally for the pain; NOT abarognosis is the inability to appreciate the weight of objects held in the hand
|
|
|
During a cervical spine examination, the PT observes restricted left rotation of the C7 – T1 spinal level. After stabilizing the thoracic spine, the therapist hand placement for mobilization to improve left rotation should be at the: A – 10 |
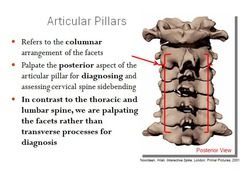
Posterior right C7 articular pillar |
|
|
The patient is able to walk independently with an assistive device in the hall outside the PT gym. When asked to walk across the hospital lobby in through the revolving door, the patient slows down considerably and stops E folding door, unable to proceed the therapist determines: A-15 |
Open skills and externally paced skills are impaired while closed skills are intact |
|
|
A patient with metabolic syndrome is participating in a circuit training program involving both aerobics and strengthening training. The therapist noticed that the patient is sweating and having difficulty concentrating on activity and coordinating movements. When asked if there's a problem, the patient is confused and has difficulty speaking. The therapist should: A-18 |
The patient down and administer fruit juice immediately NOT discontinue the exercise and rest the patient or discontinue the exercise and refer the patient back to the physician |
|
|
During examination of the patient who complains of back pain, the PT notes pain with end range AROM to left hip flexion, abduction, and external rotation. The origin of the pain is most likely the: A-19 |
Capsule of the hip joint NOT sacroiliac joint, sartorius muscle, or left kidney |
|
|
During which phases of the gait cycle with a physical therapist expect to observe an everted posture of the calcaneus? A-20 |

Initial contact (heel strike) through loading response (foot flat) NOT from mid stance through heel off (toe off) |
|
|
A factory worker injured the right arm in a factory press with damage to the owner nerve at the elbow. A diagnostic EMG was performed three weeks after the injury, with evidence of spontaneous fibrillation potential's. In this case, the PT recognizes that: A-22 |
Denervation has occurred NOT reinnervation is complete NOT neurapraxia has occurred NOT reinnervation is in process |
|
|
14-year-old boy with advanced Duchenne's muscular dystrophy is administered a pulmonary function test. The value that is unlikely to show any deviation from normal is: A-24 |
Functional residual capacity he NOT vital capacity NOT forced expiratory volume in one second NOT total lung capacity |
|
|
Therapist performs the slump test on a patient with a diagnosis of lumbar disc herniation's complaint is pain in the posterior thigh. Which of the following findings would indicate a positive test result? A-26 |
Pain in the posterior thigh that is relieved with cervical extension NOT pain in the lumbar spine region that is increased cervical flexion NOT pain in the butt ox it is unchanged head or ankle movement NOT pain in the posterior knee and calf that is relieved with ankle plantar flexion |
|
|
PT progresses through an examination, is becoming evident that a current patient is anterior cruciate ligament deficient in the right knee. Which of the following tests will be unnecessary for determining whether the ACL was ruptured? A-27 |
Anterior drawer test (not sure why this is right) NOT Lachman's test NOT Slocum's test NOT lateral pivot shift test |
|
|
Should has class III heart disease and is continually in and out of congestive heart failure. Digitalis did jocks and has been prescribed to improve heart function. The patient will demonstrate understanding of the adverse side effects of this medication by recognizing the importance of contacting the primary physician with the appearance of which of the following symptoms? A-37 A-37
|
Weakness and palpitations NOT confusion and memory loss NOT tachycardia NOT involuntary movements and shaking |
|
|
A 10-year-old presents with pain 4\10 and limited knee range of motion 5 to 95° following surgical repair of the medial collateral ligament and ACL. In this case the modality that can be used with precaution is: A-46 |
Ultrasound NOT high rate transcutaneous electrical stimulation Not continuous shortwave diathermy NOT premodulated interferential current |
|
|
A newborn with whole arm paralysis is referred to physical therapy. Initially, the plan of care should include: A-56 |
Partial immobilization of the limb across the abdomen, followed by gentle range of motion after immobilization NOT passive mobilization of the shoulder in the overhead motions NOT age-appropriate tasks training of the extremity NOT spending the shoulder and abduction and internal rotation |
|
|
A six month old child was referred to PT for right torticollis. The most effective method to stretch the muscle is by positioning the head and neck into: A-57 |
Extension, left side bending and right rotation * remember that right torticollis means the right SCM is tight |
|
|
It is most important for the PT to educate the client who recently had a radical lymph node dissection secondary to prostate cancer to: A-58 |
Closely monitor any changes in the fitting of their socks or shoes NOT routinely perform circumferential measurements of both lower extremities NOT to use a home compression pump with pressure greater than 80 mmHg NOT use alkaline soaps and cleansers on the skin |
|
|
A PT is performing clinical research in which a specific myofascial technique applied to a patient with chronic back pain. She using a single case experimental design with an ABAB format research hypothesis states the pain rating scores will decrease with the treatment intervention acceptance of this hypothesis would be if: A-59 |
B is less than a NOT B is equal to a NOT B is greater than A at the 1.0 level NOT B is greater than A at the .05 level |
|
|
The patient is recovering from a stroke and demonstrates good recovery in the lower extremity (out of synergy movement control). Timing deficits are apparent during walking. Isokinetic training can be used to improve: A-60 |
Rate control and varying movement speed NOT rate control at slow movement speeds NOT reaction time NOT initiation of movement |
|
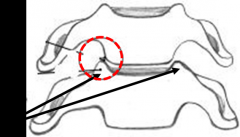
The radiographic view shown in the diagram that demonstrates the observed spinal defect is: A-63 |
Oblique |
|
|
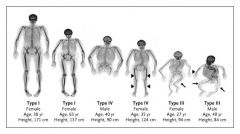
Patient presents with pronounced muscle weakness and wasting in the lower extremities, hypertension and moon shaped face with truncal obesity. The therapist recognizes the symptoms as characteristics of: A-64 |
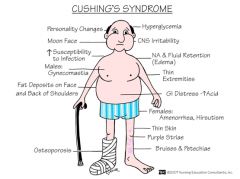
Cushing's Syndrome NOT type two diabetes NOT Addison's disease NOT hypoparathyroidism |
|
|
When conducting the anterior drawer stress test at the ankle one week following acute inversion injury, the physical therapist was attempting to test mechanical stability provided primarily by the: A-66 |
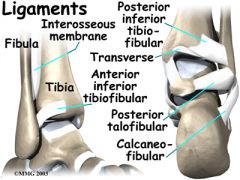
(I guessed, but got this right) Anterior talofibular ligament |
|
|
Search your reviewed current literature related to moderate exercise for maintaining independent without accelerating disease progression and persons with any of the roses. The search yielded nine studies: two clinical case reports, to cohort studies, three single randomized controlled trial's, and two multicentered RCTs. What is the levels of evidence, which studies provide the best evidence for support of exercise in persons with ALS? A-68 |

Multi center RCTs NOT cohort/comparison studies |
|
|
A patient diagnosed with lumbar spinal root impingement due to narrowing of the intravertebral foramen has been referred to physical therapy for mechanical traction. What is the lowest percentage of body weight that should be considered for the initial traction force when using a split table? A-70 |
25% NOT to 15% |
|
|
The physical therapist is reviewing the medical history of a new patient being seen for balance deficits and general deconditioning. Prior to admission, the chief finding by the physician, three days ago, was a positive fecal blood test. Which laboratory value would confirm the patient is safe for balance retraining activities? A-71 |
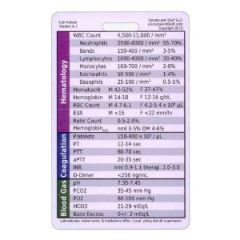
Hematocritic 42% NOT leukocyte count 7000 NOT ESR 7mm/1 h.
|
|
|
While reviewing a patient imaging films, the most appropriate imaging view to identify abnormal anatomy of the pars interarticularis in the lumbar region is: A – 72 |
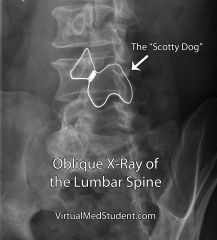
Oblique view NOT anteroposterior view NOT lateral view NOT lumbar sacral |
|
|
Patient with breast cancer had a surgical removal of the mass, followed by 12 weeks of chemotherapy (6 treatments) and eight weeks of radiation (daily). She's referred to physical therapy for mobilization of her upper extremity. The therapist recognizes that providing post radiation therapy, it is important to: A – 73 |
Observe skincare precautions NOT avoid stretching exercises that pole on the radiated site NOT observe infection control procedures NOT avoid all of the exercise for at least two months |
|
|
Patient with brittle (uncontrolled) diabetes mellitus is being seen in physical therapy for a prosthetic check out. The patient begins to experience lethargy, vomiting, and abdominal pain. The therapist notes weakness with some confusion, and suspects: A – 76 |

(Got this one right but was not sure) Ketoacidosis |
|
|
A 62-year-old patient has chronic obstructive pulmonary disease. Which of these pulmonary test results will not be increased when compared with those of a 62-year-old healthy individual? A – 77 |
FEV1/FVC (forced vital capacity) ratio NOT functional residual capacity NOT TLC NOT residual volume |
|
|
Five days after an aortic valve replacement, patient is diagnosed with a DVT. The patient was immediately started on anticoagulant and the therapist is preparing for treatment. The best treatment program should include: A-79 |
Intermittent pneumatic compression stockings NOT treatment being deferred as exercise is contra indicated at this time NOT supine exercises as the patient should be kept on bed rest NOT walking program at a vigorous intensity level |
|
|
An elderly patient has been confined to bed for two months, and now demonstrates limited range of motion in both lower extremities. Range of hip flexion is 5 to 15° and knee flexion is 10 to 120°. The most beneficial intervention to improve flexibility and ready this patient for standing is: A-80 |
Mechanical stretching using traction and 5 pound weight, two hours, two times per day NOT hold relax techniques followed by passive range of motion, 10 repetitions, two times per day NOT manual passive stretching, 10 repetitions each joint, two times per day NOT tilt-table standing, 20 minutes, daily
|
|
|
Patient who is three months post CVA is being treated and PT for it he's of capsulitis of the right shoulder. Today, the patient complains of new symptoms, including constant burning pain in the right upper extremity he is increased by dependent position and touch. The right hand is mildly swollen and stiff. In this case, the intervention that is contraindicated is: A-84 |
Passive manipulation and range of motion of the shoulder NOT stressed loading using active compression during upper extremity weight-bearing activity NOT positional elevation, compression and gentle massage to reduce edema NOT active range of motion exercises of the limb within a pain-free range to regain motion |
|
|
To prepare a patient with an incomplete T12 paraplegia (Asia A) for ambulation with crutches, the upper quadrant muscles that would be most important to strengthen include the: A-85 |
Lower trapezius, latissimus dorsi, and triceps NOT middle trapezius, latissimus dorsi, and triceps NOT deltoid, triceps and respect yours NOT upper traps, rhomboids and levator scapula |
|
|
A patient was referred to PT complaining of loss of cervical AROM. X-rays showed degenerative joint disease at the uncinate process in the cervical spine. The motion that would be most restricted would be: A-88 |
Side bending NOT rotation NOT flexion NOT extension |
|
|
A child with full thickness burns to both arms is developing hypertrophic scar. The best initial intervention to manage these scars is: A-93 |

(Got this one right, but guessed) Application of custom-made pressure garments NOT application of compression wraps NOT application of occlusive dressing NOT primary excision followed by autografts |
|
|
Patient with COPD has developed respiratory acidosis. The PT instructs the PT student participating in the care to monitor the patient closely for: A-94 |
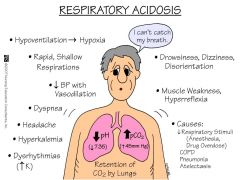
(Got this one right, but guess) Disorientation NOT tingling or numbness of the extremities NOT dizziness or lightheadedness NOT hyperreflexia |
|
|
A computer programmer in her second trimester of pregnancy was referred to physical therapy with complaints of tingling and the loss of strength in both her hands. Her symptoms are exacerbated if she is required to use her keyboard work for longer than 20 minutes. The most beneficial physical therapy intervention is: A – 95 |
Placing the wrists in resting splints NOT ice packs to the carpal tunnel NOT dexamethasone phonophoresis to the carpal tunnel NOT hydrocortisone iontophoresis to the volar surface of both wrists |
|
|
There is strong evidence linking certain drugs to increased fall risk in older adults. Patients should be cautioned about fall risks when taking: A – 96 |

Elavil NOT raloxifene NOT baclofen NOT levodopa |
|
|
Patient with complete C6 tetraplegia (Asia A) to be instructed to initially transfer with a sliding board using: A – 97 |
Shoulder extensors, external rotators and anterior deltoid to position and lock the elbow NOT shoulder depressor's and triceps, keeping the hand flexed to protect tenodesis grasp NOT pectoral muscles to stabilize the elbows and extension and scapular depressors to lift the trunk NOT serratus anterior to elevate the trunk with elbow extensors stabilizing |
|
|
Patient demonstrates weakness when rotating the head to one side as well as weakness flexing the head laterally and forward to the same side. The therapist recognize these are symptoms of a lesion of the: A – 98 |
Spinal nerve root of the accessory nerve on the contralateral side NOT spinal nerve roots of the accessory nerve on the same side |
|
|
A patient with active tuberculosis is referred to physical therapy. The patient has been hospitalized in on appropriate antituberculin drugs for three weeks. During treatment, what precautions should therapist observe? A-99
|
The patient can be treated in the PT gym, without precautions NOT the patient must be treated in a private, negative pressure room NOT the therapist must wear personal protective equipment at all times |
|
|
With PD demonstrates a highly stereotypical gait pattern characterized by impoverished movement and a festinating gait. The intervention it would be most beneficial to use it this patient is: A – 74 |
locomotor training using a motorized treadmill and bodyweight support harness NOT locomotor training using a rolling walker |
|
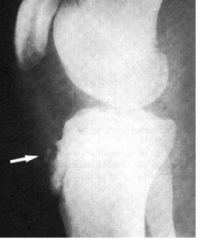
World has been referred to PT clinic for treatment of patellar tendinitis. The exam reveals that the patient is unable to hop on the affected LE because of pain. The PT decides refer the patient back to the pediatrician for an x-ray of the knee. The patient returns for therapy with the x-ray shown in the figure. The therapist initial intervention should focus on: A-100 |
Iontophoresis using dexamethasone and patient education regarding avoidance of squatting and jumping activities NOT fitting the patient with crutches for non-weight-bearing ambulation and initiation of hydrocortisone phonophoresis NOT aggressive plyometric exercises with the boots on and durance training NOT patient education regarding avoiding falls onto the affected me, and open chain me, extension exercises to improve quadriceps strength |
|
|
What common compensatory postures what a PT expect for a patient diagnosed with fixed severe forefoot varus A – 102 |
Subtalar pronation and medial meditation of the tibia NOT excessive midtarsal supination and lateral rotation of the tibia NOT telling in and lateral rotation of the femur NOT excessive ankle dorsiflexion and medial rotation of the femur ??? I still do not understand this??? |
|
|
Middle aged patient is recovering from surgical repair of an inguinal hernia and is experiencing persistent discomfort in the groin area. Patient education should focus on: A – 104 |
Proper lifting techniques and precautions against heavy lifting NOT avoiding straining or turning in bed NOT close mouth breathing during any lifting NOT sitting too long in any one position |
|
|
Posture of the forefoot that is inverted relative to the rearfoot while and subtalar neutral, would be described as: A – 105 |
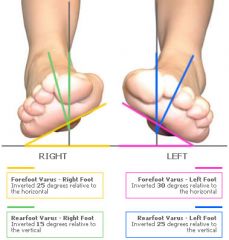
forefoot varus NOT forefoot valgus |
|
|
Patient has lumbar spinal stenosis encroaching on the spinal cord. The PT should educate the patient to avoid: A – 106 |
Swimming using the cross train NOT using a rowing machine NOT tai chi activities NOT bicycling using a recumbent cycle ergometer |
|
|
Examines the benefits of strength training and functional performance and older adults. The data analysis involves a meta-analysis. This refers to: A – 107 |
Pulling up data of RCTs to yield a larger sample NOT pulling of data of all available studies to yield a larger sample NOT a mechanism to critically evaluate studies NOT data analysis performed by the Cochrane collaboration |
|
|
During the initial exam a client with an ulcer superior to the medial malleolus, the PT notes hemosiderosis and liposclerosis. There are no signs of infection, there's minimal drainage, granulation is present in the wound is clean except for a small amount of yellow fibrin deposits. The next action the therapist should take is: A-109 |
Perform ABI NOT apply an Unna boot NOT to debride the wound with whirlpool irrigation NOT apply 4 layer bandaging system |
|
|
An 11 year old was referred to physical therapy with complaints of vague pain at the right hip and thigh that radiated to the knee. Active range of motion is restricted in abduction, flexion and internal over Tatian. A gluteus medius gait was observed ambulation for 100 feet. Best choice for PT intervention is: A – 110 |
Close chain partial weight-bearing lower extremity exercises for slipped capital femoral epiphysis NOT orthosis to control lower extremity position as a result of femoral anteversion NOT hip joint mobilization to improve the restriction motion as result of Legg-Calve'-Perthes disease * does not make sense, as the treatment is to surgically stabilize the bone with screws and pins!* |
|
|
A patient is referred to physical therapist the diagnosis of bells palsy. Which cluster of examination findings below with the therapist expect to find? A-111 |
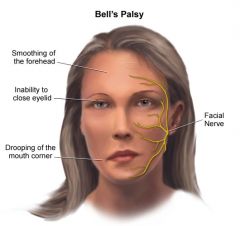
Decreased closure of one eye, drooping of the mouth and inability to raise the eyebrow NOT ptosis, weakening in the temporal and massetter muscles and deviation of the tongue to one side NOT decreased sensation to the forehead, cheek and jaw; absence of a gag reflex; deviation of the tongue to one side NOT ptosis, decreased abduction of the eye and excessive tearing |
|
|
Physical therapist in a PT student at a pediatric clinic are reviewing precautions and contraindications regarding various pediatric pathologies. The precaution with the most credibility that merits discussion is: A– 113 |
Do not do PROM with children with osteogenesis imperfecta NOT do not use active exercise with children with muscular dystrophy NOT do not use PROM with children with arthrogryposis multiplex congenita NOT limit sensory input with children with autism |
|
|
Patient presents with a large plantar ulcer that will be debrided. The foot is cold, pale, and edematous. The patient complains of dull aching, especially when the leg is in the dependent position. The condition that would most likely result in this critical presentation is: A – 115 |
Venus insufficiency NOT chronic arterial insufficiency NOT acute arterial insufficiency NOT DVT |
|
|
A patient with stasis dermatitis secondary to Venus insufficiency is being examined by the PT. Visual inspection of the skin can be expected to reveal: A – 117 |
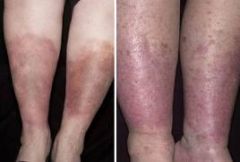
Hemosiderin Staining NOT plaques with scales NOT extensive erosions with serous exudate NOT pruritus, erythema and edema |
|
|
A PT receives a referral for a patient with neurapraxia involving the owner nerve secondary to an elbow fracture. Based on knowledge of this condition therapist expects that: A – 119 |
(I got this one right, but guessed) Nerve dysfunction will be rapidly reversed, generally in 2-3weeks |
|
|
A home health PT is treating elderly patient. On this day, the patient is confused, shortness of breath and generalized weakness. Given a history of hypertension and hyperlipidemia, the therapist suspects the patient: A – 121 |
May be presenting with early signs of myocardial infarction NOT forgot to take prescribed hypertension medication NOT maybe experiencing unstable angina NOT is exhibiting mental changes indicative of early Alzheimer's disease |
|
|
Patients hospitalized in intensive care unit following a dramatic SCI resulting in C3 tetraplegia (ASIA A). The patient is receiving endotracheal suctioning, following development of significant pulmonary congestion. The recommended time duration for endotracheal suctioning is: A– 123 |
10 to 15 seconds NOT 1 to 5 seconds NOT 5 to 10 seconds NOT 15 to 20 seconds |
|
|
A frail older adult is confined to bed in a nursing facility and has developed a small superficial wound over the sacral area because only small amounts of necrotic tissue are present, the physician has decided to use autolytic wound debridement. This is best achieved with: A – 124 |
Transparent film dressing NOT sharp debridement NOT wet to dry gauze dressing with antimicrobial appointment NOT wound irrigation using a syringe |
|
|
Patient was instructed to apply conventional (high rate) transcutaneous electrical nerve stimulation to the low back to modulate of chronic pain condition. The patient now states that the TENS unit is no longer effective in reducing the pain in spite of increasing the intensity to maximum. The PT should now advise the patient to: A – 125 |
Switch to modulation mood TENS NOT switch to low rate TENS NOT increase the treatment frequency NOT decrease the pulse duration |
|
|
PT has decided to refer a two-year-old child to a neurologist after the initial evaluation. Therapist has concluded that the child may be autistic. The most part in fact her to include in the referral is that the child is: A – 128 |
Defensive when touched NOT responsive to most but not all command NOT delayed and gross motor skills NOT quiet and did not want to separate from his mother |
|
|
During a physical therapy session, and elderly woman with LBP tells the PT that she has had urinary incontinence for the last year. This is particularly problematic when she's had a cold and cough a lot. She's not hold her physician about this problem because she is too embarrassed. The therapist best course of action is to: A – 131 |
Examine the patient, document impairments and discuss findings with the physician NOT refer the patient back to her position NOT examine the patient, document impairments and then refer her back to her physician NOT examine the patient and proceed with treatment for low back pain |
|
|
During a sensory examination, a pt complains f a dull, aching pain and is not able to discriminate a stimulus ass sharp or dull. 2-pt discrimination is absent, Based in these findings. the pathway that is intact is the : A-132 |
Anterior spinothalamic tract |
|
|
A pt is 5 days post myocardial infarction and is referred for inpatient cardiac rehabilitation. Appropriate criteria for determining the initial intensity of exercise include: A-133 |
HR <120 bpm and RPE <13 NOT HR resting plus 30 bpm and RPE<14 |
|
|
A-135 |
rhythm on a 12-lead ECG NOT exertional level on the Borg scale |
|
|
A pt w/ spastic hemiplegia is referred to PT for ambulation training. The pt is having difficulty in rising to a standing position due to cocontraction of the hamstrings and quadriceps. The PT elects to use biofeedback as an adjunct to help break up this pattern. For knee extension, the biofeedback protocol should consist of: A-139 |
Low detection sensitivity w/ electrodes close together NOT high detection sensitivity w/ electrodes far apart |
|
|
An adolescent female is referred to PT with a diagnosis of anterior knee pain. Positive findings include pez planus, lateral tibial torsion and genu valgum. The position of the femur will be in is excessive: A – 141
|
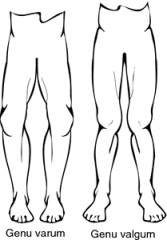
Medial rotation |
|
|
Patient is referred to PT for the Stabile her rehab. Patient presents with spontaneous nystagmus that can be suppressed with visual fixation, oscillopsia, and loss of gaze stabilization. Additional findings include intense disequilibrium, and and ataxic wide-based gate with constant veering to the left. Based on these findings, the PT determines that the patient is most likely exhibiting signs and symptoms: A – 142 |
Meniere's disease NOT acute unilateral vestibular dysfunction NOT acoustic Naroma NOT BPPV |
|
|
Optimal position for ventilation of the patient with a C5 SCI (ASIA A) is: A – 147 |
Supine, head of bed flat NOT semi-fowler's NOT sidling, HOB flat NOT sidling, HOB elevated 45 deg |
|
|
The patient has extensive full-thickness burns to the dorsum, of the right hand and forearm, and is being fitted with a resting splint to support the wrists and hands in functional position. The splint should positioned the wrist and hand in: A – 150 |
Slight wrist extension, with fingers supported and thumb in partial opposition and abduction NOT neutral wrist position, with slight finger flexion and thumb flexion |
|
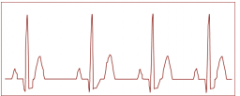
Patient is on the cardiac unit following admission for CHF and history of an MI. The patient is currently compensated by pharmacological management and is comfortable, alert and oriented at rest with normal HR and BP. The telemetric ECG to depicts the rhythm shown in figure. PT's appropriate interpretation and action is: A-151 |
ST SEGMENT depression; check medical record for baseline ECG NOT normal sinus rhythm; continue to monitor during activity progression |
|
|
An 18-month-old child with down syndrome and developmental delay is being treated and early intervention program. They are training activities that should be considered include: A – 153 |
Holding and weight shifting in sitting and standing using tactile and verbal cue NOT stimulation to postural extensors and sitting using rhythmic stabilization |
|
|
With MS demonstrates strong bilateral lower extremity extensor spasticity in the typical distribution of antigravity muscles. This patient would be expected to demonstrate: A – 155 |
(I got this one right, but guessed) Sacral sitting with increased extension and adduction of lower extremities |
|
|
Upon examining a patient with vague hip pain that radiates to the lateral knee, the PT find the negative FABER test, negative grind test and a positive Noble's compression test. The dysfunction is most likely due to: A – 159 |
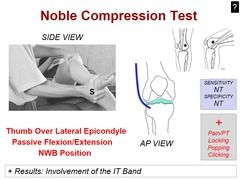
And iliotibial band friction disorder NOT SI joint disfunction |
|
|
A patient with COPD is sitting a bedside chair. The apices of the lungs in this position compared with other areas of the lungs in this position would demonstrate: A – 162 |
Increased volume of air at REEP NOT highs changes in ventilation during the respiratory cycle |
|
|
A therapist is examining a child with a history of primary lymphedema of the right lower extremity that was diagnosed at birth. Thickening of skin folds of the toes is evident. The therapist documents these findings as: A – 164 |

(I got this one right, but I guess) A positive Stemmers sign |
|
|
As the result of blunt trauma to the quadriceps femoris muscle, patient experiences loss of knee function. The best choice for early physical therapy intervention is: A – 165 |
Gentle AROM exercises in weight-bearing NOT gentle PROM exercises in non-weightbearing to regain normal knee motion |
|
|
A PT observes menu recurvatum during ambulation in a patient with hemiplegia. The patient has been using a posterior leafspring orthosis since discharge from subacute rehabilitation four weeks ago. The therapist has previously administered the fugal Meyer assessment of physical performance, and determine the lower extremity score to be 22 (of a possible 34), With strong synergies in the lower extremity and no out of synergy movement. The most likely cause of this deviation is: A – 171 |
Spencer spasticity NOT hamstring weakness |
|
|
A client with rheumatoid arthritis presents at a physical therapy clinic with severe whiplash from a motor vehicle accident one week ago. Initial cervical radiographs results revealed osseous structures appear intact. The clients chief complaints of cervical pain and sudden falls with loss of consciousness. Examination reveals a positive Romberg sign and hyperreflexia. The PT's initial action is to: A-173 |
Fit this client with a heart cervical collar and contact the referring physician recommending a computed tomography scan NOT immediately inform the referring physician recommended magnetic resonance imaging scan |
|
|
An elderly patient with DM is recovering from recent surgery to craft a large ulcer of the heel of the left foot. PT is concerned that loss of range of motion of the ankle will limit ambulation and independent status. One afternoon the therapist very busy request of one of the physical therapy aides do the range motion exercises. The aid is new to the department but is willing to take on this Challenge if the therapist demonstrates the exercises. The therapist best course of action is to: A – 175 |
Perform the range of motion exercises without delegating the task NOT take five minutes to instruct the aid in range of motion exercises |
|

A PT is working with a client who fracture of the left fibula three months ago. The client is still having pain with exercise. Based on the recent radiograph pictured and the given information, the prognosis for this client is: A – 176 |
A bone stimulator or surgery will be required NOT non-weight-bearing is indicated for complete healing |
|
|
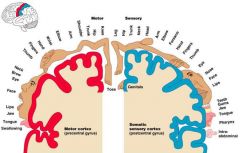
A patient is referred for rehabilitation after a middle cerebral artery stroke. Based on this diagnosis, PT can expect that the patient will present with: A – 178 |

Contralateral hemiparesis and secondary deficits, with the arm more involved than the leg NOT contralateral hemiparesis and sensory deficits, with the leg more involved than the arm |
|
|
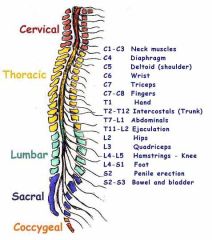
Remember the Homunculus |
|
|
|
To test for maximum passive tibiofemoral internal or external rotation the need to be placed in: A – 180 |
90° of knee flexion NOT 45° of knee flexion |
|
|
PT is performing the maximal cervical quadrant test to the right with a patient with right C5-C6 facet syndrome. Patient would most likely complain of: A – 181 |
Pain in the right cervical region NOT tightness in the right upper trapezius NOT radicular pain into the right upper limb NOT referred pain to the left mid scapular region |
|
|
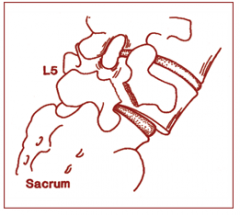
Patient diagnosed with lumbar spondylosis with out disc herniation or bulging has a left L 5 compression. Most likely structure compressing the nerve root is the: A– 183 |
Ligamental flavum NOT anterior longitudinal ligament * remember that the nerve roots come out on the sides where the ligamental flavum is located |
|
|
During an exercise tolerance test, patient demonstrates a poor reaction to increasing exercise intensity. An absolute indication for terminating this test is: A – 184 |
Onset of moderate to severe angina NOT 1.5 mm of downsloping ST segment depression NOT fatigue and shortness of breath NOT supraventricular tachycardia |
|
|
Manual glide of the talus posteriorly with in the ankle joint mortise can be used as a technique to increase: A – 188 |
(got this one right, but not sure why now) Tibiotalar dorsiflexion motion |
|
|
A patient with CHF is on digitalis to improve myocardial contraction. The patient is a new participant in phase 2 outpatient could be cardiac rehabilitation program. PT expects the effects of this medication to include: A – 191 |
Depressed ST SEGMENT on ECG with QT and T-WAVE changes NOT decreased BP
|
|
|
Patient is being treated for secondary lymphedema of the right arm as a result of a radical mastectomy and radiation therapy. The resulting edema (stage one) can best be managing physical therapy by: A – 192 |
Intermittent pneumatic compression, extremity elevation and massage NOT isometric exercises, extremity positioning in elevation and compression bandaging |
|
|
Was referred for PT after a right breast lump ectomy with axillary node dissection. Scapular control is poor extremity flexion or abduction when attempted. Early PT intervention should focus on: A – 192 |
Gravity assisted right upper extremity exercises to promote scapular control following damage the long thoracic nerve NOT strengthening of the right rhomboid to promote normal function of the scapula as a result of damage to the dorsal scapular nerve |
|
|
Patient is referred to PT with complaints of weakness and unsteady gait. The patient had a kidney transplant two years ago. Medications include oral steroids and immunosuppressive agents. Examination reveals decreased proprioception and strength 4/5 both lower extremities. Balance test score was 40/56. The most important action for the PT To take in this case is to: A – 196 |
Refer the patient back to primary care provider NOT instruct in progressive balance exercises NOT instruct in progressive resistance training exercises NOT for me neurologist |
|
|
Complains of difficulty walking. At rest the skin of the lower leg appears discolored. After walking for about two minutes, the patient complains of pain in the leg. A marked pallor is also evident in skin of the lower third of the extremity. The PT suspects: A – 200 |
Vascular claudication NOT neurogenic claudication |