Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
28 Cards in this Set
- Front
- Back
|
Where is the majority of the potassium inside the body?
|
Intracellular space (98%)
|
|
|
What protein has the largest impact on K levels in the body?
|
Na/K ATPase
Regulation of this process is a big dea |
|
|
What is a main function of K as an ion inside the body? What happens if K homeostasis is disrupted?
|
Control of membrane potential in cardiac, neuromuscular cells.
Cardiac arrhythmias |
|
|
What's the normal concentration of K in the ICF? ECF?
|
ICF: 150 mEq/L
ECF: 4.5 mEq/L |
|
|
What changes happen on EKG during hyperkalemia? When in the course the problem do the abnormalities occur?
|
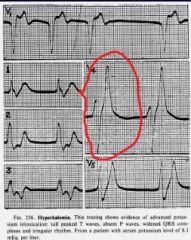
Peaked T waves
You see the changes early on, before you start to have arrhythmias |
|
|
What changes happen on EKG during hypokalemia?
|
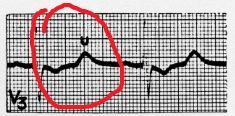
U waves
|
|
|
What are the changes in the EKG that you see during K concentration abnormalities?
|

|
|
|
What are the changes in the EKG that you see during K concentration abnormalities?
|

|
|
|
What is the effect of insulin in membrane channels?
|
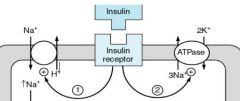
Increase in Na(into)/H(outof) exchange
Increase in Na/K ATPase |
|
|
What defines a metabolic acidosis?
|
pH<7.4
HCO3<24 mEq/L |
|
|
What defines a metabolic alkalosis?
|
pH>7.4
HCO3>24 mEq/L |
|
|
What defines a respiratory acidosis?
|
pH<7.4
PCO2>40 mmHg |
|
|
What defines a respiratory alkalosis?
|
pH>7.4
PCO2<40 mmHg` |
|
|
What is the relationship between intracellular H and K?
|
Reciprocal:
Increased K, less H Increased H, less K |
|
|
Generally, what is the relationship between potassium and acid-base status?
|
Hypokalemia and alkalemia
Hyperkalemia and acidemia |
|
|
What is the activity of beta agonists on channel activity in the kidney?
|
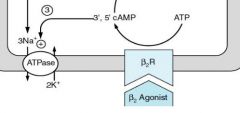
Increase in Na/K exchange
Blocking the beta receptors leads to hyperkalemia...you don't have stimulation of the Na/K exchange |
|
|
What is a nonintuitive stimulus for K insulin release?
|
Increased K intake
|
|
|
What are the main routes of K excretion?
|
Kidney: >85%
GI tract: <15% |
|
|
Where is the main site of control for renal handling of K?
|
The DCT
|
|
|
What are some of the factors that control K homeostasis at the DCT?
|
Aldosterone
Plama K Flow rate pH ADH |
|
|
What are the two main cell types at the collecting duct? What are their functions?
|
Principal cells: Na/K regulation
ICs: Acid-base status |
|
|
What are the effects of aldosterone on the cells?
|
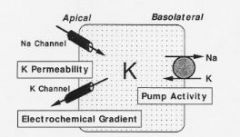
-More channels on the apical membrane
-More Na/K ATPase activity -Changes enzymes of energy activity in cells--> need to be able to make more pumps |
|
|
What is the effect of potassium on aldosterone levels?
|
More potassium, more aldosterone released
Body doesn't want to become hyperkaelemic |
|
|
What is the impact of flow on K excretion?
|
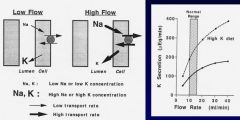
Low flow:
-Na is absorbed well before CD-->not large drive for this guy to go into cells. Not much drive for the Na/K ATPase...not extra K inside the cells-->not abnormally large gradient pushing K out. -naturally high amount of K in lumen High flow: -You've got high Na --> pushes stuff out into the cell-->high Na/K-->lots of K inside cell-->pushing of K out of the glomeruli into urine at high rate -always low concentration in lumen-->more drive of K out |
|
|
Where is the majority of the Mg in the body? Is it readily available?
|
It's in the bone.
It's bound inside the plasma |
|
|
What are the functions of magnesium inside the body?
|
Regulation of membrane excitability via the regulation of postassium, calcium metabolism
|
|
|
Where does handling of Mg take place within the kidney?
|
Distally:
Collecting duct DCT |
|
|
Why should you be concerned with loop diuretics and Mg? Don't loop diuretics work on sodium?
|
Na and Mg resorption distally in the tubule are linked, so things that block Na reabsorption distally also stop Mg reabsorption.
This can cause membrane excitability problems |