Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
275 Cards in this Set
- Front
- Back
|
How many bodies does the sacrum have?
|
Five
|
|
|
How many sets of pelvic (anterior) sacral foramina does the sacrum have?
|
Four
|
|
|
What are the foramen of the sacrum for?
|
Transmission of nerves and blood vessels.
|
|
|
The large masses of bone lateral to the 1st segment of the sacrum are called _______.
|
The alae or wings
|
|
|
The two superior articular processes of the sacrum and the inferior articular process of L5 form the _________.
|
Zygapophyseal joint
|
|
|
________ is the anterior ridge of the 1st sacral segment.
|
Sacral promontory
|
|
|
________ is the continuation of the verebral canal and containts the sacral nerves.
|
Sacral Canal
|
|
|
The _________ is formed by the fused spinous processes of the sacral vertebrae.
|
Median Sacral Crest
|
|
|
The sacrum artivulates with the ilium of the pelvis at the __________.
|
The Auricular surface
|
|
|
What are the small tubercles representing the inferior articular processes projecting inferiorly from each side of the 5th sacral segment?
|
Sacral horns
|
|
|
Each SI joint opens obliquely and posteriorly at what angle?
|
30 degrees
|
|
|
How many segments does the coccyx have?
|
3-5 coccygeal segments
|
|
|
What is the distal portion of the coccyx called?
|
Apex
|
|
|
What is the most proximal portion of the coccyx called?
|
Base
|
|
|
What is the breathing technique for imaging the sacrum and coccyx?
|
Suspend respiration on expiration
|
|
|
What size cassette is used for imaging the sacrum and coccyx?
|
10x12 portrait
|
|
|
What is the CR placement for an AP Axial sacrum?
|
Angle 15 degrees cephalad, midway between the level fo the ASIS and the pubis (approx. 2" distal to the ASIS)
|
|
|
What is the CR placement for an AP Axial coccyx?
|
Angled 10 degrees caudad, 2: superior to the pubis and at MSP
|
|
|
What is the CR placement for the lateral sacrum/coccyx?
|
Perpendicular to IR and 3-4" posterior to the ASIS
|
|
|
What is the CR placement for the lateral coccyx?
|
Perpendicular to IR and 3-4" posterior and 2" distal to the ASIS
|
|
|
What are the holes in the sacrum called?
|
Pelvic (anterior) sacral foramina
|
|
|
What are the gonadal doses for a lateral sacrum/coccyx?
|
Male= 2
Female= 45 |
|
|
Rotation is indicated on a lateral sacrum/coccyx when ________.
|
The greater sciatic notches and femoral heads are not superimposed.
|
|
|
What projection of the lumbar spine best demonstrates intervertebral joints?
|
AP projection
|
|
|
The lateral projection of the lumbar spine best demonstrates what anatomy?
|
Intervertebral joints and intervertebral foramina
|
|
|
The lateral projection of the lumbar spine best demonstrates what pathology?
|
Fractures and Spondylosis
|
|
|
What anatomy is best demonstrated on the 45 degree oblique lumbar spine?
|
Zygapophyseal joints
|
|
|
The superior articular process of one vertebra and the inferior articular process of another vertebra form the _______.
|
Intervertebral foramen
|
|
|
On the LPO position of the lumbar spine, which zygapophyseal joint is demonstrated?
|
Left
|
|
|
On the LAO position of the lumbar spine, which zygapophyseal joint is demonstrated?
|
Right
|
|
|
The soft inner portion of the intervertebral disk is called the _________.
|
Nucleus pulposus
|
|
|
How many vertebra are in the lumbar spine?
|
Five
|
|
|
How many vertebra are in the cervical spine?
|
Seven
|
|
|
The oblique cervical spine best demonstrates the _________.
|
Intervertebral foramina
|
|
|
Cervical vertebra number 1 is also called the __________.
|
Atlas
|
|
|
Cervical vertebra number 2 is also called the __________.
|
Axis
|
|
|
The RAO position for the cervical spine best demonstrates the _________.
|
Downside intervertebral foramina
|
|
|
The LPO position for the cervical spine bet demonstrates the ________.
|
Upside intervertebral foramina.
|
|
|
The gonion (or angle of the mandible) corresponds to which cervical vertebrae?
|
C3
|
|
|
The SID should be 60-72" for anterior/posterior oblique and lateral positions of the C-Spine, true or false.
|
True
|
|
|
The SID should be a minimum of 40" for the AP and open mouth positions of the C-Spine, true/false.
|
True
|
|
|
The lateral cervical spine position best demonstrates the _____________.
|
Zygapophyseal joints
|
|
|
Viewing "O's" on a radiograph of a c-spine means that the patient was in _________ position.
|
Oblique
|
|
|
The AP projection of the thoracic spine best demonstrates the ___________.
|
Intervertebral joints
|
|
|
The lateral projection of the thoracic spine best demonstrates the ___________.
|
Intervertebral disk spaces and intervertebral foramina.
|
|
|
70-75 degree oblique of the thoracic spine best demonstrates ____________.
|
Zygapophyseal joints
|
|
|
The superior articular process of one vertebrae and the inferior articular process of the vertebrae above it form the _________.
|
Zygapophyseal joints
|
|
|
The superior vertebral notch of one vertebrae and the inferior notch of the vertebrae above it form the _________.
|
Intervertebral foramen
|
|
|
The LPO position of the thoracic spine best demonstrates ___________.
|
Right zygapophyseal joints
|
|
|
The RAO position of the thoracic spine best demonstrates _____________.
|
Right zygapophyseal joints
|
|
|
For the oblique thoracic spine position, anterior obliques are recommended because ____________.
|
Less breast dose
|
|
|
The __________ is a small, blunt conical eminence that projects medially and posteriorly from the junction of the neck and shaft of the femur.
|
The greater trochanter
|
|
|
What bony landmark is used for positioning the femoral head and neck?
|
Anterior Superior Iliac Spine
|
|
|
What is the name of the joint found between the superior rami of the pubic bone?
|
Symphysis pubis
|
|
|
Where is the CR placed for a unilateral frog leg?
|
Mid-femoral neck
|
|
|
Where is the CR placed for an AP projection of the pelvis?
|
midway between the ASIS and the symphysis pubis
|
|
|
What is the recommended amount of abduction, of the femurs, for an AP bilateral frog-leg projection?
|
40-45 degrees
|
|
|
How much obliquity of the body should be used for the posterior oblique positions for the SI joints?
|
25-30 degrees
|
|
|
the LPO position for SI joints will demonstrate the right joint, true/false?
|
True
|
|
|
Why must the lower limbs be rotated 15-20 degrees internally for the AP hip position?
|
To place the femoral neck parallel to the IR
|
|
|
The term "pelvic girdle" refrers to the total pelvis including the sacrum and coccyx, true/false?
|
False
|
|
|
Which bones fuse to form the acetabulum?
|
Ischium, pubis, and ilium
|
|
|
What two bony landmarks are palpated using the traditional hip localization method?
|
Symphysis pubis and ASIS
|
|
|
Using the traditional hip localization method, the femoral head can be located _________.
|
1 1/2" below the midpoint of the imaginary line between the two bony landmarks.
|
|
|
True or false. The male pelvis is more heart shaped?
|
True
|
|
|
True or false. The female pelvis is wide and more shallow?
|
True
|
|
|
True or false. The male pelvis has an obtuse angle of the pubic arch.
|
False
|
|
|
True or false. the Female pelvis has a round and large pelvic inlet?
|
True
|
|
|
True or false. The male pelvis has an acute angle of the pubic arch?
|
True
|
|
|
The symphysis pubis is at the level of _____.
|
Base of the coccyx
|
|
|
The ASIS is at the level of _____.
|
S1-S2
|
|
|
The xiphoid tip is at the level of ________.
|
T9-T10
|
|
|
The lower costal margin is at the level of _______.
|
L2-L3
|
|
|
The iliac crest is at the level of ________.
|
L4-L5
|
|
|
The ear of the scottie dog is the __________.
|
Superior articular process
|
|
|
The neck of the scottie dog is the ________.
|
Pars interarticularis
|
|
|
The eye of the scottie dog is the ____________.
|
Pedicle
|
|
|
The nose of the scottie dog is the ___________.
|
Transverse process
|
|
|
The leg of the scottie dog is the ___________.
|
Inferior articular process
|
|
|
The leg of one scottie dog and the ear of another scottie dog make up the ____________.
|
Zygapophyseal joint
|
|
|
The zygapophyseal joints of the L-Spine are classified as _______ joints.
|
Synovial
|
|
|
The zygapophyseal joints of the L-Spine have _______ mobility type.
|
Diarthrodial
|
|
|
The zygapophyseal joints of the L-Spine have what type of movement?
|
Plane (gliding)
|
|
|
The intervertebral joints of the L-Spine are of what classification?
|
Cartilaginous (symphysis)
|
|
|
The intervertebral joints of the L-Spine have what type of mobility?
|
Ampiarthrodial (slightly moveable)
|
|
|
Why is the chin extended on a lateral C-Spine?
|
To prevent superimposition of the mandible over the spine
|
|
|
True or false. An RPO position of the C-Spine requires a 45 degree obliquity of the body with 15-20 degree caudad angle?
|
False. A cephalic angle is used for posterior obliques.
|
|
|
Which part of the intervertebral disk is composed of semigelatinous material?
|
Nucleus Pulposus
|
|
|
Kyphosis is defined as _________.
|
Abnormal thoracic curvature with increased convexity.
|
|
|
Which position best demostrates zygapophyseal joints of the c-spine?
|
Oblique C-spine
|
|
|
If an AP open mouth projection demonstrates the base of the skull and upper incisors are superimposed but they are obscuring the upper portion of the dens, what projection(s) would help demonstrate the dens?
|
The Fuch or Judd method
|
|
|
What breathing technique is used for imaging the C-Spine?
|
Suspend breathing on expiration
|
|
|
What can be done to enhance visibility of the vertebral bodies during a lateral T-Spine?
|
Use a breathing technique to blur the ribs
|
|
|
The bony structures connected directly to the vertebral body are the ______.
|
Pedicles
|
|
|
What angle do the zygapophyseal joints lie at in relation to the midsagittal plance for the thoracic spine?
|
70-75 degrees
|
|
|
Using the anode heel effect which portion of the body would you place at the anode side for a T-Spine?
|
Place the upper side of the T-Spine under the anode.
|
|
|
How much obliquity of the body is required for an LAO projection of the T-Spine (from the plane of the table)?
|
70 degrees
|
|
|
What level is the jugular notch located?
|
T2-T3
|
|
|
At what level is the vertebra prominen?
|
C7
|
|
|
What level is the sternal angle?
|
T4-T5
|
|
|
What level is the mastoid tip located?
|
C1
|
|
|
What level is the thyroid cartilage located?
|
C5
|
|
|
What is the first compensatory curve of the spine?
|
C-Spine
|
|
|
What is the first primary curve of the spine?
|
T-Spine
|
|
|
What is the second compensatory curve?
|
L-Spine
|
|
|
What is the second primary curve?
|
S-Spine
|
|
|
True or false. The anterior oblique t-spine demonstrates the upside zygapophyseal joints?
|
False
|
|
|
How much CR angle is needed for the AP axial C-Spine?
|
15-20 degrees cephalad
|
|
|
Where is the articular pillar located on a cervical vertebra?
|
Between the superior and inferior articular processes.
|
|
|
What is the method name for swimmer's?
|
Twining method
|
|
|
At what angle do the zygapophyseal joints lie in relation to the MSP for the cervical vertebra?
|
90 degrees
|
|
|
What method will project the dens within the shadow of the foramen magnum?
|
Fuch Method
|
|
|
Which thoracic vertebrae possess no facets for costotransverse joints?
|
T11-T12
|
|
|
Why must the lower limb be rotated 15 to 20 degrees internally for AP hip projections?
|
To place the femoral neck parallel to the IR
|
|
|
True or False. The term "pelvic girdle" refers to the total pelvis including the sacrum and coccyx.
|
False
|
|
|
Which bones fuse together to form the acetabulum?
|
Ischium, pubis, and ilium
|
|
|
Which bone of the pelvic girdle forms the anterior inferior aspect?
|
Pubis
|
|
|
The lesser sciatic notch is an aspect of the _________.
|
Ischium
|
|
|
The sacroiliac joints are classified as ____________ joints with _________ mobility.
|
Synovial; amphiarthrodial
|
|
|
The two bony landmarks that are palpated using the traditional hip localization method are what?
|
The ASIS and the symphysis pubis
|
|
|
Using the hip localization method where is the femoral head located?
|
1 1/2" below the midpoint of the imaginary line between the ASIS and the symphysis pubis
|
|
|
Gonadal shielding of the male patient for AP pelvis requires that the shield not extend above the level of the ____________.
|
Inferior margin of the pubis
|
|
|
A common condition of the femur that develops in elderly patients, leading to frequent fractures of the hip is ___________.
|
Osteoporosis
|
|
|
True or false. Gonadal shielding should be used on all patients for AP hip projections?
|
True, if placed correctly
|
|
|
Where is the CR placed for an AP Pelvis
|
Midway between the ASIS and the symphysis pubis
|
|
|
What is the amount of abduction of the femurs recommended for an AP bilateral frog-leg projection?
|
40 - 45 degrees
|
|
|
Which position will demonstrate the superior and posterior rim of the acetabulum?
|
Posterior oblique (Judet Method)
|
|
|
How much obliquity of the body should be used for posterior oblique positions for the SI joints?
|
25-30 degrees
|
|
|
Which position will best demonstrate the right SI joint?
|
LPO
|
|
|
Will the lesser trochanter be visible on an axiolateral (inferosuperior) lateral hip?
|
Yes but only a small part
|
|
|
True or false. The IR must be parallel to the femoral neck for the axiolateral (inferosuperior) projection of the hip.
|
True
|
|
|
What is the proper name for the frog-leg projection?
|
Modified cleaves
|
|
|
What CR angle is required for the AP Axial inlet projection?
|
40 degrees caudad
|
|
|
A radiograph of an AP pelvis reveals the right iliac wing is foreshortened as compared with the left side. What is the error?
|
Left rotation
|
|
|
A radiograph of an AP pelvis reveals that the left obturator foramen is more open or elongated as compared to the right. What is the error?
|
Right rotation
|
|
|
A radiograph of an LPO projection for SI joints reveals that the ilium is superimposed over the involved joint. What is the error?
|
Excessive rotation or obliquity
|
|
|
True or false. If a patient has excessive external rotation of one foot, a fractured hip may be indicated.
|
True
|
|
|
A patient has a possible separation of the symphysis pubis due to trauma. The AP pelvis is inconclusive for determining the extent of the injury. What other projection can be taken?
|
AP axial (Taylor) outlet projection
|
|
|
What modality is most sensitive in diagnosing early signs of metstatic carcinoma of the pelvis?
|
Nuclear Medicine
|
|
|
The most common fracture in geriatric patients because of high incidence of osteoporosis or avascular necrosis is ____________.
|
Proximal hip fracture
|
|
|
Another name for osteoarthritis is _______.
|
Degenerative joint disease
|
|
|
Which ionization chamber(s) should be activated when using AEC for an AP pelvis?
|
Upper right and left chambers
|
|
|
What pathologic indications may result in the early fusion of the SI joints?
|
Ankylosing spondylitis
|
|
|
The lateral aspect of the distal tibia forms a flattened triangular shaped notch. This is called the _______ and is for articulation with the fibula.
|
Fibular notch
|
|
|
The _______ is a rough textured prominence on the mid-anterior surface of the tibia.
|
Tibial tuberosity
|
|
|
The medial malleolus is part of the distal ________.
|
Tibia
|
|
|
The lateral malleolus is part of the distal ____________.
|
Fibula
|
|
|
The adductor tubercle is on the _________ aspect of the ________ condyle.
|
Lateroposterior; medial
|
|
|
When positioning for the AP Medial oblique knee, the entire leg should be rotated ___ degrees.
|
45 degrees internally
|
|
|
What is the correct CR placement for the AP knee?
|
1/2" distal to the apex of the patella
|
|
|
What is the correct CR angulation and placement for a lateral knee?
|
5-7 degrees cephalad to a point 1" distal to the medial epicondyle
|
|
|
When viewing a lateral knee radiograph, you see that the knee is slightly rotated. The adductor tuberlce is seen posterior and in profile, what will correct this error?
|
Rotate the leg more laterally
|
|
|
When viewing a knee radiograph you see that there is a symmetric appearance of the femoral head and tibial condyles and the joint space. The approximate medial half of the fibular head is seen superimposed by the tibia. The intercondylar eminence is seen in the center of the intercondylar fossa. This description describes proper positioning of the ___________.
|
AP Knee
|
|
|
When viewing a radiograph you see the tibia and fibula demonstrated with no rotation and the tibial tuberosity is in profile. A portion of the proximal head of the fibula is seen superimposed by the tibia. The outlines of the distal fibula are seen through the posterior half of the tibia. The posterior borders of the femoral condyles are superimposed. This description describes proper positioning of the _____.
|
Lateral lower leg
|
|
|
When viewing a radiograph you see the distal femur, proximal tibia and fibula with the patella superimposing the medial efmoral condyle. The lateral condyles of the femur and tibia are well demonstrated. The medial and lateral knee joints appear unequal. the tibiofibular joint is open. The head and neck of the fibular are well visualized and free of superimposition. Approximately half of the patella is seen superimposed by the femur. This description best describes proper positioning of the ______.
|
AP Medial Oblique Knee
|
|
|
When viewing a radiograph you see the distal femur, proximal tibia and fibula and patella in lateral profile. The patellofemoral joint is open. The posterior borders of the femoral condyles are directly superimposed. The knee joint is in the center of the collimated field. This description best describes proper positioning of the _______.
|
Lateral knee
|
|
|
Is the Camp Coventry method for the tangential projection of the patella?
|
No
|
|
|
Correct CR angle and centering of the tangential (axial or sunrise/skyline) projection of the patella is evidenced by _________.
|
Open patellofemoral joint
|
|
|
What is the CR angle for the plantodorsal axial projection of the calcaneous?
|
40 degrees cephalic
|
|
|
What is the CR placement for a lateral calcaneus?
|
1" inferior to the medial malleolus
|
|
|
What is the correct rotation for an oblique ankle?
|
Medial 45 degrees
|
|
|
What is the CR placement for a lateral ankle?
|
Medial malleolus
|
|
|
What three bones form the ankle joint?
|
Fibula, tibia, talus
|
|
|
What is the correct degree of rotation for a mortise ankle position?
|
Internally 15-20 degrees
|
|
|
What is the correct degree of rotation for an AP oblique ankle?
|
Internally 45 degrees
|
|
|
What is the correct CR placement for an AP ankle?
|
Midway between the malleoli
|
|
|
What is the name of the distal tibial joint surface that forms the roof of the mortise?
|
Tibial plafond
|
|
|
What is the name of the line that is formed between the medial and lateral malleoli?
|
Intermalleolar
|
|
|
How many tarsals are in the foot?
|
7
|
|
|
What is the alternate name for the calcaneous?
|
Os Calcis
|
|
|
What is the alternate name for the talus?
|
Astragalus
|
|
|
What is the CR placement for the lateral great toe
|
Interphalageal joint
|
|
|
What is the proper degree of rotation for a routine medial oblique foot?
|
30-45 degrees medially
|
|
|
what is the CR placement for a lateral foot?
|
Medial cuneiform
|
|
|
Which tendon attaches directly to the tibial tuberosity?
|
Patellar
|
|
|
True or false. The adductor tubercle is located on the posterior aspect of the medial femoral condyle?
|
True
|
|
|
This distal tib/fib joint is classified as __________.
|
Fibrous
|
|
|
To ensure that both joints are included on an AP projectioin of the tibia and fibula, the IR should be ________.
|
Positioned diagonally
|
|
|
What CR angle is required for an AP projection of the knee on a patient with an ASIS-to-tabletop measurement of 18 cm?
|
3-5" caudad
|
|
|
Which projection of the knee will best demonstrate the styloid process of the fibula?
|
AP oblique with medial rotation
|
|
|
True or false. The adductor tubercle is present on the lateral condyle and can be used to determine possible rotation of a lateral knee?
|
False
|
|
|
The posterior visibility of the adductor tubercle on a lateral knee indicates:
|
Under-rotation of knee toward IR
|
|
|
A radiograph of an AP knee reveals rotation with almost total superimposition of the fibular head and proximal tibia. What must the technologist do to correct this positioning error on the repeat?
|
Rotate the knee medially
|
|
|
A knee study is needed with special interest in the region of the proximal tibiofibular joint and the lateral condyle of the tibia. Which projections should the technologist obtain?
|
AP, Lateral, and medial oblique knee
|
|
|
What projections best demonstrate signs of Osgood-Shlatter disease?
|
AP and lateral knee
|
|
|
True or false. A 3-5" caudad CR angle should be used for an AP knee projection for patients with thick thighs?
|
False
|
|
|
True or false. The correct CR placement for an AP projection of the knee is mid-patella.
|
False
|
|
|
True or false. The intercondylar eminence is part of the distal femur.
|
False
|
|
|
Which is more distal, the medial or lateral malleolus?
|
Lateral
|
|
|
How many tarsal bones are there?
|
7
|
|
|
What is the posterior surface of the foot called?
|
Plantar
|
|
|
Where would the interphalangeal joint of the foot be found?
|
Between the phalanges of the first digit
|
|
|
What bone contains the sustentaculum tali?
|
Calcaneus
|
|
|
How many facets make up the subtalar joint?
|
3
|
|
|
Name the arches of the foot
|
Longitudinal and transverse
|
|
|
On which bone is the medial malleolus?
|
Tibia
|
|
|
Extending the ankle joint, or pointing the foot and toes downward is called _________.
|
Plantar flexion
|
|
|
How much CR angulation should be used for an AP projection of the toes?
|
10-15 degrees toward the calcaneus
|
|
|
Which studies should be performed for the 2nd toe?
|
AP, medial oblique, lateromedial lateral
|
|
|
To properly visualize the joint spaces on an AP foot, the CR must be _________.
|
Perpendicular to the metatarsals
|
|
|
Which position of the foot will best demonstrate the lateral (third) cuneiform?
|
AP medial oblique
|
|
|
What CR angulation is required for the AP oblique projection of the foot?
|
Perpendicular to IR
|
|
|
How much CR angulation is needed for the axial plantodorsal projection of the calcaneous?
|
40 degrees
|
|
|
What position is useful to evaluate acetabular fracture or hip dislocation?
|
Posterior oblique pelvis-acetabulum (Judet Method)
|
|
|
What CR angle is required for an AP foot?
|
None, CR is perpendicular to IR
|
|
|
How much CR angulation is needed for the axial plantodorsal projection of the calcaneus?
|
40 degrees
|
|
|
Where is the CR placed for a mediolateral projection of the calcaneus?
|
1 inch distal to the medial malleous
|
|
|
How much rotation, from an AP position, of the ankle will demonstrate the mortise joint?
|
15-20 degrees medially
|
|
|
Which projection of the ankle best demonstrates the distal tibiofibular joint?
|
AP oblique w/ 45 degree rotation
|
|
|
What is the alternate name for the talus?
|
Astragalus
|
|
|
How do you recognize a lateral knee that is under-rotated?
|
The fibular head will appear more superimposed by the tibia that a true lateral
|
|
|
When viewing an xray you see the tibia and fibula demonstrated with no rotation and the tibial tuberosity is in profile. A portion of the proximal head of the fibula is seen superimposed by the tibia. The outlines of the distal fibula are seen through the posterior half of the tibia. The posterior borders of the femoral condyles are superimposed. This description best describes what position?
|
Lateral lower leg
|
|
|
What is the movement type of the interphalangeal joints?
|
ginglymus or hinge
|
|
|
What is the movement type of the metatarsophalangeal joints?
|
Modified ellipsoidal or condyloid
|
|
|
What is the movement type of the tarsometatarsal joints?
|
Plane or gliding
|
|
|
What is the movement type of the intertarsal joints?
|
plane or gliding
|
|
|
What is the movement type of the ankle joint?
|
Ginglymus or hinge
|
|
|
What is the movement type of the femorotibial joint?
|
Ginglymus or hinge
|
|
|
What is the movement type of the patellofemoral joint?
|
Sellar or saddle
|
|
|
What is the movement type of the proximal tibiofibular joint?
|
Plane or gliding
|
|
|
What is the classification of the joints of the foot, ankle, leg and knee?
|
Synovial
|
|
|
What is the classification of the distal tibiofibular joint?
|
Fibrous
|
|
|
What is the mobility type of the joints of the foot, ankle, leg, and knee?
|
Diarthrodial
|
|
|
What is the mobility type of the distal tibiofibular joint?
|
Amphiarthrodial of the syndesmosis type
|
|
|
What is Paget's disease?
|
A nonneoplastic bone disease that disrupts new bone growth, resulting in an over-production of very dense, soft bone. The pelvis is the most common initial site of the disease.
|
|
|
What is Chondromalacia patellae (runner's knee)?
|
softening of the cartilage under the patella, which results in wearing away of this cartilage.
|
|
|
What is Ewing's sarcoma?
|
A common primary malignant bone tumor in children and young adults, arising from bone marrow. Bone stratifies new bone formation resulting in an "onion peel" look on xrays.
|
|
|
What is gout?
|
A form of arthritis that may be hereditary in which uric acid appears in excessive amounts in the blood and may be deposited in the joints and other tissue.
|
|
|
What is multiple myeloma?
|
Most common type of primary cancerous bone tumor. Generally affecting ages 40-70. Xray appearance is loss of calcium in bone, lesions scatted throughout the affected bones.
|
|
|
What is Osgood-Schlatter disease?
|
An inflammation of the bone and cartilage involving the anterior proximal tibia and is most common in boys 10 to 15. The cause is believe to be an injury that occurs when the large patellar tendon detaches part of the tibial tuberosity to which it is attached.
|
|
|
What is osteoarthritis?
|
Degenerative joint disease (DJD). A noninflammatory joint disease characterized by gradual deterioration of the articular cartilage with overgrown bone formation. "Normal part of aging"
|
|
|
What are osteoclastomas?
|
Giant cell tumors. Benign lesions that occur in long bones of young adults. Appear on xrays as largle "bubbles" separated by thin stripes of bone.
|
|
|
What is osteomalacia?
|
Rickets. Bone softening. Caused by a lack of bone mineralization because of a deficiency of calcium, phosphorus, and/or vitamin D or an inability to absorb these minerals.
|
|
|
What is Reiter syndrome?
|
Affects the SI joints and lower limbs of young men, on xray displays as bony erosion at the achilles tendon. Caused by a previous infection of the GI tract or STD.
|
|
|
What size cassette should be used for a RAO and lateral sternum?
|
10x12 Portrait
|
|
|
What SID should be used for an RAO sternum?
|
40"
|
|
|
What SID should be used for a lateral sternum?
|
72"
|
|
|
What breathing technique should be used for a RAO sternum?
|
Breathe regularly to blur the ribs
|
|
|
What type of breathing technique is used for a lateral sternum?
|
Suspend on inspiration
|
|
|
WHat marker should be used for a RAO sternum?
|
Left, anatomically correct b/c the sternum is projected over the left side (in heart shadow)
|
|
|
Where is the CR for an RAO sternum?
|
Midway between the juglar notch and the xiphoid process, which is about the level of the inferior angle of the scapula
|
|
|
How much obliquity is needed for an RAO sternum?
|
15-20 degrees
|
|
|
A patient has an upper right anterior rib injury, what marker should be used and what position would best demonstrate the area of interest?
|
LAO, using right marker to indicate the side of injury
|
|
|
True or false. Each clavicle joins the manubrium lateral to the jugular notch of the sternum.
|
True
|
|
|
True or false. The anterior ribs articulate with the sternum via the costovertebral cartilage.
|
False, via the costocartilage
|
|
|
True or false. The 3rd through 7th costocartilages connect directly to the body of the sternum.
|
True
|
|
|
True or false. The 3rd through 7th ribs connect directly to the body of the sternum.
|
False, connect via costocartilage
|
|
|
True or false. The vertebral end of the rib consists of a head, neck and tubercle.
|
True
|
|
|
The head of the rib articulates with the _________.
|
Vertebral body
|
|
|
The bony thorax is widest at the lateral margins of the ________.
|
8th and 9th ribs
|
|
|
True or false. The sternoclavicular joint is synovial with a gliding motion and therefore is synarthrodial.
|
False. It is synovial and diarthrodial.
|
|
|
True or false. The sternocostal joint of the 1st rib allows no motion.
|
True
|
|
|
True or false. The average rotation of the thorax is 15-20 degrees into the LAO position for a PA sternum.
|
False, RAO sternum.
|
|
|
True or false. The degree of obliquity for an RAO sternum depends on the size of the thorax.
|
True
|
|
|
True or false. For xrays of the ribs above the diaphragm the patient should be erect and suspend respiration on inspiration.
|
True
|
|
|
True or false. For xrays of the ribs below the diaphragm medium kvp should be used (75-85).
|
True
|
|
|
The RAO position for the sternoclavicular joints best demonstrates which joint?
|
Right joint
|
|
|
The LAO position for the sternoclavicular joints best demonstrates the ________ (upside or downside)?
|
Downside
|
|
|
The CR for ribs above the diaphragm is __________.
|
3-4 inches below the jugular notch
|
|
|
The CR for ribs below the diaphragm is ____________.
|
Midway between the xiphoid process and the lower rib cage
|
|
|
The CR for anterior obliques of the sternoclavicular joints is perpendicular and at the level of T2-T3 and 1-2" lateral (toward the side up) to the MSP. True or false.
|
True
|
|
|
True or false. The CR for PA sternoclavicular joints is perpendicular and at the level of T2-T3 or 3 inches distal to the vertebral prominens.
|
True
|
|
|
True or false. Each clavicle joins the manubrium medial to the jugular notch of the sternum.
|
False
|
|
|
True or false. The anterior ribs articulate with the sternum via the costocartilage.
|
True
|
|
|
True or false. The 1st – 10th ribs connect directly to the body of the sternum.
|
False
|
|
|
True or false. The sternal end of the rib consists of a head, neck and tubercle.
|
False
|
|
|
True or false. The sternoclavicular joint is synovial joint with a gliding motion, and therefore is synarthrodial.
|
False, it is synovial and diarthrodial with plane (gliding) movement type
|
|
|
What kVp should be used for ribs above the diaphragm?
|
Low, 65-75 kVp
|
|
|
What are the terms used for the middle, long portion of the sternum?
|
Body, Corpus, Gladiolus
|
|
|
The most distal aspect of the sternum does not generally ossify until a person is approximately _____ years of age?
|
39-45 years
|
|
|
A. Medial Condyle
B. Lateral Condyle C. Adductor Tubercle D. Patellofemoral joint space E. Intercondylar eminence |

Name the labeled parts
|
|
|
1. Adductor Tubercle
2. Medial Femoral condyle 3. Tibial Plateau 4. Neck of the fibula 5. Lateral femoral condyle |
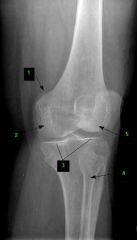
Name the labeled anatomy
|
|
|
A. Ala of Ilium
B. Acetabulum C. Femoral Head D. Greater Trochanter E. Femoral Neck F. Ischial Spine G. Superior Ramus of Pubis H. Inferior Ramus of Pubis I. Symphysis Pubis J. Ischial Tuberosity K. Body of Ischium L. Anterior Superior Iliac Spine M. Iliac Crest |

Name the labeled anatomy
|
|
|
1. Dens
2. Posterior arch and tubercle of Atlas 3. Body of C3 4. zygapophyseal joint between C4-5 5. Spinous process of C7 |

Name the labeled anatomy
|
|
|
A. Neck
B. Head C. Tubercle D. Angle E. Costal groove F. Sternal End G. Body |
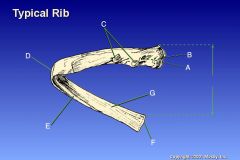
Name the labeled anatomy
|