Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
40 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
POM Lec 11: Sepsis |
POM Lec 11: Sepsis
|
|
|
|
Typical Sepsis Case:
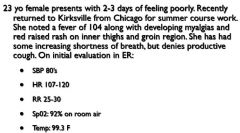
23 yo female presents with 2-3 days of feeling poorly. Recently returned to Kirksville from Chicago for summer course work. She noted a fever of 104 along with developing myalgias and red raised rash on inner thighs and groin region. She has had some increasing shortness of breath, but denies productive cough. On initial evaluation in ER: • SBP 80’s • HR 107-120 • RR 25-30 • Sp02: 92% on room air • Temp: 99.3 F |
Typical Sepsis Case:
23 yo female presents with 2-3 days of feeling poorly. Recently returned to Kirksville from Chicago for summer course work. She noted a fever of 104 along with developing myalgias and red raised rash on inner thighs and groin region. She has had some increasing shortness of breath, but denies productive cough. On initial evaluation in ER: • SBP 80’s • HR 107-120 • RR 25-30 • Sp02: 92% on room air • Temp: 99.3 F |
|
|
|
1st: Realize that sepsis is part of a continuum consisting of 4 stages, all resulting the body's response to something that is irritative to the body:
1. SIRS (Systemic Inflamm Response Syndrome) 2. Sepsis 3. Severe Sepsis 4. Septic Shock |
1st: Realize that sepsis is part of a continuum consisting of 4 stages, all resulting the body's response to something that is irritative to the body:
1. SIRS (Systemic Inflamm Response Syndrome) 2. Sepsis 3. Severe Sepsis 4. Septic Shock |
|
|
|
Let's Define the Stages on the Previous Card & Give their Criteria:
1) SIRS (Systemic Inflamm Response Syndrome)? 2) Sepsis? 3) Severe Sepsis? 4) Septic Shock? |
1) When an infectious or non-infectious "irritant" -->
Inflamm Response --> Damage to the body (Note: It's the actual inflammatory response that causes the damge, not the infxn!) Criteria - Need 2 or More: 1. Temp: > 38 C or < 36 C 2. HR: > 90/min 3. RR: > 20 / min OR PaCO2 < 32 mmHg 4. WBC: > 12,000 OR < 4,000 OR > 10% bands 2) When criteia for dx of SIRS are met + evidence or Infxn in either the blood and tissues or just the tissues alone **NOTE: Tachypnea and Tachycardia may be the only 2 SIRS criteria you have - and that's OK*** 3) When the criteria for Sepsis are met + Organ Dysfnctn (Possible MODS) 4) Subset of severe sepsis. Criteria: 1. Sepsis + SBP < 90 mmHg OR MAP < 65 OR SBP Decreases > 40 mmHg + DESPITE ADEQUATE FLUID RESUSCITATION |
|
|
|
In the previous slide, we said that the definition of sepsis was:
When criteia for dx of SIRS are met + evidence or Infxn. 1. What are the 3 MC locations that this infxn will come from? 2. In a later slide, we will mention how ppl in sepsis will develop dysfnctnl mitochondria. Dysfnctnl mitochondria will lead to what, which can be a clinical indicator that sepsis is occuring? 3. How people will respond to any infxn can be understood with the mnemonic PIRO. What does PIRO stand for and give details of them? |
1. Respiratory Infxn
GU Infxn ABD Infxn 2. Dyscnftnl mitchondria --> No more aerobic respiration --> Anaerobic Respiration --> INC LACTATE Levels 3. P:Predisposition to infxn A) Pts w/ TNF-beta2 and TLR 4 Asp299Gly are predisposed to what? I: Infxn type A) It is impt to determine whether the infxn is what? R: Response of pt to that infxn A) 3 Things you should give these pts? O: Organ dysfnctn present? A) Most important thingin organ dysfnctn? |
P:
A) Septic Shock I: A) Viral, Bacterial, Fungal, etc... R: A) Corticosteroids, Fluids, Broad Spec ABX early bc longer they are HYPO-tnsive, the worse their survival rate O: A) Recognize it early |
|
|
It's the _______ @ the end of the sepsis progression that kills pts?
|
MODS (Multiple Organ Dysfnctn Syndrome)
|
|
|
|
A Few #s:
1) Sepsis is the # ____ cause of death? 2) 64.9% of Septic PTs were _____ old and had a 13.1 RR comp'd to younger pts? |
1) #10 Cause of Death
2) 65 y/o |
|
|
|
NOTE: page 5, slide 4 has a list of assoc s/s seen in sepsis. "The Update" - look @ if you think it may help
|
NOTE: page 5, slide 4 has a list of assoc s/s seen in sepsis. "The Update" - look @ if you think it may help
|
|
|
|
The Pathophys of Sepsis is complex: Here are some of the major players you should be familiar w/:
1. Gram Negs w/ Endotoxin / LPS 2. Gram Pos w/ Lipotechoic and Super-Ag (TSST) 3. IL-1, IL-6, IL-12, TNF, IFN-gamma 4. Toll Like Receptors 5. PRO C 6. NO 7. Mitochondrial Dysfnctn & PARPs (Poly-ADP-Ribosyl-Polymerase) 8.. GENETICS!! |
The Pathophys of Sepsis is complex: Here are some of the major players you should be familiar w/:
1. Gram Negs w/ Endotoxin / LPS 2. Gram Pos w/ Lipotechoic and Super-Ag (TSST) 3. IL-1, IL-6, IL-12, TNF, IFN-gamma 4. Toll Like Receptors 5. PRO C 6. NO 7. Mitochondrial Dysfnctn & PARPs (Poly-ADP-Ribosyl-Polymerase) 8.. GENETICS!! |
|
|
|
The previous slide mentioned Mitochondrial Dysfnctn and PARPS as part of the pathophysiology of sepsis.
Give the steps of mitochondrial dysfnctn, which is part of the pathophysiology of sepsis? This is AKA what? This may be responsible for what? |
Stim of PARPS -->
Dec NAD --> Inability of Mitochondria to Use O2 --> Dec TCA / Kreb's Cycle --> Mitochondrial Dysfnctn Cytopathic Hypoxia Continued decline of pts even after restoration of nomrla PO2 tissue levels |
|
|
|
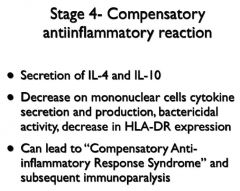
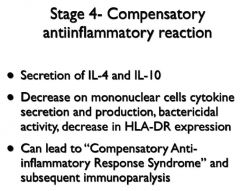
Can you list the 5 stages in the pathophysiology of sepsis?
|
1. Infxous Insult to susceptible host
2. Preliminary systemic response 3. Overwhelming systemic response 4. Compensatory antiinflammatory rxn 5. Immunomodulatory failure |
|
|
|
The Following Gives the Actual Slides with all the details about Pathophys. Maybe Just Glance Through it to be familiar, but I def don't think you should memorize it.
|
The Following Gives the Actual Slides with all the details about Pathophys. Maybe Just Glance Through it to be familiar, but I def don't think you should memorize it.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
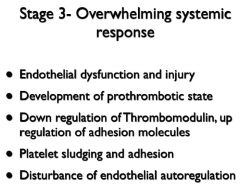
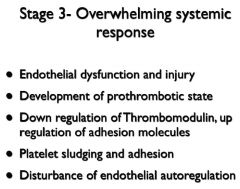
Slide 3 of the pathogenesis says that septic pts can develop a pro-thrombotic state.
Why does this happen? |
BC you will have consumption of coagulation inhibitors AND up-regulation of procoags
|
|
|
|
|
|
|
Sepsis Case
|
|
|
|
|
|
|
|
|
|
|
|
|
Lec 12: Shock
|
Lec 12: Shock
|
|
|
|
1. What does the following define:
Profound and Widespread reduction of EFFECTIVE tissue perfusion that @ first causes reversible and eventually causes irreversible injury 2. What does the following define: |
1. Shock
2. Syndrome in which TISSUE PERFUSION is reduced & blood flow is INADEQUATE to meet cellular reqs. |
|
|
|
List 7 s/s that are common to all forms of shock (septic, hypovolemic, cardiogenic, extra-cardiac obstructive, distributive)?
|
MAP < 60 in adults
Hypo-TN: Usually but NOT always Tachy Cool Extremities, but MAY be warmer in later stages Oliguria from no kidney perfusion Cloud sensorium Elevated Lactate |
|
|
|
Give the 5 major variables that determine Oxygen Delivery (DO2)?
|
CO (HR X SV)
HGB SaO2 |
|
|
|
What Do The Following Define:
1) A type of shock due to decreased circulating blood volume in relation to the total vascular capacity and characterized by a reduction of diastolic filling pressures 2) A type of shock due to cardiac pump failure related to loss of myocardial contractility/functional myocardium or structural/ mechanical failure of the cardiac anatomy and characterized by elevations of diastolic filling pressures and volumes 3) due to obstruction to flow in the cardiovascular circuit and characterized by either impairment of diastolic filling or excessive afterload 4) caused by loss of vasomotor control resulting in arteriolar/venular dilatation and characterized (after fluid resuscitation) by increased cardiac output and decreased SVR |
1) Hypovolemic shock
2) Cardiogenic shock 3) Extra-Cardiac Obstructive Shock 4) Distributive Shock |
|
|
|
Hypovolemic Shock:
What are 4 Causes of Hypovolemic Shock? |
1) Hemorrhagic Fluid Depletion
2) Non-Hemorrhagic Fluid Depletion (vomit, diarrhea,etc...) 3) Inc vasc capacitance (vasodilation from inc NOP or Dec Vasopressin and Cortisol) |
|
|
|
1) The most important cause of distributive shock is what?
2) Another common cause of distributvei shock is what? Other causes of distributive shock listed: Toxic Shock Syndrome Anaphylactic, Anaphylactoid Neurogenic Toxic |
1) Septic shock (bacterial, fungal, viral, rickettsial) -->
Myocardial depression!!!!!!! 2) NO! |
|
|
|
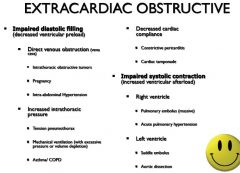
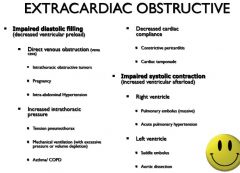
1) 2 major causes of extracardiac obstructive shock?
A) 2 major causes of impaired diastolic filling? |
1) Impaired diastolic filling, impaired systolic contraction
A) Intra-ABD HTN; Tension Pneumothorax (see pics in notes) |
|
|
|
|
|
|
|
An endocrinoloogic shock is a combination of what 2 types of shock?
2 ets of endocrinological shock? |
Cardiogenic and Distributive
Adrenal Insuffic & Thyroid Disorder |
|
|
|
Lec 13: Shock Tx!
|
Lec 13: Shock Tx!
|
|
|
|
NOTE:
When you see that someone is in shock, you must do a PE and Tx simultaneously! - Get good IV access! |
NOTE:
When you see that someone is in shock, you must do a PE and Tx simultaneously! - Get good IV access! |
|
|
|
1) What are the 3 Tx goals for tx-ing shock?
2) What is the critical BP Equation you need to understand in order to Tx shock? |
1) Fluid Resuscitation: to inc SV
Vasopressor Therapy: to inc perfusion pressure and contractility Inotropic Therapy: to increase contractility 2) BP = CO X SVR CO = HR X SV *SVR ( Systemic Vascular Resistence) *SV = Stroke Volume |
|
|
|
Remember from last lecture,you want to tx the pt to a MAP of what?
|
MAP > 60 mm Hg
|
|
|
|
Fluid Resuscitation:
1) 2 Types agents for fluid resuscitation? 2) When a pt comes in and is in ANY kind of shock, what should your first tx be? |
1) Crystaloids and Colloids:
Saline and Albumin 2) Volume Replacement!!!!!!! |
|
|
|
Vasopressors:
1) Dopamine A) @ low dose Dop binds what and does what? B) @ Med - High Dose Dop Binds what and does what? C) @ High Dose Dop binds what and does what? 2) Nor-Epi A) MOA? B) CU? C) More potent than what? 3) Epi A) MOA of epi? B) Inc what 4 things? 4) Phenyl-ephrine A) MOA of phenyl-ephrine? B) Good if what else is present w/ shock? C) 1 AE of phenylephrine? 5) Vasopressin (ADH) A) 2 MOA of vasopressin? B) AE? 6) Dobutamine A) MOA of dobutamine? B) AE of dobutamine? 7) Phosphodiesterase Inhib - Milrinone A) MOA of PDI Inhib? B) AEs? |
1)
A) DA1, DA2 --> Vasodilation B) beta I --> Inc Contractility and HR C) alpha --> Vasoconstriction 2) A) alpha ag; moderate beta ag B) Inc BO w/out adverse FX C) Dopamine 3) A) Alpha and beta ags B) CI, SV, HR, SVR 4) A) alpha-1 ag B) Tachyarrhythmias C) Inc O2 Consumption 5) A) Stim ACTH --> better renal blood flow; Sensitizes catecholamine receptors B) Coronary Ischemia 6) A) beta-1 Agonist --> Inc CO and Contractility B) Arrhythmias - esp tachyarrhythmias and vasodilation 7) A) Inc cAMP --> Inc IC Ca --> Inc force of contraction A) Hypo-TN; Tachyarhythmias, but less than dobutamine |
|
|
|
|
|
|
|
Rickelman's Review: HE gave away 1 test question.
1) PT w/ BP 70/40 back from elective surgery. CO = 2.4. SVR = 1400. What is your first step? |
1) VOLUME REPLACEMENT
NOTE: 1. Norm CO = 4 2. Norm SCR = 1,000 3. In this case CO was low and SVR was high, TF according to BP = CO X SVR & CO = SV X HR, if you Inc the Col --> Inc SV --> Inc CO --> Inc BP 4. 1st step for ANY shock pt is fluid replacement!!! |
|