![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
137 Cards in this Set
- Front
- Back
|
Define motility. |
the movements of the GI tract that propel food along the gut and are involved in the mixing of food to aid digestion and absorption |
|
|
Describe the basic muscular structure of the GIT |
smooth muscle outer longitudinal layer inner circular layer |
|
|
Describe the musculature of the oesophagus. |
upper third--skeletal middle third--mix of skeletal and smooth lower third--smooth |
|
|
How does GIT smooth muscle function and why? |
syncytium--smooth muscle cells are electrically connected to each other via gap junctions |
|
|
What happens when circular smooth muscle layers contract? |
reduces diameter of lumen increases length |
|
|
What happens when longitudinal smooth muscle layers contract? |
shortens segment expands lumen |
|
|
How does peristalsis move a bolus of food to the stomach? |
alternating waves of contraction and relaxation circular muscle behind bolus contract circular muscle of the receiving segment relaxes |
|
|
Which muscle sphincters are skeletal? |
upper esophageal external anal |
|
|
Which muscle sphincters are smooth muscle? |
lower oesophageal pyloric oddi ileocecal internal anal |
|
|
What does parasympathetic stimulation to to the gut? |
increases gut motility increases secretions |
|
|
What does sympathetic stimulation do to the gut? |
decreases gut motility decreases secretions |
|
|
The enteric nervous system is composed to 2 plexuses. What are they? |
1) myenteric plexus 2) submucosal plexus |
|
|
What is the myenteric plexus and what does it control? |
--outer plexus between longitudinal and circular muscle layers --control motility |
|
|
What is the submucosal plexus and what does it control? |
--inner plexus in submucosa
--controls glandular secretions, local blood flow and absorption |
|
|
The enteric NS can function ____ and can be modulated by the ___. |
can function autonomously modulated by autonomic NS |
|
|
What controls the smooth muscle sphincters? |
enteric and autonomic nerves |
|
|
Describe the the stomach's storage function. |
stretch triggers vagovagal reflex from the stomach --> brain --> to stomach reduces contraction--accomodate large volumes |
|
|
What is the peristaltic contraction rate set by? |
gastric pacemaker cells--interstitial cells of Cajal |
|
|
What are hunger pains? |
peristaltic contractions of empty stomach |
|
|
What is the inherent rhythm of motility in the small intestine set by? |
set by gut modified by hormones, enteric NS, autonomic NS |
|
|
What are the contractions of the small intestine? |
mixing segemnting |
|
|
What are migrating myoelectric complexes? |
After most of a meal has been absorbed... --segmenting contractions cease --replaced by peristaltic activity--migrating myoelectric complexes --start at lower portion of stomach --activity spreads down sm intestine over 2 hours --when reaches end of small intestine, new waves begin at stomach |
|
|
What is the purpose of migrating myoelectric complexes? |
--move undigested material to large intestine --prevents bacterial overgrowth |
|
|
How long does material take to move from ileocecal sphincter to the rectum? |
~12-24 hours |
|
|
What are the motility patterns of the large intestine designed to do? |
dehydrate compact store eleminate faeces |
|
|
What are the contractions in the large intestine called? |
haustral contractions |
|
|
What are haustral contractions? |
segmental pattern of motility initiated by stretch of matter entering large intestine programmed by myenteric plexus ring segments of circular & longitudinal muscle contract--bulging of unstimulated regions--haustratons |
|
|
What are mass movements of the large intestine? |
long, slow moving and powerful contractions that sweep over large segments from caecum to sigmoid colon |
|
|
How many mass movements of the large intestine are there per day? |
3-4 |
|
|
Describe the mass movements of the large intestine. |
constrictive ring occurs and distal loss of hausfrau with contraction as a uni ~30 sec |
|
|
What are mass movements of the large intestine facilitated by? |
gastrocolic and duodenocolic reflexes stretch of stomach and duodenum mediated by ANS |
|
|
What signals the need to defecate? |
mass movements of faeces into the rectum activates stretch receptors distension leads to activation of enteric NS causing relaxation of internal anal sphincter |
|
|
What are the signals that are involved in the defecation? |
afferent signals --> spinal cord --> spinal reflex parasympathetic fibres stimulate the contraction of the rectum and sigmoid colony and the relaxation of the internal anal sphincter |
|
|
What part of the NS is involved with voluntary control over defecation? |
somatic innervation of the external anal sphincter |
|
|
What is the chart called for characterising stool and what are the two extremes? |
Bristol stool chart constipation and diarrhoea |
|
|
Poor motility in the colon leads to what? |
greater time for absorption hard faeces & constipation |
|
|
Excess motility in the colon leads to what? |
less time for absorption of fluids loose faeces and diarrhea |
|
|
What are treatments for constipation? |
'normal cases'--bulk-forming laxatives & high fibre diet 'severe cases'--osmotic & stimulant laxatives, manual evacuation (enema) |
|
|
What are the 4 mechanisms of diarrhoea? |
1) osmotic--large quantities of non-absorbed hypertonic substances in lumen 2) secretory--active secretion of fluid, electrolytes and decreased absorption 3) inflammatory--musocal damage --> loss of fluid & blood; defective absorption of fluid & electrolytes 4) abnormal motility |
|
|
How is diarrhoea treated? |
treat underlying cause oral fluid & electrolyte replacement |
|
|
What is a congenital cause of constipation? |
Hirschsprung's disease |
|
|
What is Hirschsprung's disease? |
congenital cause of constipation --aganglionic segment of distal colon--megacolon --no defication reflexes in affected areas--no strong peristaltic motility --affected area contracts, with accumulation of large amounts of faecal matter proximal to area |
|
|
How does Hirschsprung's disease present? |
failure to pass a stool within the first 48 hours of life |
|
|
How is Hirschsprung's disease diagnose? |
biopsy stained for ganglion cells and acetylcholinesterase which is elevated in the disease state |
|
|
What is the treatment for Hirschsprung's disease? |
surgical removal of aganglionic section |
|
|
What is gastroparesis? |
delayed gastric emptying poor/loss of propulsive motility |
|
|
What causes gastroparesis? |
commonly due to diabetic autonomic neuropathy |
|
|
How is gastroparesis treated? |
medications that stimulate motility liquefied/pureed diet, smaller more frequent meals botox on pyloric sphincter |
|
|
What is dysphagia? |
the sensation of obstruction during passage of liquid or solid through the pharynx or esophagus |
|
|
What are the common causes of dysphagia? |
1) diseases of mouth & tongue--ex: tonsillitis 2) neuromuscular disorders 3) esophageal motility disorders 4) extrinsic pressure--ex: goitre 5) intrinsic lesions--ex: outpouchings of oesophagus & pharyngeal wall |
|
|
What is achalasia? |
failure of the lower oesophageal sphincter to relax during swallowing |
|
|
What causes achalasia? |
degeneration of the neural network of the myenteric plexus |
|
|
How is achalasia treated? |
no cure endoscoptic dilation of sphincter with ballot to weaken sphincter endoscopic injection of botox surgery |
|
|
Describe the pathways that lead to vomiting. |
coordinated by vomiting centre in medulla and sensory signals to nuclei of the centre motor impulses from vomiting centre cause wave of reverse peristalsis that begins in small intestine |
|
|
Describe the coordination of the pathways during vomiting. |
1) excessive salivation 2) initial deep breath 3) respiration inhibited 4) epiglottis & soft palate close off trace & nasopharynx 5) strong downward contraction of diaphragm and contraction of abdominal muscles 6) relaxation of lower esophageal sphincter |
|
|
What organs in the GIT secrete things? |
salivary glands stomach pancreas liver small intestine large intestine |
|
|
What are the functions of secretions in the GIT? |
digestive enzymes mucous--lubrication & protection (including immune) |
|
|
In adults, about how much fluid is added to the GI tract daily as secretions to aid digestion and absorption of nutrients? |
~7L |
|
|
What are the three controls of secretions? |
1) local--tactile, distension, irritation 2) reflex--nervous input 3) hormonal--GI hormones |
|
|
What are the 3 pairs of extrinsic (outside oral cavity) salivary glands that produce most of the saliva? |
parotid submandibular sublingual |
|
|
Wat are the intrinsic (minor) salivary glands in the oral cavity? |
buccal and others |
|
|
What are the two secretory cell types of salivary glands? |
serous--watery--enzymes & ions mucous--mucous--stringy & viscous |
|
|
what are the two types of protein secreted by salivary glands? |
serous--alpha amylase--starch digestion mucous--mucin--lubrication, surface protection |
|
|
What are the functions of saliva? |
1) lubrication 2) digestion 3) protection 4) control of H2O intake 5) speech 6) absorption 7) taste sensation |
|
|
Describe the nervous regulation of salivary secretion. |
higher centres in the brain communicate with salivary nuclei in the medulla oblongata with communicates with the salivary glands. |
|
|
What is the parasympathetic affect on salivation? |
increased rate of secretion |
|
|
What is the sympathetic affect on salivation? |
decreased rate of secretion |
|
|
Salivation What stimuli activate higher centre in the brain? |
sight, sound, thought |
|
|
Salivation What stimuli activate the salivary nuclei in the medulla oblongata? |
taste, smell, chewing, object in mouth |
|
|
Pharmacologically, how is excessive salivation treated? |
low dose muscarinic receptor antagonists |
|
|
Pharmacologically, how is insufficient salivation treated? |
low dose muscarinic receptor agonists |
|
|
What are the two tubular glands of the stomach and the location of each? |
gastric/oxynic glands--proximal 80% of stomach pyloric glands--distal 20% of stomach |
|
|
What do gastric/oxyntic glands secrete? |
HCl pepsinogen intrinsic factor mucous |
|
|
What do pyloric glands secrete? |
mucous |
|
|
What are the 4 main types of secretory cells of the gastric glands? |
mucous parietal--oxyntic chief--peptic enteroendocrine--D cells--somatostatin |
|
|
What are the 3 types of secretory cells of pyloric glands? |
mucous chief enteroendocrine |
|
|
What do mucous neck cells secrete? |
mucus |
|
|
What do parietal cells secrete? |
HCl intrinsic factor |
|
|
What do enterochromaffin-like cells secrete? |
histamine |
|
|
What do chief cells secrete? |
pepsinogen gastric lipase |
|
|
What do D cells secrete? |
somatostatin |
|
|
What do G cells secrete? |
gastrin |
|
|
How much acid secretion occurs in the stomach per day? |
1-3 L |
|
|
What is the luminal pH of the stomach? |
<1 |
|
|
What is the cytoplasmic pH of parietal cells? |
~7.2 |
|
|
Name 4 neurohumoral factors that regulate acid secretion in parietal cells. |
stimulatory--histamine, gastrin, acetylcholine inhibitory--somatostatin |
|
|
What is a non-neurohumoral factor that stimulates gastric acid secretion? |
caffeine |
|
|
How do you treat excess gastric acid secretion? |
proton pump inhibitors |
|
|
What does pepsin do? |
accelerate digestion of protein |
|
|
How is pepsinogen activated? |
cleaved to pepsin by acid generated from parietal cells |
|
|
How is the stomach protected from the corrosive acidic gastric juice? |
mucosal barrier--layer of HCO3 tight junctions prevent leakage into underlying tissues rapid cell division to replace damaged epithelial cells--new stomach lining every 3-5 days |
|
|
How often is the lining of the stomach replaced? |
every 3-5 days |
|
|
Where the the 3 different sites of stimulation to activate of inhibit gastric secretions? |
head stomach small intestine |
|
|
What are the phases of gastric secretion? |
cephalic gastric intestinal |
|
|
What are the stimulatory and inhibitory events of the cephalic phase? |
stim--sight and thought of food, stimulation of taste and smell receptors inhib--loss of appetite, depression |
|
|
What are the stimulatory and inhibitory events of the gastric phase? |
stim--stomach distension activates stretch receptors, food chemicals and rising pH activate chemoreceptors inhib--excessive acidity, emotional upset |
|
|
What are the stimulatory and inhibitory events of the intestinal phase? |
stim--presence of low pH, partially digested foods, fats, or hypertonic solution in duodenum when stomach begins to empty inhib--distension of duodenum, presence of fatty, acidic, hypertonic chyme and/or irritants in duodenum |
|
|
What are the causes of gastric and duodenal ulcers? |
1) high acid and pepsin content 2) irritation of mucosa 3) poor blood supply 4) poor mucous secretion 5) infection--H pylori |
|
|
What are the exocrine and endocrine secretions of the pancreas? |
exo--pancreatic juice endo--insulin & glucagon |
|
|
What is pancreatic juice and its function? |
alkaline--pH 8 neutralise acid chyme entering duodenum provides optimal environment for intestinal and pancreatic enzymes |
|
|
What do pancreatic enzymes do? |
digest all food types |
|
|
What are the inactive proteolytic enzymes of the pancreas? |
trypsinogen chymotrypsinogen procarboxypoypeptidase elastase--prevents autodigestion |
|
|
What are the active enzymes of the pancreas? |
lipase cholesterol esterase phospholipase--fats amylase--carbs ribonuclease--nucleic acids deoxyribonuclease--nucleic acids |
|
|
What cleaves trypsingoen activating it? |
enterokinase/enteropeptidase on intestinal epithelial cells |
|
|
What does trypsin cleave/activate? |
chymotripsinogen procarboxypeptidase |
|
|
How else can trypsinogen be activated other than by enterokinase/enteropeptidase? |
autocatalytically by trypsin |
|
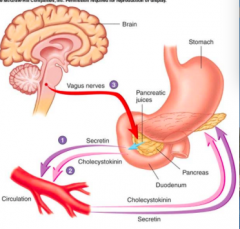
Describe what is happening at 1, 2 and 3 |
1) secretin is released from duodenum--stimulates pancreas to secrete bicarb 2) cholecystokinin is released from duodenum--stimulates pancreas to release digestive enzymes 3) parasympathetic tim from vagus nerve--stimulates pancreas to release digestive enzymes |
|
|
What is the role of the liver in digestion? |
secretion of bile |
|
|
What does bile do? |
role in fat digestion and absroption |
|
|
How does bile help digestion/absorption? |
emulsifies fat into smaller particles in order to enhance action of pancreatic lipase |
|
|
What is the composition of bile? |
water bile salts bile pigments--bilirubin cholesterol lecithin--phospholipid--forms micelles electrolytes |
|
|
What are orexigenic signals? |
increase feeding ghrelin |
|
|
What are anorexigenic signals? |
decrease feeding leptin |
|
|
What are some hormones that reduced food intake? |
cholecystokinin, peptide YY--released in response to nutrients in GIT insulin--stimulated by increased blood glucose leptin--produced by white adipose tissue |
|
|
What are the feeding and satiety centres of the hypothalamus? |
lateral hypothalamus--feeding vetromedial and arcuate nuclei--satiety |
|
|
Neurons in the arcuate nuclei of they hypothalamus. which suppress appetite and increase energy expenditure |
pro-opiomelanocortin cocain and amphetamine related transcript |
|
|
Neurons in the arcuate nuclei of they hypothalamus. Which increase food intake and decrease energy expenditure |
neuropeptide Y agouti-related protein |
|
|
describe the feedback control of leptin. |
fat cells produce leptin --> acts on receptors in hypothalamus 1) --> increases sympathetic activity --> increases thermogenesis 2) --> decreases food intake |
|
|
How is the feedback control of leptin altered in obesity? |
food intake doesn't decrease sympathetic activity doesn't trigger increased metabolism |
|
|
What is the set-point hypothesis? |
presence of regulatory system for feeding & fasting behaviour in the CNS suggests a set point for energy levels, body weight and metabolism body defends this level |
|
|
How much cardiac output does the liver receive? |
25% |
|
|
What are some of the functions of the liver? |
1) glycogen storage 2) protein synthesis 3) detox 4) red cell destruction 5) hormone production 6) immunity 7) lipid emulsification 8) maintenance of blood glucose levels 9) regulates blood lipids |
|
|
What is the dual blood supply of the liver? |
hepatic portal vein--75% hepatic arteries--25% |
|
|
What to hepatocytes synthesize? |
bile salts cholesterol lecithin bile pgments |
|
|
Liver where does the portal vein blood come from? |
spleen stomach pancreas small intestine colon |
|
|
Liver where does the hepatic artery branch off from? |
celiac artery |
|
|
Liver what are the low resistance cavities called that blood perfuses through? |
sinusoids |
|
|
What is the pathway of flow of bile from the liver to the duodenum? |
bile --> canaliculi --> bile ductule --> hepatic duct --> common hepatic duct --> common bile duct --> duodenum |
|
|
During meals, what sphincter is open to allow bile to go into the duodenum? |
sphincter of oddi |
|
|
What is the enterohepatic circulation and its pathway? |
recycles bile salts liver --> intestine --> liver via enterohepatic circulation bile salts are absorbed by mass action |
|
|
How much of the bile salts are broken down by bacteria in the ileum and lost in faeces? |
5% |
|
|
what is the bile acid dependent fraction of hepatocytes? |
bile acids produced by liver and recirculated from blood conjugated with glycine or taurine to increase H2O solubility |
|
|
What is the bile acid independent fraction of hepatocytes? |
generation of bicarb ions |
|
|
What is jaundice? |
accumulation of yellow bile pigments in the blood |
|
|
What do cholesterol gallstones look like? |
pale |
|
|
What do bie pigment stones look like? |
black--calcium bilirubiinate brown--calcium salts of fatty acids & calcium bilirubinate |
|
|
Liver
which is reversible and which is irreversible fibrosis, cirrhosis |
fibrosis--reversible cirrhosis--irreversible |