![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
134 Cards in this Set
- Front
- Back
|
What function does the folding serve in the cerebrum? |
Increases the surface area, allowing more cell bodies (grey matter) |
|
|
What is the name of the main structure connecting left and right cerebral hemispheres? |
Corpus Callosum |
|
|
Do sensory and motor regions of the cortex 'talk' to one another? |
Yes. Most of the neurones in the cerebrum are fully contained within the cortex. |
|
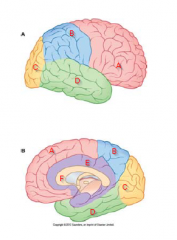
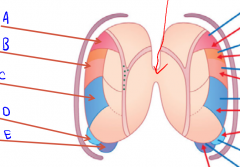
Label A-F |
A- Frontal lobe B - Parietal Lobe C - Occipital Lobe D - Temporal Lobe E - Limbic Lobe F - Corpus Callosum |
|
Label A - E |
A - Central sulcus B - Lateral fissure C - Parieto-occipital sulcus D - Calcarine salcus E - Corpus Callosum |
|
|
What is a commisural fibre? |
A fibre which passes from one hemisphere to another |
|
|
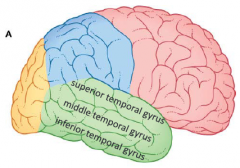
What gyri are contained within the temporal lobe? |
|
|
|
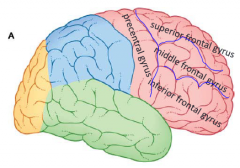
What gyri are contained within the frontal lobe? |
|
|
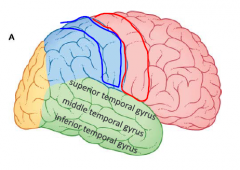
Label the highlighted gyri |
Blue - Post central gyri Red - Pre central gyri |
|
|
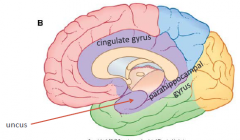
What are the gyri of the limbic lobe? |
|
|
|
Why do we associate certain smells with certain emotions? |
Because the olfactory (smell) centre is situated in the limbic lobe which is where emotional processing occurs |
|
|
What are Brodmann's areas? |
Brodmann divided the cortex in to 47 areas which he numbered and listed functions for |
|
|
What is the difference between primary and association cortices? |
Primary cortex is the simplest level of processing, whereas association cortex is a higher level of processing E.g. primary motor cortex can initiate muscle contractions but without association cortex cannot perform meaninful movements. |
|
|
What function does the post-central gyrus serve? |
Primary sensory cortex |
|
|
How is the primary sensory cortex organised? |
Somatotopic ordering. This means it is ordered based on anatomical location. E.g. Foot is near leg and hip, but not near hand. |
|
|
Roughly where is Wernicke's area located? |
In the temporal lobe, near the primary auditory area |
|
|
What is the specific function of Wernicke's area. What is it called when this area is damaged? |
Comprehension of speech. Damage to this area means the patient is unable to comprehend speech and this is known as Receptive Aphasia |
|
|
Which lobe contains the visual cortex? How is the area organised? |
Occipital lobe - organised retinotopically. This means that adjacent areas of the cortex contain information from adjacent areas of retina. |
|
|
Specifically where is the primary visual cortex and association visual cortex located? |
Primary cortex - located in the occipital lobe adjacent to the calcarine sulcus on either side. Mostly medial. Association cortex - remaining parts of the occipital lobe |
|
|
What function does the precentral gyrus serve? |
The primary motor cortex is contained here. |
|
|
What are the 3 sections of the association motor cortex? |
Supplementary motor cortex Premotor cortex Broca's area |
|
|
Specifically, where is Broca's area located? |
Just anterior to the face and throat regions on of the primary motor cortex. This is usually only located in one hemisphere |
|
|
Which association motor cortex has the most connections to the cerebellum? |
The premotor cortex. |
|
|
How is the auditory cortex organised? |
Tonotopically. Meaning similar auditory tones are organised close together |
|
|
Which primary cortices are somatotopically organised? |
Sensory and Motor |
|
|
In the sensory and motor cortices, is the foot located medially or laterally? |
Medially. Within the longitudinal fissure |
|
|
Which hemisphere is usually dominant for handedness'? Is this any different for speech? |
As the majority of people are right handed, the left hemisphere is the dominant one for controlling the hand. The left hemisphere is even more dominant for speech but does not relate to handedness. E.g. right handed people can still be either left or right speech dominant and vice-versa |
|
|
What are the 3 layers of meninges? |
- Dura mater - Arachnoid mater - Pia mater |
|
|
What is the name of the meningeal layer that is tightly bound to the inner surface of the skull? |
Dura mater |
|
|
What is the name of the meningeal layer which adheres to the brain surface |
Pia mater |
|
|
What is the name of the structure descending in to the longitudinal fissure? What is the structure composed of? |
Falx cerebri. Is an extension of the dura mater |
|
|
How does the falx cerebri help protect the brain? |
This structure slows the rotation of the brain within the skull thus lessening any potential internal impact on the skull.
|
|
|
Name the meninges and meningeal spaces from inside to outside |
- brain - pia mater - subarachnoid space - arachnoid mater - subdural space - dura mater - epidural space - skull |
|
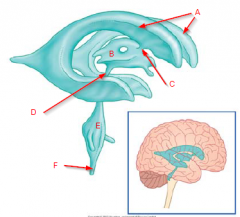
Label structures |
A - Lateral Ventricles B - 3rd ventricle C - Interventricular foramina D - Cerebral aqueduct E - 4th ventricle F - Central canal of SC |
|
|
Where is the 3rd ventricle located? |
Between the left and right thalamus |
|
|
Where is the 4th ventricle located? |
Between the Brainstem and Cerebellum |
|
|
What is the function of the interventricular foraminae? |
Join the lateral ventricles to the 3rd ventricle |
|
|
What is the function of the cerebral aqueduct? |
Joins 3rd and 4th ventricle |
|
|
Which meningeal space does the CSF occupy? |
Subarachnoid space |
|
|
How does CSF get in to the subarachnoid space? |
Through foramina in the 4th ventricle |
|
|
What is the name of the structure that produces cerebrospinal fluid? |
The choroid plexus. This is a structure that lines the ventricles. Ependymal cells produce the CSF |
|
|
How is CSF resorbed? |
CSF is returned to the venous system through arachnoid villi, which protrude in to the venous sinuses. |
|
|
Roughly how much CSF is in the CNS? How much is produced and resorbed daily? |
There is a rough volume of 150mL of CSF. We roughly produce and resorb 400-500mL daily. |
|
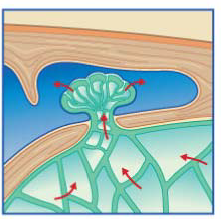
What is this structure? What is its purpose? |
Arachnoid villi. Returns CSF from the subarachnoid space to the venous system via venous sinuses. |
|
|
What are the two major blood vessels in the neck that supply the brain? |
- Vertebral arteries - Internal carotid arteries |
|
|
Which major arteries enter the skull through the foramen magnum? How are they formed |
The basilar artery. Formed by the left and right vertebral arteries joining. The internal carotid artery. Branches off the common carotid artery. |
|
|
What are the 3 cerebral arteries that supply the cerebrum? How are they formed? |
Anterior Cerebral artery - terminal division of internal carotid artery Middle Cerebral artery - terminal division of internal carotid artery Posterior cerebral artery - Basilar artery divides into R + L posterior cerebral arteries |
|
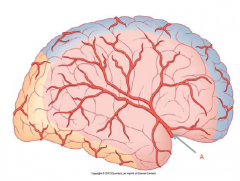
|
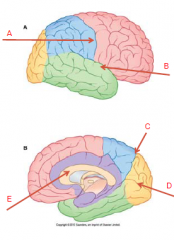
A - Middle cerebral artery |
|
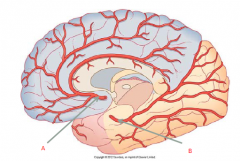
|
A - Anterior cerebral artery B - Posterior cerebral artery |
|
|
What is the blood-brain barrier? |
In the blood vessels of the brain, the endothlieal cells lining the capillaries form tight junctions to prevent the free passage of certain substances. |
|
|
What structure is responsible for the blood brain barrier? |
Astrocytes |
|
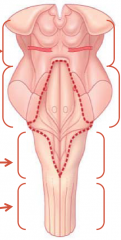
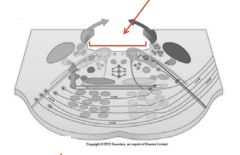
What structure does the dotted line indicate? |
4th ventricle |
|
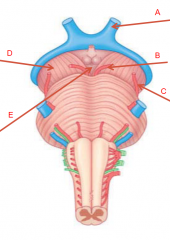
|
A - optic nerve (2) B - oculomotor (3) C - trochlear nerve (4) D - cerebral peduncles E - interpeduncular fossa |
|
|
Which part of the brainstem does the trigeminal nerve attach? |
Pons |
|
|
How are the fibres orienated in the pons? |
Transverse |
|
|
Where are the superior and inferior colliculi located on the brainstem? |
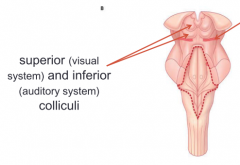
Dorsal surface of the midbrain |
|
|
What are some dorsal anatomical features of the Pons? |
|
|
|
What are some dorsal anatomical features of the Medulla? |
|
|
|
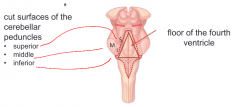
Where is the floor of the 4th ventricle? |
Dorsal surface of pons and medulla |
|
|
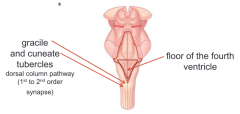
Where are the gracile and cuneate tubercles located? |
Dorsal surface of medulla |
|
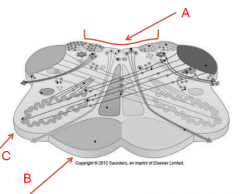
Which part of the brainstem is pictured here? Label A-C? |
Midbrain A - Cerebral aqueduct B - Interpeduncular fossa C - cerebral peduncle |
|
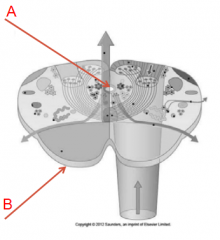
Which part of the brainstem is pictured here? Label A |
Pons A - 4th ventricle |
|
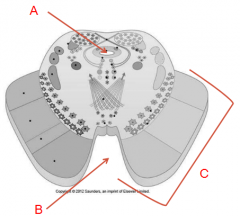
Which part of the brainstem is pictured here? Label A-C |
Open Medulla A - 4th ventricle B - Pyramid C - Olive |
|
|
What are 2 features unique to the open medulla that the closed medulla don't have? |
- olive - floor of 4th ventricle |
|
Which part of the brainstem is pictured here? Label A-B |
Closed medulla A - Central canal of spinal cord B - Pyramid |
|
|
How is the pons connected to the cerebellum? |
Cerebellar peduncles |
|
|
How is the midbrain connected to the cerebrum? |
cerebral peduncles |
|
|
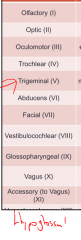
Name and number the 12 cranial nerves |
|
|
|
Which nerve supplies the muscles of mastication? |
Trigeminal 5 |
|
|
Which cranial nerves exit the midbrain? |
Oculomotor (3) and Trochlear (4) |
|
|
Which cranial nerves exit the pons? |
Trigeminal (pons) Abducens, Facial and Vestibulocochlear (pontomedullary junction) |
|
|
Which cranial nerves exit the brainstem at the medulla? |
- Glossopharyngeal (9) - Vagus (10) - Accessory (11) - Hypoglossal (12) |
|
|
What is the function of the superior colliculi of the midbrain? |
contributes to the visual system |
|
|
What is the function of the inferior colliculi of the midbrain? |
Contributes to the auditory system |
|
|
How many neurones in the cortico bulbar pathway? |
2 |
|
|
Which side of the body does the corticobulbar tract effect? |
Predominantly contralateral. However, muscles in the upper face have bilateral input |
|
|
If a patient has complete motor loss on one side of their face, where is the lesion? Would this be an UMN or LMN lesion and why? |
The lesion would be in the facial nerve (CN7). This would be a LMN lesion, as the entire face is effected. It was was an UMN lesion, muscles in the upper face would still have function as these have bilateral input and would therefore have input from UMN on the contralateral side |
|
|
What are the 3 divisions of the trigeminal nerve? |
- Opthalmic - Maxillary - Mandibular |
|
|
What is Bell's Palsy? |
a disorder of the facial nerve |
|
|
The 'eye follow' test is used for which cranial nerves? |
- Oculomotor (3) - Trochlear (4) - Abducens (6) |
|
|
What eye movement is the 'abducens' nerve responsible for? |
Direct lateral movement (abducens = abduct) |
|
|
What is the reticular formation? |
Neural network in the brainstem. Composed of most of the remaining tissue (not CN nuclei or long pathways) |
|
|
What is the reticular formation responsible for? |
- automatic and reflex activities - pattern generators (parallel eye movements, chewing, swallowing) - respiratory control - cardiovascular control - sleep cycles - pain perception |
|
|
What are the structures of the diencephalon? |
- epithalamus - subthalamus - hypothalamus - thalamus |
|
|
What tissue is the thalamus mostly composed of? (grey/white matter) |
Grey matter |
|
|
How are the thalamic nuclei organised |
Thalamic nuclei are ordered the same way as corresponding cortices. E.g. Visual nuclei is retinotopic, auditory is tonotopic, sensory is somatotopic |
|
|
What is the only sense not interpreted by the thalamus? |
Olfaction (smell) |
|
Label A-E on this diagram of the thalamus |
A - Ventroanterior B - Ventrolateral C - Ventroposterior D - Lateral geniculate E - Medial Geniculate |
|
|
Which thalamic nuclei are responsible for motor? |
Ventro-anterior and ventro-lateral |
|
|
What is the ventroposterior thalamic nucleus responsible for? |
General senses. Medial parts are responsible for the face, lateral parts are for everything else. |
|
|
Specifically, where are the cell bodies of 3rd order afferent neurones located?
|
Ventroposterior nucleus of the thalamus. |
|
|
What is the function of the medial geniculate nucleus of the thalamus? |
Auditory sense |
|
|
What is the function of the lateral geniculate nucleus of the thalamus? |
Visual sense |
|
|
What is the term used to describe receptive and expressive aphasia? |
Global aphasia |
|
|
What is the medical term used for swallowing difficulties? |
Dysphagia |
|
|
What is the difference between an ABI and a TBI? |
ABI is a broad term used to described any brain injury that is not congenital. The brain injury can be caused by any numerous factors. TBI is an injury to the brain resulting from an external mechanical force. |
|
|
ABI's are most common in which demographic? |
Young males (15-24) |
|
|
What is the second leading cause of death in Australia? |
Cerebrovascular disease. Second leading cause of death worldwide also |
|
|
What is cerebrovascular disease? |
CVD is a disease of the blood vessels supplying the brain |
|
|
What is the common name for a Cerebrovascular accident? (CVA) |
Stroke |
|
|
What is the term used to describe the death of neural tissue? |
Infarction |
|
|
What is a transient ischaemic attack (TIA)? |
A TIA is also known as a mini-stroke and is a temporary ischaemia caused by a temporary blockage of a cerebral blood vessel. The blockage clears before acute infarction occurs. |
|
|
How long does a TIA last? |
Less than 24 hours |
|
|
What are some non-modifiable risk factors for stroke? |
- family history - age (increased risk with age) - gender (men at more risk) |
|
|
What are some modifiable risk factors for stroke? |
- TIA - High BP - High cholesterol - smoking -obesity - poor diet - sedentary lifestyle - alcohol - heart disease - diabetes |
|
|
What are the two types of stroke and what is the difference? |
Ischaemic - caused by a blockage to a blood vessel Haemorrhagic - caused by bleeding in to brain tissue (e.g. ruptured vessels) |
|
|
Which type of stroke is most common? |
Ischaemic (approx 85% of all strokes) |
|
|
What are the causes of ischaemic stroke? |
Occlusion of an artery. Usually by - Thrombosis (Blood clot forming on artery wall) - Embolism (Blood clot breaking off and getting stuck in a distal artery) |
|
|
What is the ischaemic penumbra? |
A band of cells surrounding the ischaemic tissue. This tissue may also die but has minimal blood flow from other arteries so the chances of saving the penumbra are better. This area can be saved if circulation is restored in time. |
|
|
How are strokes classified? |
Oxford (Bamford) Classification, which is based on the clinical presentation. (TACI, PACI, LACI and POCI) |
|
|
What are the 2 main types of haemorrhagic stroke? What is the difference? |
Intracerebral - burst blood vessel causing bleed in to cerebrum. Is usually a focal blees Subarachnoid - bleeding in the subarachnoid space. Not as focal as an intracerebral haemorrhage |
|
|
What are the symptoms of stroke? |
Depends on the location in the cerebrum. It is highly variable |
|
|
What are the main causes of a TBI? |
- motor vehicle accidents - falls - assault |
|
|
How are TBI's classified? |
As open or closed. Open TBI has exposed brain tissue and closed does not. |
|
|
What is a coup/contrecoup injury of the brain? |
Coup/contrecoup refers to a particular TBI where the brain injury occurs on oppose sides of the skull as a result of the skull rebounding from one side to another. Coup injury is the initial impact. Contrecoup injury is the rebound injury |
|
|
What are the pathological consequences of a TBI? |
- Ischaemia - Haemorrhage - Increased ICP - Cebebral oedema - herniation |
|
|
What is normal intracranial pressure? |
0-15 mmHg |
|
|
What are some pathological results of increased intracranial pressure? |
- Altered levels of consciousness - Hypoxia and cell death - herniation of brain tissue |
|
|
What is the usual classification system for a TBI? |
Glasgow Coma Scale
|
|
|
What are the best and worst GCS scores for a TBI? |
3 is the worst possible GCS score. 15 is the best. |
|
|
A person has a head injury. They have a momentary loss of consciousness. They present with a headache, are disoriented, confused, irritable and suffering amnesia. Would this be classified as a mild, moderate or severe head injury? |
Mild |
|
|
A person has a head injury. They are unconscious for a short time. They also present with some neurological deficits including hemiparesis and aphasia. Would this be classified as a mild, moderate or severe head injury? |
Moderate |
|
|
A person has a head injury. They are in a coma and present with severe neurological deficits including hemiplegia and they require ventilation. Would this be classified as a mild, moderate or severe head injury? |
Severe |
|
|
What are 4 different types of intracranial haemorrhage that can result from a TBI? |
- Extradural - Subdural (can be acute and chronic) - Intracerebral - Subarachnoid |
|
|
What is a diffuse axonal injury (DAI)? |
A DAI is a result of brain moving back and forth within skull and causes microscopic damage to axons in the brain/brainstem. Characterised by an immediate loss of consciousness |
|
|
What are some factors that will influence the prognosis of a TBI? |
- Size of lesion - Location of injury - Time since injury - Age - PTA (post traumatic amnesia) - gender (worse for males) |
|
|
What is meningitis? |
An infection of the meninges |
|
|
What is encephalitis? |
An infection of the brain |
|
|
How does bacterial meningitis spread? |
Through CSF |
|
|
What tissues does bacterial meningitis effect and how does the infection enter the area? |
Pia mater and arachnoid mater. Can enter via skull fracture, middle ear or upper respiratory tract |
|
|
How is bacterial meningitis treated? |
Antibiotics |
|
|
What is encephalitis? |
Virus invades and destroys neurons, glia. Resulting in inflammation and enema.
Neurological effects depend on which area is effected |
|
|
What are some symptoms of bacterial meningitis? |
Fever, headache, neck stiffness, seizures, altered consciousness. May also cause hydrocephalus and cranial nerve palsy |
|
|
What is the effect of poliomyelitis? |
Attacks motor neurons of brain stem and spinal cord. Results in sudden weakness or paralysis in parts of the body, fever, vomiting, malaise. |