Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
57 Cards in this Set
- Front
- Back
|
Discuss Michaelis-Menten kinetics:
|

|
|
|
Discuss the Lineweaver-Burk plot:
|

|
|
|
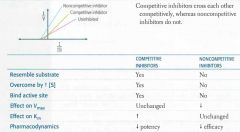
Discuss enzyme inhibition:
|
|
|
|
Overall summary of enzyme kinetics
|

|
|
|
What is bioavailability?
IV vs. oral-- |
Fraction of administered drug that reaches systemic circulation unchanged.
For an IV dose, F = 100%. Orally: F typically <100% to incomplete absorption and first-pass metabolism. |
|
|
Discuss volume of distribution:
what can alter Vd? |

|
|
|
Discuss half life:
|

|
|
|
Discuss drug clearance:
what can impair it? |

|
|
|
Discuss drug dosage calculations:
in renal and liver disease? |

|
|
|
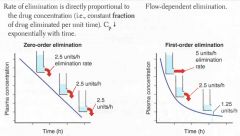
Discuss zero-order drug elimination:
|

|
|
|
Discuss first-order drug elimination:
|
|
|
|
Discuss urine pH and drug elimination:
weak acids-- weak bases-- |

|
|
|
Discuss phase I and phase II drug metabolism:
considerations in geriatric patients? |

|
|
|
What is efficacy?
What is potency? give examples of classes with high efficacy/potency |
Efficacy: Maximal effect a drug can produce. High-efficacy drug classes are analgesic (pain) medications, antibiotics, antihistamines, and decongestants. Partial agonists have less efficacy than full agonists.
Potency: Amount of drug needed for a given effect. Higher potency means higher affinity for receptor. Highly potent drug classes include chemotherapeutic (cancer) drugs, antihypertensive (blood pressure) drugs, and antilipid (cholesterol) drugs. |
|
|
Discuss receptor binding in the context of competitive agonists, noncompetitive agonists, and partial agonists:
|

|
|
|
What is the therapeutic index?
|

|
|
|
What is the therapeutic window?
|
Measure of clinical drug safety. Range of minimum effective close to minimum toxic dose.
|
|
|
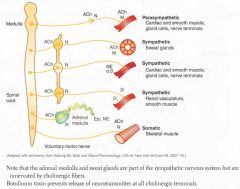
Diagram summary of CNS/PNS, with neurotransmitters and receptors:
|
|
|
|
Discuss kinds of ACh receptors:
|
Nicotinic ACh receptors are ligand-gated Na+/K+ channels; there are NN (found in autonomic ganglia) and NM (found in neuromuscular junction) subtypes.
Muscarinic ACh receptors are G-protein-coupled receptors that act through 2nd messengers; 5 subtypes: M1, M2, M3, M4, and M5. |
|
|
Discuss sympathetic G protein linked 2nd messengers:
receptor class-- g protein class-- major functions-- |

|
|
|
Discuss parasympathetic G protein linked 2nd messengers:
receptor class-- g protein class-- major functions-- |

|
|
|
Discuss dopamine receptors:
receptor class-- g protein class-- major functions-- |

|
|
|
Discuss histamine receptors:
receptor class-- g protein class-- major functions-- |

|
|
|
Discuss vasopressin receptors:
receptor class-- g protein class-- major functions-- |

|
|
|
Crazy yet effective mnemonic for remembering g-protein classes associated with different receptors:
|

"Qiss (kiss) and qiq (kick) till you're siq (sick) of sqs (super qinky sex)."
|
|
|
Summary of autonomic actions leading to smooth muscle contraction:
Summary of actions leading to cardiac/striated muscle contraction: |

|
|
|
Diagram of actions of autonomic drugs:
cholinergic-- adrenergic-- |

|
|
|
Diagram of a Noradrenergic nerve terminal:
|

|
|
|
Cholinomimetic agents:
List 4 direct agonists: and their clinical applications: and their actions: |

|
|
|
Cholinomimetic agents:
List 5 Indirect agonists (anticholinesterases): and their clinical applications: and their actions: |

|
|
|
Discuss Cholinesterase inhibitor poisoning:
|
Often due to organophosphates, such as parathion, that irreversibly inhibit AChE.
Causes Diarrhea, Urination, Miosis, Bronchospasm, Bradycardia, Excitation of skeletal muscle and CNS, Lacrimation, Sweating, and Salivation. Antidote: atropine + pralidoxime (regenerates active AChE). *DUMBBELSS. Organophosphates are components of insecticides; poisoning usually seen in farmers. |
|
|
List muscarinic antagonists:
and the organ systems they affect: and their clinical applications: |

|
|
|
Discuss atropine:
Its effects on various organ systems: And its toxicity/side effects: |

|
|
|
List some Direct sympathomimetics:
Their effects on a1, a2, ß1, ß2, and D1 receptors: Their clinical applications: |

|
|
|
List some Indirect sympathomimetics:
Their effects on a1, a2, ß1, ß2, and D1 receptors: Their clinical applications: |

|
|
|
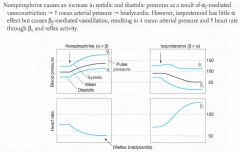
Discuss norepinephrine vs. isoproterenol:
|
|
|
|
List and describe 2 Sympathoplegics:
|

|
|
|
List and discuss applications and toxicity of nonselective, a1 selective, and a2 selective alpha blockers:
|

|
|
|
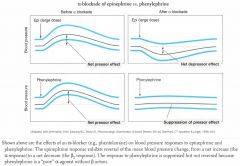
Discuss alpha blockade of epinephrine vs. phenylephrine:
|
|
|
|
ß-blockers:
list 9-- list applications and effects-- toxicity-- selectivity-- |

|
|
|
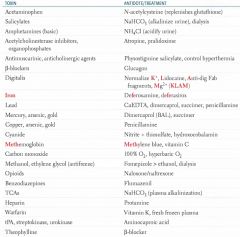
Specific antidotes:
list toxins and their antidotes/treatments: |
|
|
|
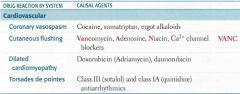
List 4 cardiovascular drug reactions:
and causal agents for each-- |
|
|
|
List 7 hematologic drug reactions:
and causal agents for each-- |

|
|
|
List 2 respiratory drug reactions:
and causal agents for each-- |

|
|
|
List 4 GI drug reactions:
and causal agents for each-- |

|
|
|
List 5 reproductive/endocrine drug reactions:
and causal agents for each-- |

|
|
|
List 10 MS/Cx Tissue drug reactions:
and causal agents for each-- |

|
|
|
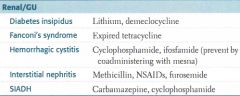
List 5 renal/GU drug reactions:
and causal agents for each-- |
|
|
|
List 4 neurologic cardiovascular drug reactions:
and causal agents for each-- |

|
|
|
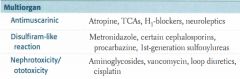
List 3 multiorgan drug reactions:
and causal agents for each-- |
|
|
|
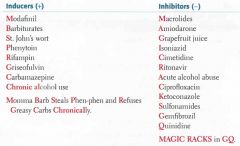
List P-450 Inducers (8) and Inhibitors (12):
|
|
|
|
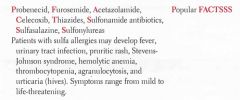
List (8) and discuss sulfa drugs:
|
|
|
|
Drug categories by ending:
antimicrobials-- |

|
|
|
Drug categories by ending:
CNS drugs-- |

|
|
|
Drug categories by ending:
autonomic drugs-- |

|
|
|
Drug categories by ending:
cardiovascular drugs-- |

|
|
|
Drug categories by ending:
other-- |

|