![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
91 Cards in this Set
- Front
- Back
|
Ethosuximide |
Used for absence seizures(good efficacy and safety) Not good for partial seizures. MOA(possibly Ca++ channels) Toxicity: GI(pain & N/V), Lethargy, HA, hiccup, euphoria. Only syrup available(as known) |
|
|
Depakene(valproic acid) Depakote(Sodium valproate) |
For absence seizures, some myoclonic seizures, generalized tonic clonic, bipolar, migraine prophalaxis. (broad spectrum AED) Displaces phenytoin from proteins. Inhibits metabolism for phenobarbital, phenytoin, carbamazepine via CYP450. Toxicity: GI (pain, N/V, heartburn), sedation (more with phenobarbital), fine tremor |
|
|
What is the difference between depakene and depakote? |
Depakote has less GI upset. |
|
|
Benzodiazepines |
psychoactive drug that depresses all lvls of the CNS. (possibly by increasing GABA) Very good for seizures. |
|
|
Diazepam(Valium) |
IV/PR very effective in stopping continuous seizure activity. Bad for chronic therapy |
|
|
Lorazepam (Ativan) |
IV better for status epilepticus than diazepam. |
|
|
Clonazepam (Klonipin) |
Long-acting drug with efficacy against absence seizures. Some effectiveness in myoclonic seizures. Only in the oral form. |
|
|
How do we handle infantile spasms? |
It's mostly palliative. The corticotropins can be given IM. Prednisone can be given. Vigabatrin(GABA analog) |
|
|
How do we diagnose a pt with epilepsy? |
Hx: eyewitnessed Physical/neuro exam EEG CT scan MRI Special studies: Ictal spect, PET, video EEG monitoring. |
|
|
What are some treatments for epilepsy? |
Drugs Surgery Vagus nerve stimulation Ketogenic diet |
|
|
What drugs are good for tonic-clonic seizures? |
Carbazepine, phenytoin, phenobarbital, and broad spectrums |
|
|
What drugs are good for absence seizures? |
Ethosuximide and broad spectrum |
|
|
What are broad spectrum AED? |
Valproic acid and clonazepam |
|
|
What are some adjunct AED? |
Lamotrigine and gabapentin |
|
|
What is status epilepticus? |
most common form of generalized tonic-clonic Life-threatening emergency that requires immediate management. Almost always requires anti-seizure medication. Can give fosphenytoin(need more) LD:15-20 mg/Kg. for those inresponsive to fosphenytoin, give large dose of 20 mg/Kg of phenobarbital. |
|
|
What is a good pathway for monitoring and treating seizures? |
Not witnessed > give benzo > repeated > Benzo > repeat > fosphenytoin/phenobarbital > intubate and ventilate Witnessed wait 5 min before starting this pathway |
|
|
How often does the 1st drug work in seizures? |
47% |
|
|
How often does the 2nd drug work in seizures? |
13% |
|
|
How many need to look into surgical interventions and other therapies? |
40% |
|
|
What do we need to look at in pts on anti seizure meds before the OR? |
look at how we can maintain the drug lvls during the surgery |
|
|
What are things to look at when you are giving a neuromuscular blockade on a patient taking phenytoin? |
Those using phenytoin chronically are more resistant to neuromuscular blockade. Those just starting the use of phenytoin will have an enhanced neuromuscular blockade. |
|
|
What drug stimulate seizure activity? |
methohexital, sevoflurane |
|
|
What narcotic can stimulate seizures? |
demerol |
|
|
How do craniotomies help epilepsy? |
take out the reactive portion. Anti-seizure meds are reduced or withdrawn to see the seizure, so can't have deep sedation or surgeon can't spot seizure. |
|
|
What is hemostasis? Is it normal? |
stopping of blood flow. It is normal when DPS occurs to the blood vessel. |
|
|
What breaks down clots? |
Plasmin |
|
|
What can happen is vasoconstriction and formation of platelet plugs occurs in a blood vessel? |
It can completely occlude the vessel. |
|
|
What are the phases of platelets? |
Adhesion aggregation secretion of pro-clotting factors Cross linking of adjacent platelets |
|
|
What happens in clotting? |
Injury > vWF binds to GP1b and collagen binds to GP1a > release of TXA2, ADP, and 5-HT > activate next platelet to degranulate > activates the coagulation cascade > Prothrombin > thrombin > changes fibrinogen to fibrin > connects platelets at the GP IIb/IIIa. |
|
|
Where is collagen? |
Just under the endothelial cells |
|
|
Where does aspirin work? |
TXA2 |
|
|
What makes fibrinogin? |
Liver |
|
|
What is PGI2 and where does it come from? |
It inhibits platelet aggregation and it comes from the endothelial cell. |
|
|
Thrombogenisis |
clots forming around platelets |
|
|
What changes prothrombin to thrombin? |
Factor X |
|
|
How does the extrinsic factor work? |
Trauma activates Factor VII > activates factor X > Prothrombin to thrombin > Fibrinogen to fibrin > facor XIII makes it into cross linked fibrin clot |
|
|
How does intrinsic factor work? |
DPS surface activates XII > Activate XI > Activate IX > Factor VIII(Activated by thrombin) + Factor IX activate factor X > Prothrombin to thrombin > Fibrinogen to fibrin > facor XIII makes it into cross linked fibrin clot |
|
|
What inhibits the extrinsic pathway? |
TFPI (Tissue factor pathway Inhibitor) -keeps VII from being activated |
|
|
What inhibits both pathways? |
Antithrombin |
|
|
What inhibits the intrinsic pathway? |
Protein C, which is activated by protein S and thrombin, inactivates V and VIII |
|
|
What is the most common type of hemophilia? |
Factor VIII
intrinsic pathway can be activated without factor VIII, but it will not be as stable or long lasting. |
|
|
What does thrombin activate? |
V VIII XI XIII Protein C |
|
|
DVT |
usually form in the lower limbs, potentially life threatening. The common factors are called Virchow's Triad -Stasis -Endothelial injury -Hypercoagulability |
|
|
What are risk factors for DVT? |
Inherited -Antithrombin III deficiency -Protein C deficiency -Protein S deficiency -Sickle Cell Anemia -Activated Protein C resistance Aquired -Bedridden -Sx/trauma -Obesity -Estrogen use -Malignancies -Chronic Venous insufficiency |
|
|
Disseminated Intravenous Coagulation (DIC) |
Blood clots are occurring all over the body. The coagulation factors and platelets are all used up in the making of these clots, so spontaneous bleeding occurs. Is more treatable. Cause: massive tissue injury, malignancy, sepsis, abruptio placentae. Treatment: plasma transfusions, treat underlying cause, 10-50% mortality rate |
|
|
Thombotic Thrombocytopenic Purpura (TTP) |
Tiny clots developing all over the body that get into your capillaries. This is caused by ADAMST13 deficiency. |
|
|
Heparin Induced Thrombocytopenia (HIT) |
Immune reaction caused by heparin where the antibodies try to attack heparin. drops platelets D/C heparin and give protamine |
|
|
What are the two major systems to regulate coagulation? |
Fibrin inhibition -keep clots from forming Fibrinolysis -To break down clots after |
|
|
What are some protease inhibitors? |
alpha1-antiprotease alpha2-macroglobulin alpha-antiplasmin antithrombin |
|
|
How does the fibrolynic system work? |
Converts the inactive plasminogen to plasmin. Plasmin remodels and breaks down clots. Limits the extension of the thrombus. Plasmin is released from injured cells. |
|
|
What medications can we use to break up clots? |
Tissue plasminogen activator(t-PA) Urokinase Streptokinase(these all promote production of plasmin) |
|
|
What can we use for hemophelia? |
Aminocaproic acid It protects clots from lysis |
|
|
What is the plasmin cascade? |
plasminogen activated by t-PA/urokinase/streptokinase to become plasminogen. Thrombin breaks down Fibrin and fibrinogen |
|
|
What is streptokinase? |
It is a bacteria that activates plasminogen |
|
|
What are the different types of coagulation modifier drugs? |
Anticoagulants Antiplatelets Thrombolytic drugs Hemostatic or antifibrinolytic drugs |
|
|
Warfarin |
oral anticoagulant that decreases the synthesis of clotting factors by inhibiting Vitamin K. This is to prevent DVT. |
|
|
Heparin |
Parental anticoagulant that inactivates clotting factors to prevent DVT. Large molecule, so it has a lot of toxicities, but it stabalizes ATIII. Need the higher molecular weight to affect the clotting cascade. |
|
|
Aspirin |
Antiplatelet drug that decreases the platelet aggregation to prevent arterial thrombosis. |
|
|
Streptokinase |
Thrombolytic drugs |
|
|
Fondaparinux(Atrixtra) |
Pentasaccharide peptide sequence of heparin that binds to ATIII. Fewer SE, but not as effective. Synthetic and selective for factor X. There are less bleeding risks, so useful for HIT. |
|
|
What is the MOA of heparin? |
binds and activates antithrombin III and enhances activity by 1000x and can catalyze reaction w/o being consumed. |
|
|
What does unfractionated mean? |
Many different weights of heparin from 5,000-30,000. These are extracted from porcine intestinal mucosa and bovine lung |
|
|
Enoxaparin (Lovenox) |
LMW heparin that's less specific for factor Xa, so less on thrombin. |
|
|
What are some Heparin toxicities? |
Bleeding: Monitor aPTT, LMW have more predictable plasma lvls, elderly women and pts with renal failure are more prone to hemorrhage. Transient thrombocytopenia from HIT(antibodies are around for 100 days) |
|
|
Prthrombin time (PT) |
How long in seconds does it take for the blood to clot. This assesses the function of the extrinsic system and the common pathway of the coagulation cascade. They add factor III(Timing isn't consistent from lab to lab because they use different factors.) |
|
|
International Normalized Ratio (INR) |
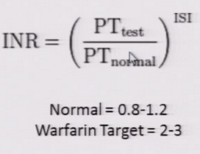
What is reported because it is more accurate due to factoring in the different sources of factor III. |
|
|
activate Partial Thromboplastin Time (aPTT) |
Measures the intrinsic pathway and common pathway. Phospholipid is added to induce the pathway. Normal-35-45 seconds |
|
|
What do you do for a pt on heparin that has an elevated PT and aPTT? |
d/c heparin protamine sulfate -binds to heparin due to strong + charge -excess is also an anti-coagulant -less effect on LMW -NO effect on fondaparinux |
|
|
What are contraindications for heparin? |
Active bleeding, hemophilia, thrombocytopenia, severe HTN, intercranial hemmorhage, infective endocarditis, Active TB, GI ulcers, advanced hepatic disease |
|
|
Hirudin (Lepirudin - recombinant) |
Binds to both active and substrate recognition. Isolated from leeches and helps with micro-vascular sx. |
|
|
How was warfarin discovered? |
Stored sweet clover acted on by fungus was causing cattle hemorrhagic disease. Discovered by the University of Wisconsin. |
|
|
What is one of the most commonly subscribed drugs that also happen to have a lot of related bleeding disorders and deaths? |
Warfarin |
|
|
What are the pharmacokinetics of warfarin? |
100% oral availability 99% protein binding, giving it high 1/2 life=36 hrs |
|
|
What is the MOA for warfarin? |
Blocks the gamma-carboxylation of several glutamate residues.(block Vit K pathways) Protein C and S are modified through this pathway. |
|
|
When you start a pt on warfarin what should you consider? |
start low, go slow because it only inhibit s protein C 1st, which makes it a procoagulant for the 1st 8-12 hours. This can cause Cutaneus necrosis form the little clots. |
|
|
Is warfarin safe for pregnancy? |
cause birth defects and hemorrhagic disorder in the fetus |
|
|
What is the therapeutic range for warfarin? What is normal? |
INR Normal: 0.8-1.2 INR on med: 2-3 Reduce the prothrombin time to 25% of normal Need to reduce/dc at 20% or less |
|
|
How would you reverse warfarin? |
Stop the drug Give large dose of Vitamin K FFP Factor IX concentrates |
|
|
What if you have a problem and can't use warfarin? |
There are new therapies that are antibody based, which make them more expensive. |
|
|
What are fibrinolytics? |
Llyse thrombi and catalyze the formation of serine protease plasmin. |
|
|
What makes streptokinase? |
Streptococci |
|
|
What makes urokinase? |
Kidney, lyses the thrombi from within |
|
|
Tissue plasminogen factors (tPA) |
Recombinant(altepase) activates plasminogen that is bound to fibrin -this confines the fibrinolysis to formed thrombus -avoids systemic activation |
|
|
Aspirin |
anti platelet, which affect TXA2 and changes the platelet's shape, granule release, and aggregation. |
|
|
Clopidogrel(plavix) and Ticlopidine(Ticlid) |
Anti platelet that block receptor sites on platelets to reduce platelet aggregation. MOA: irreverably inhibit ADP on platelets. NO effect on prostaglandin metabolism 8.7% reduction of ischemic events from aspirin SE: Nausea, dyspepsia, diarrhea, hemorrhage, leukopenia, TTP |
|
|
IIb/IIIa Receptor Blockers |
anti platelet that blocks platelets from hooking up with each other. Abciximab-monoclonal antibody |
|
|
Vitamin K |
fat soluble in green leafy vegetables and gut bacteria. Helps make Prothrombin and factors VII, IX, and X. |
|
|
Plasma fractions |
Help with plasma coagulation factor deficiencies. You can have concentrated and give specific types based on the deficiency. |
|
|
Desmopressin Acetate |
Increases factor VII activity for mild hemophilia and von willebrand disease. It increase the activeity of the intrinsic pathway. |
|
|
Aminocaproic acid |
Competitively inhibits plasminogen activation Used for adjunctive hemophilia therapy, bleeding from fibrolynic therapy, intracranial aneurysms, and postsurgical bleeding |
|
|
Aprotinin |
Inhibits: fibrinolysis by free plasmin 50% reduction in bleeding in certain sx like open heart and liver. |